In a Danish study of 558 patients with a brain abscess, those that had early surgical drainage did better than those treated conservatively with antibiotics only. Prompt neurosurgical consultation is warranted for these patients.
Despite ongoing attacks against the principles of DEI, most medical organizations know and have acknowledged the necessary role of creating a more diverse, equitable and inclusive environment. Doing so requires both a bottom up and a top down approach, with engaged leadership supporting active efforts to increase diversity
This author, published just this month in Annals, details a unique and exciting way to engage resident leadership in the DEI efforts of an emergency department, with the creation of a Chief Resident for DEI role. They detail the creation of the role, and describe some of the roles and responsibilities and thoughfully discuss some of the limitations. It's an exciting and thought provoking read.
Intranasal (IN) midazolam is often used for anxiolysis in pediatrics prior to procedures. In this study, 0.2 mg/kg of IN midazolam (up to 6 mg total dose) was given prior to laceration repair in children 2-10 years.
90% of children were at least minimally sedated at the start of the procedure and these children also displayed less anxiety when measured on a standardized anxiety scale.
Children's whose procedure started 10-20 minutes after IN medication compared to 25-35 minutes had significantly lower anxiety.
IN midazolam can be successful as an anxiolytic, but careful attention should be directed at the timing of the procedure.
GCS was first introduced in 1974 and now includes a preverbal version for patients < 2 years.
This study looked for non inferiority between motor Glascow Coma Scale (mGCS) and the total GCS in pediatric patients. The study also examined if a mGCS<6 was non inferior to a GCS < 14 in children. 582 patients < 18 years were reviewed in this retrospective review.
The mGCS was noninferior to total GCS as a triage tool in pediatric trauma. It also validated the use of mGCS <6 in place of GCS <14 in the field with identification of children at risk of death or requiring ICU care.
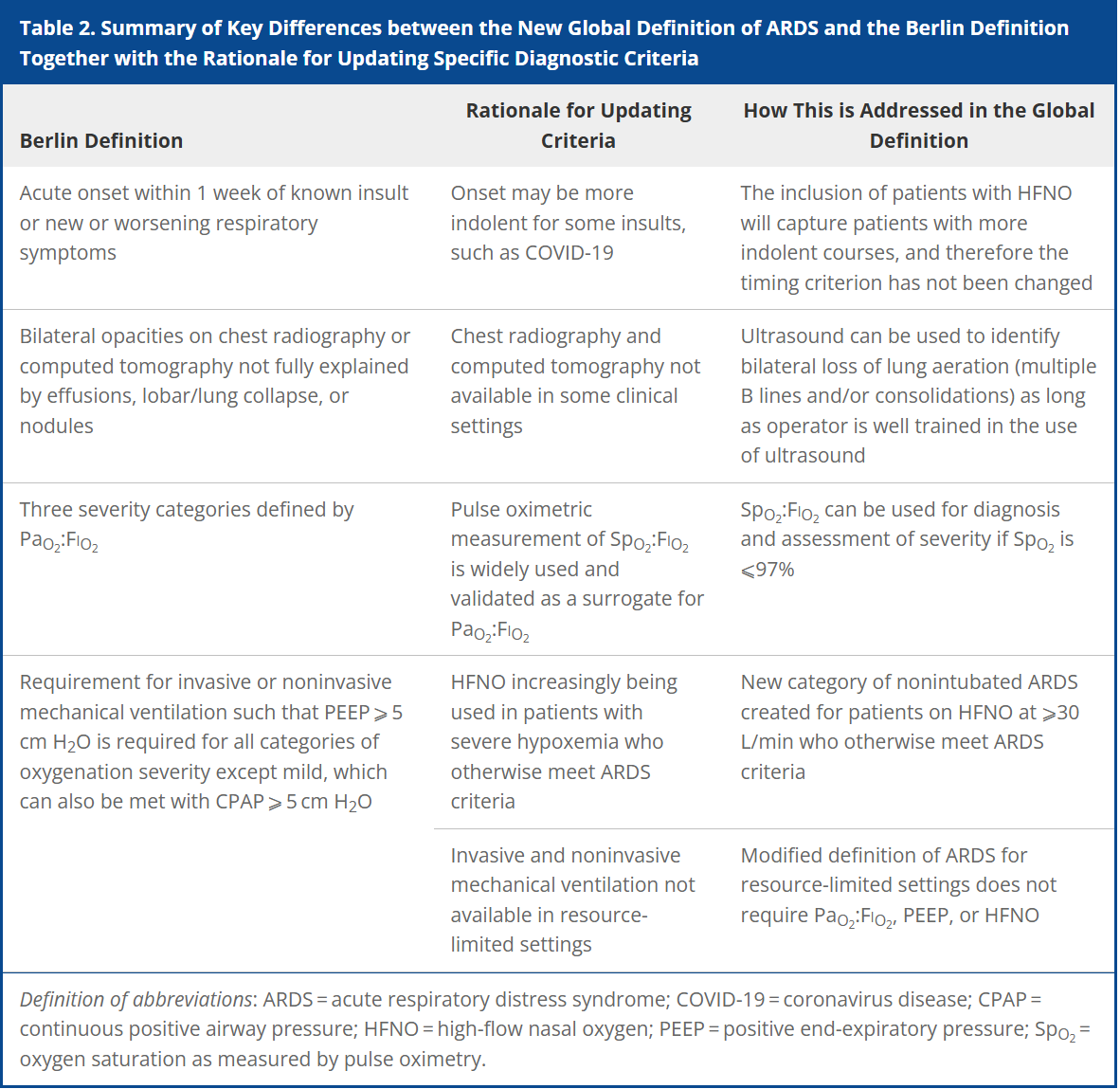
Acute respiratory distress syndrome (ARDS) is an acute, inflammatory lung injury that effects the lung diffusely and can be triggered by various insults. Aside from the Kigali modification, the most recent updated definition of ARDS was the Berlin definition in 2012. There have been many advances and changes in the understanding and clinical practice for managing patients with ARDS since then. In 2024, Matthay, et al. proposed the new global definition to build upon the Berlin criteria [1]. They addressed several important issues with the Berlin definition to improve the diagnostic criteria and improve ability for diagnosis in resource-limited settings.
ARDS Berlin Definition
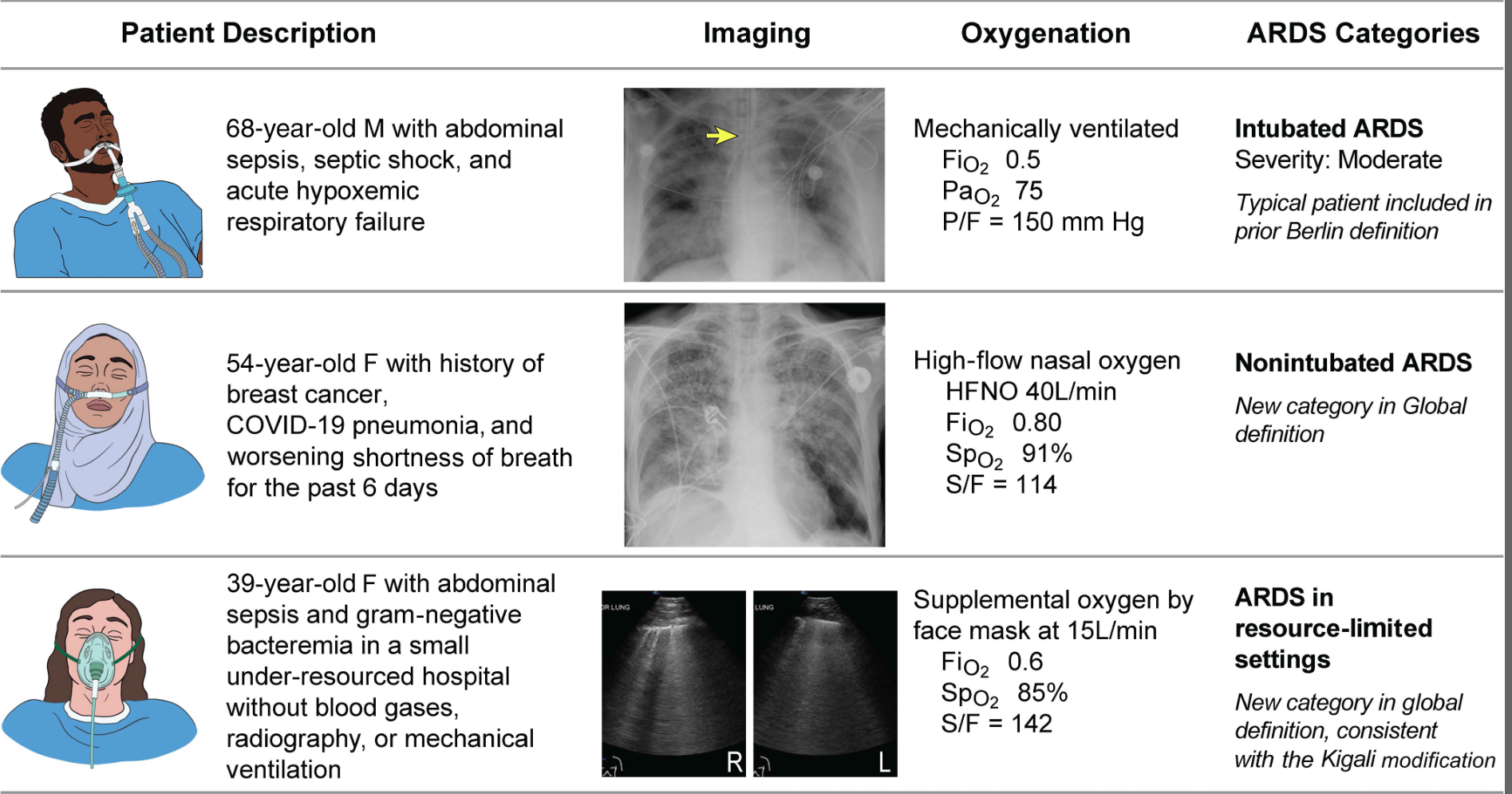
Important updates for the Global definition of ARDS
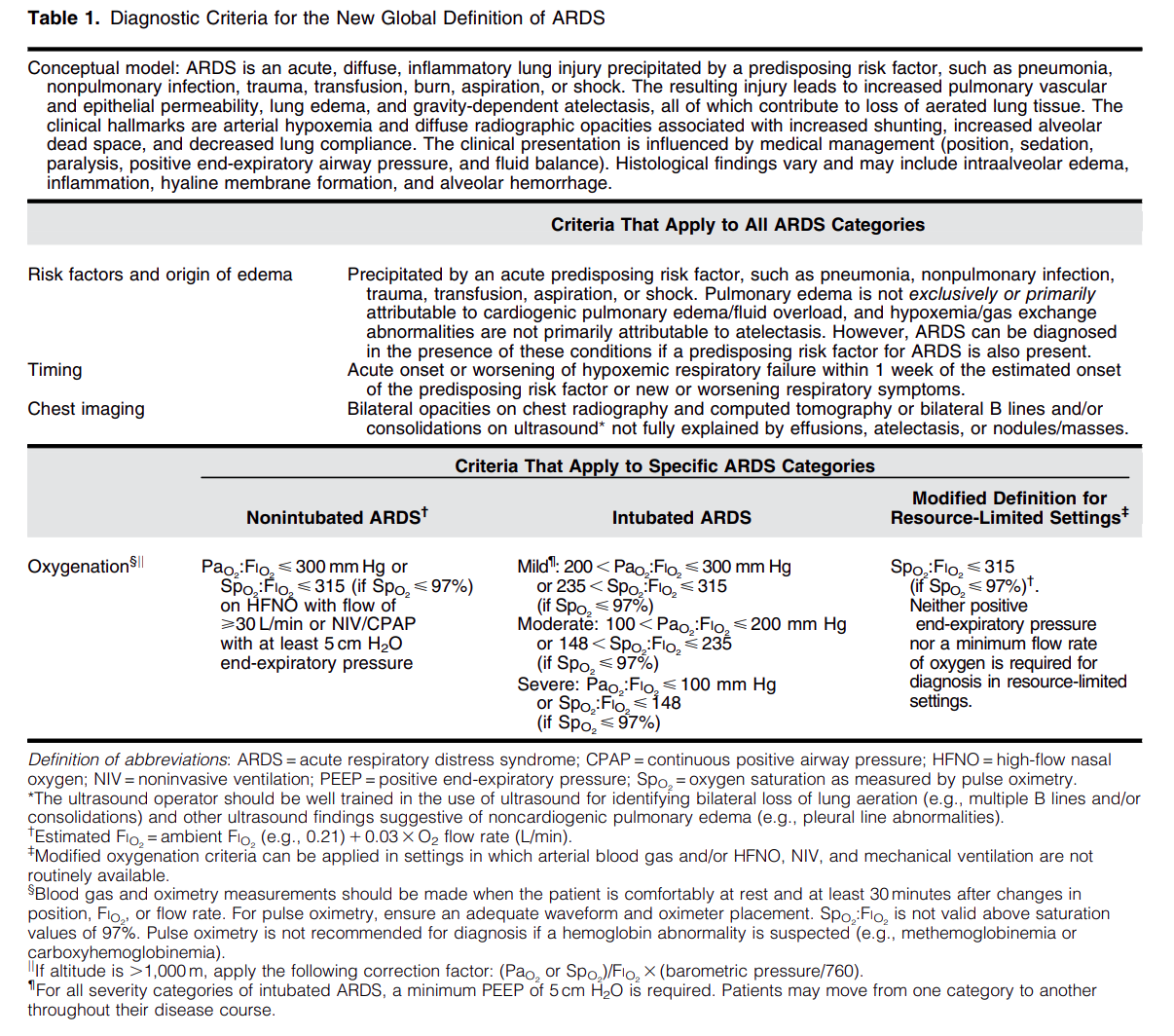
Diagnostic Criteria for the New Global Definition of ARDS from Matthay et al.
The Global Definition of ARDS expands upon the Berlin definition. It was shown that this new definition improves diagnosis in resource-limited settings, allows for earlier detection, and better classification [2]. A retrospective study evaluating this new global definition found that there was a significant number of patients identified using this new definition who would have been missed using the Berlin definition [3]. These patients may benefit from ARDS directed therapies and further prospective studies will be needed to assess how this new definition effects clinical management of these patients using the new definition.
A hip effusion can cause pain with leg movement in both pediatric and adult patients.
A recent multicenter, prospective study assessed the diagnostic accuracy of POCUS performed by pediatric emergency physicians in detecting hip effusion.
They found that POCUS had a sensitivity of 89.3% (95% CI 80.6 to 95.0%) and specificity of 99.2% (95% CI 97.0 to 99.9%).
To scan the hip:
-Position the patient supine with the patient’s hip externally rotated.
-Place the probe transversely across the patient’s leg with the marker towards the patient’s right and scan proximally.
-Upon reaching the proximal femur, rotate the probe marker so it points towards the patient’s umbilicus.
-Look for an anechoic stripe at the femoral neck, preceding the femoral head.
An anechoic stripe measuring at least 5 mm in the anterior synovial space or an asymmetry exceeding 2 mm compared to the opposite, asymptomatic hip is diagnostic for hip effusion in BOTH pediatric and adult populations.
In this Israeli study comparing mortality for trauma patients intubated in the emergency department vs the operating room, in hospital mortality was higher for the ED group before controlling for injury severity score and shock. After controlling for injury severity and shock, there was no difference in In hospital mortality. Coupled with previous research, if intubation can wait until after resuscitation and in the OR, that is ideal. And sometimes it just has to happen in the ED and we should be prepared for rapid resuscitation.
NSAIDs are first line analgesic medications for many pain related ED presentations
All NSAIDs are not created equal in their side effect profile
Ibuprofen and ketorolac are both commonly used NSAIDs in the ED
A 2010 review looked at relative risk estimates of individual NSAIDs and associated upper GI bleeding/perforation.
Definitions: Most of included studies included patients with NSAID use within prior week and daignosed upper GI bleed admitted to the hospital.
Daily use predicted increased risk.
In comparison between these two common medications Ibuprofen and Ketorolac: RR as follows
Ibuprofen (2.69 [95% CI 2.17-3.33]) vs ketorolac (14.54 [95% CI 5.87-36.04])
Ketorolac has approximately double the half life of ibuprofen
Other commonly used ED medications were also included:
RRs:
Naproxen 5.63 (95% CI 3.83-8.28)
Indomethacin 5.40 (95% CI 4.16-7.00)
Meloxicam 4.15 (95% CI 2.59-6.64)
Diclofenac 3.98 (95% CI 3.36-4.72)
Conclusion: The risk of upper GI bleeding varies between individual NSAIDs at the doses commonly used in the general population. When possible, consider the relative risk of a particular NSAID when making a selection.
As the weather warms up, remember that pediatric patients have some physiologic factors that increase their risk of heat related complications. Approximately 37 infants die in cars annually, with risk of vehicular related heat illness starting with outdoor temperatures as low 72°F (32°C). Approximately 9,000 high school athletes require treatment for heat related illness annually with approximately 2 deaths per year.
Physiology:
Infants and young children have physiologically limited thermoregulation. They also may lack developmental abilities to impact their environment (they cannot ask for water, remove clothing or a seat belt, or move themselves to a cooler environment).
Older children take longer to acclimate to environments than their adult counterparts- requiring 10-14 days to adjust to work outs in higher temperatures (a gradual approach of increasing gear over time has been recommended for outdoor sports requiring padding or heavy equipment)
Management:
Heat exhaustion/stroke- focus on cooling the patient with temperatures being monitored with a core measurement. In teens and older children this can be done in a similar manner to adults- with removal of clothes, emersion therapy for heat stroke. In infants and young children, some experts favor evaporative management over emersion due to reflex bradycardia as well as patient compliance.
There are no recommended medications for use during heat stroke. Benzodiazepines may be utilized to present shivering or to treat seizures only if needed.
Prevention:
For athletes steps should include encouraging hydration (flavored drinks have been shown to increase consumption and improve hydration), developing strategies for acclimatization for athletes, and have materials present (ice baths) to intervene quickly for players with symptoms. For infants and young children car alarms or reminders, and practicing placing a needed item in the back seat can prevent parents from inadvertently leaving a child in a car.
Background:
Early antibiotic administration is consistently linked to improved mortality outcomes in patients with sepsis. As a result, time-to-antibiotic delivery is a critical metric in hospital sepsis quality improvement initiatives. Empiric treatment often consists of a broad-spectrum beta-lactam to cover both gram-positive and gram-negative organisms, alongside vancomycin to ensure coverage of methicillin-resistant Staphylococcus aureus (MRSA). When multiple agents are indicated, they may be given simultaneously; however, factors such as limited intravenous (IV) access or drug incompatibilities can necessitate sequential administration. Administration of vancomycin first may delay the administration of a beta-lactam agent by at least 60-120 minutes due to its prolonged infusion time. This raises an important clinical question: Does the order in which antibiotics are administered influence outcomes in sepsis?
A 2022 retrospective study by Amoah et al. found that, among patients with confirmed bloodstream infections, a beta-lactam-first regimen was associated with a 52% reduction in the odds of short-term mortality compared to a vancomycin-first regimen. However, the generalizability of these findings to the broader population of patients with suspected sepsis, of whom only 15-20% ultimately have positive blood cultures, remains uncertain.
What's new?
A recent retrospective, multi-center, cohort study by Kondo et al. evaluated the impact of a beta-lactam-first antibiotic strategy compared to a vancomycin-first strategy on in-hospital mortality in patients with suspected sepsis. Of the 25,391 patients with sepsis who were screened, 21,449 (84.4%) received a beta-lactam first and 3,942 (15.6%) received vancomycin first. Patients who received vancomycin first had lower comorbidity burden, lower illness severity, more skin/musculoskeletal infections, and received beta lactams a median of 3.5 hours later relative to ED arrival compared to those who received a beta-lactam first. Although the overall rate of documented bloodstream infections was similar between groups, MRSA-positive cultures were more common in the vancomycin-first group, both in clinical cultures (4.5% vs. 3.2%) and in blood cultures (1.8 vs. 1.2%).
Beta-lactam administration prior to vancomycin was associated with an 11% reduction in the odds of in-hospital mortality (aOR: 0.89; 95% CI: 0.8-0.99; p=0.046). When the time-to-first antibiotic covariate was replaced with time-to-first beta-lactam, this association was no longer significant (aOR 0.93, 95% CI: 0.82-1.05, p=0.25), suggesting a possible link between time-to-first beta-lactam antibiotic and mortality. There was a trend toward lower in-hospital morality for the beta-lactam first regimen in several subgroups examined, including patients with positive blood cultures or positive MRSA cultures, and patients who received anti-pseudomonal beta-lactams; however, none reached statistical significance.
Bottom line:
Given the observed mortality benefit and absence of harm associated with a beta-lactam-first approach, even among patients with positive MRSA cultures, the findings of this study support the prioritization of beta-lactam therapy in patients with sepsis.
Pulse Checks in Cardiac Arrest: Your Fingers Are Not Reliable.
Summary: Whenever possible, use an ultrasound or an arterial line for pulse checks. Our fingers are not reliable.
Key points:
Multiple studies have demonstrated that manual pulse checks are not a reliable method to determine ROSC. Arterial lines and ultrasound are far more reliable methods. However, using more accurate measures of circulation lead to an additional dilemma: at what MAP, SBP, or ultrasound measured flow should we stop chest compressions? There is no agreed upon number, and as with most dilemmas in clinical medicine, the best answer is, “it depends”. However, a MAP > 50 or SBP > 60 for most patients is a reasonable choice to stop chest compressions. MAP < 50 or SBP < 60 are unlikely to provide adequate perfusion to the brain, and chest compressions should be resumed.
References:
Everyone clenches up when an imminent delivery shows up at the ED bay doors, even though most of these deliveries will not need intervention. Still, there are catastrophic ways delivery can go wrong, so today, let's talk about a new study on breech delivery.
The Study: Bogner et. al conducted a prospective single-center observational cohort study from 2006-2021 looking at breech deliveries in ~230 patients, with 92 of them being delivered in the traditional, supine way, while 140 of them delivered on all-fours. The only difference found between the two groups was that the all-fours group had heavier babies with bigger heads.
The Results: Over half (51.4%) of the patients in the all-fours position required no additional interventions from the provider compared to 11.9% of the supine group, and there were fewer perineal injuries. There was no increase in neonatal outcomes or NICU referrals in the all-fours group as compared to the supine group.
Limitations: Single center, no randomization, 11 patients started in all-fours and then had to switch to supine due to difficulty with delivery and prolonged second stage of labor, excluded footling breech
Takeaways: All-fours may be a position to consider for your patient with a breech delivery - especially if you haven't brushed up on your breech maneuvers recently.
Another case series of 3 resuscitative hysterotomies, all performed by obstetricians, reported 33% maternal and 67% neonate survival.(1).
The mechanics of the procedure are:
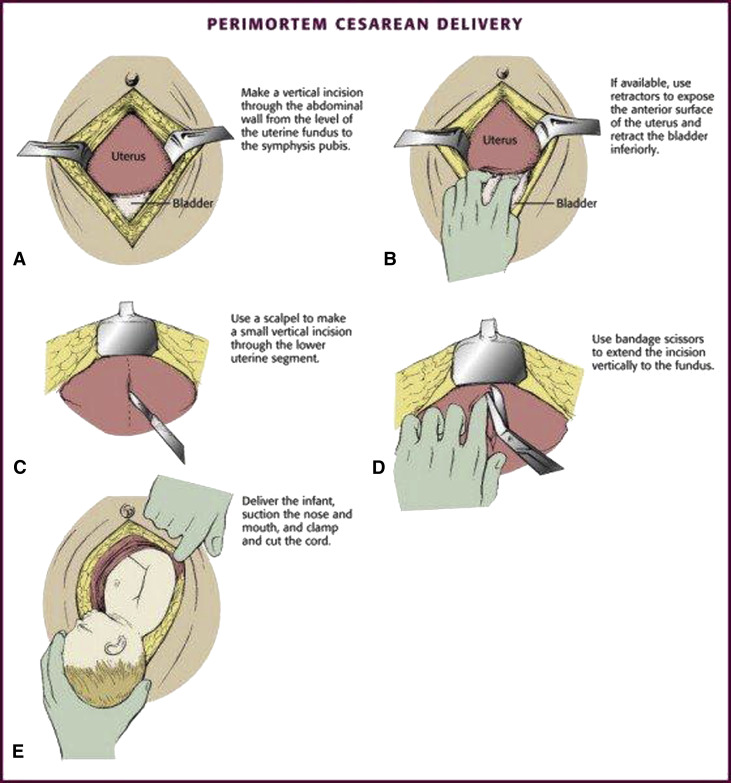
(3)
A literature search revealed very little evidence, however in 66 women and 68 neonates who underwent resuscitative hysterotomy for out of hospital cardiac arrest 4.5% of women and 45% of neonates survived to discharge. The longest down time was 29 minutes and 47 minutes for women and neonates respectively. While more evidence is needed, it appears this procedure should be performed as early as possible and may lead to some survival benefit.
Acute ischemic strokes involving the posterior circulation have significantly lower rates of hemorrhagic transformation after thrombolysis compared to anterior circulation strokes, a difference attributed to smaller infarct sizes and greater “ischemic tolerance” in the posterior circulation.
Given this lower hemorrhage risk, the EXPECTS trial evaluated the safety and efficacy of extending the thrombolysis window to 4.5–24 hours in patients with acute posterior circulation ischemic stroke who were not candidates for endovascular thrombectomy. This randomized controlled trial, conducted across 30 sites in China, enrolled 234 adults with mainly mild posterior circulation stroke (median NIHSS 3) and no evidence of extensive infarction on CT. Participants were randomized to receive either intravenous alteplase or standard medical care within the 4.5–24 hour window after symptom onset.
The primary outcome of functional independence at 90 days (modified Rankin Scale 0–2) was achieved in 89.6% of the alteplase group versus 72.6% of the standard care group. Rates of symptomatic intracranial hemorrhage were low and similar between groups (1.7% alteplase vs. 0.9% standard care), and 90-day mortality was lower in the alteplase group (5.2% vs. 8.5%).
These findings support extending the therapeutic window for intravenous thrombolysis in posterior circulation stroke beyond 4.5 hours when thrombectomy is not an option. However, the trial’s limitations, including a study population predominantly with mild strokes, exclusion of patients with extensive infarction, and enrollment limited to Chinese centers, warrant further investigation in larger and more diverse populations.
Bottom Line: Within limitations, emerging evidence supports an extended thrombolytic window beyond 4.5 hours for patients with posterior circulation strokes who are ineligible for thrombectomy.
The National Association of Emergency Medical Service Physicians reminds us that femur fractures rarely cause enough blood loss to cause hemodynamic instability (look for other sources), often have concomitant injuries in the pelvis or distal extremity, and can be effectively splinted either static or with traction (which has contraindications, complications, and technical hurdles).
A recent retrospective cohort study out of China investigated an escalating energy (200 > 300 > 360J) versus fixed energy (200 > 200 > 200 J) defibrillation strategy in OHCA with ventricular fibrillation requiring repeated defibrillations.
Notes:
Results:
Caveats:
An Australian retrospective study of 158 patients treated for nail gun injuries found those treated with operative debridement or with prophylactic antibiotics had no different 30 day infection rates compared to patients receiving no antibiotics.
Author: Matthew Jackson, MD
The Ket-Mid Study (1) is a recent RCT out of a tertiary center in a largely rural region of Egypt that evaluated combined ketamine (2 mg/kg) and midazolam (0.2 mg/kg) (ket-mid) to midazolam plus placebo (pla-mid) as the first line seizure abortive therapy. Children in the ket-mid group achieved 76% termination at 5 minutes compared to 21% of those in the pla-mid group (p<0.001). Adverse outcomes were rare, though the pla-mid group did have more hypotension.
Notably, the population included differed from that typically seen in the US. These kids were seizing for a long time, with a median seizure duration before IV meds of 34 minutes, and the benefit of ketamine on subgroup analysis seemed to shrink for those that were treated in less than 30 minutes. CNS infections were also much more common, accounting for the underlying pathology in 11% of cases. Important exclusion criteria also included trauma, inborn errors of metabolism, underlying CNS malignancy, and others not always known to EMS or ED clinicians at the time therapy begins.
This literature search from 1946-2023 looking at comparing selective use of CT scans vs whole body scans in geriatric trauma found no benefit of whole body CT in mortality, hospital length of stay or ED discharge. This study only included 15,000 pts over that very long time line. More robust, current work needs to be done on this important topic.