Shout out to UMEM alum Diane Kuhn, MD, PhD as the first author of this recent publication…
She and her colleagues examined the factors that contribute to ED patient experience scores, uncovering several which are not considered in the current CMS evaluative framework. See the editor's (our very own Stephen Schenkel, MD, MPP) capsule summary below:
What is already known on this topic? Medicare plans nationally standardized Emergency Department (ED) Patient Experience scores (ED
CAHPS) to allow comparison across sites.
What question this study addressed. Are there clinical and operational ED characteristics for which ED patient experience scores ought to be adjusted?
What this study adds to our knowledge. Based on 58,622 ED visits from one system, patients arriving in pain were less satisfied and those receiving radiologic studies had a positive experience.
How this is relevant to clinical practice. Influences on patient satisfaction are multifactorial and many are outside the control of the ED. Comparing EDs based on patient experience is complex and prone to misinterpretation.
As the authors point out, If patients placed in a hallway bed have a more negative experience simply due to the location in the department, or patients arriving in pain have a more negative experience regardless of ED care, then some EDs will face more challenges than others in achieving optimal patient experiences.
The current CMS evaluative framework may inherently disadvantage certain EDs, including those with limited physical space relative to their patient volumes, such as safety-net hospitals, or those that care for a high proportion of patients experiencing chronic pain. Is this fair? Does it reflect what CMS is trying to evaluate? Are there alternatives?
Kudos to Dr. Kuhn on her insightful publication and Dr. Schenkel for his expert editing!
Early Systolic Notching and Pulmonary Embolism
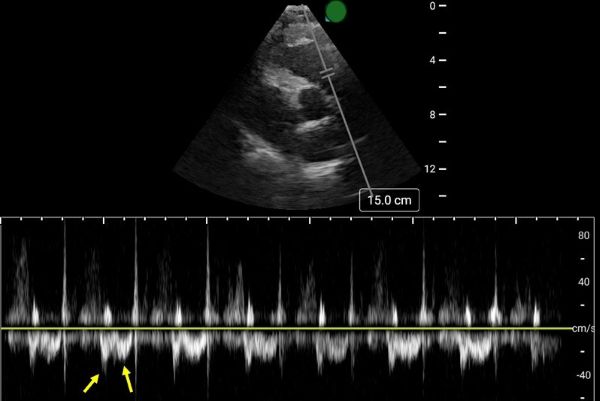
A prospective multicenter study conducted across four academic emergency departments in Turkey evaluated the diagnostic accuracy of early systolic notching (ESN) in emergency department patients. Among the 183 patients included, 52.5% were diagnosed with pulmonary embolism (PE), while 19.7% exhibited the ESN finding. ESN demonstrated a sensitivity of 34% (95% CI: 25–45%) and a specificity of 97% (95% CI: 90–99%) for PE. Sensitivity increased to 69% in patients classified as high or intermediate-high risk. Overall, ESN exhibits moderate to high specificity but low sensitivity, consistent with other sonographic signs of PE. Notably, ESN may also be present in patients with chronic thromboembolic disease secondary to prior pulmonary hypertension.
How to Obtain ESN
To detect ESN, acquire a parasternal short axis view at the base of the heart to visualize the right ventricular outflow tract and pulmonic valve. Position the pulse wave Doppler gate just proximal to the pulmonic valve, with the cursor traversing the outflow tract. ESN is characterized by a sharp systolic spike with a notch, followed by a dome-shaped waveform
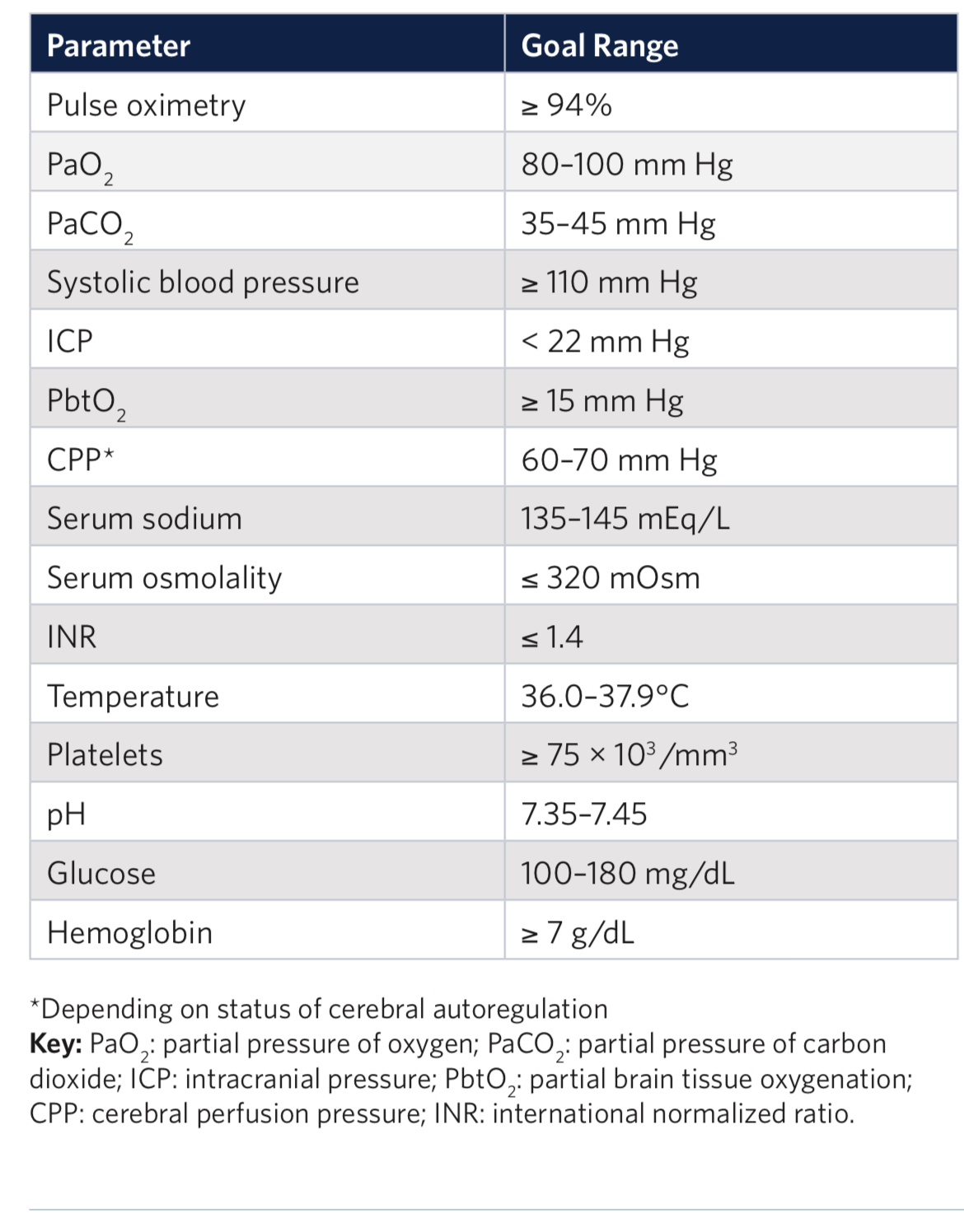
Outcomes in traumatic brain injury are improved when physiologic homeostasis is achieved as soon as possible after injury. Here are the American College of Surgeons’ recommendations. Note SBP over 110 and a hemoglobin over 7. A study looking at a more liberal transfusion target showed worse ARDS and no mortality benefit.
Trauma is a leading cause of death in pediatric patients. The Pediatric Traumatic Hemorrhagic Shock Consensus Conference Recommendations have stated that blood products are better than crystalloid and recommend the use of low titer type O whole blood (LTOWB) over individual components for pediatric traumatic resuscitation.
This study used the Trauma Quality Improvement Program Database to look at 1122 pediatric patients (< 18 years) over a 3 year period to retrospectively examine the impact of the ratio of whole blood and blood products given during the resuscitation of these patients. When at least 30% of the blood products delivered within the first 4 hours of resuscitation were low titer O whole blood, survival improved at the 6, 12 and 24 hour time mark.
The authors concluded that the observed survival benefit supports the greater availability and use of LTOWB during pediatric trauma resuscitation.
This was a multicenter retrospective cohort study over 6 years at 7 level one and two trauma centers.
1631 patients who had out of hospital traumatic cardiac arrest were included. The majority of the patients were adults, female, suffered penetrating trauma (64%) and were in a non-shockable rhythm. Prehospital epinephrine was given to 54% of patients.
Overall, survival to hospital discharge was lower in the epinephrine group (5% vs 16%). In the penetrating trauma subgroup, there was no statistically significant survival difference in patients who received epinephrine and those who did not.
EMS jurisdictions should examine their trauma arrest protocols and consider excluding the use of epinephrine. Several states, such as Maryland, have already removed epinephrine from the trauma arrest protocol.
Following up Dr. Flint's pearl from the other day, the largest study to date looking at a lower Mean Arterial Pressure (MAP) target in elderly ICU patients is the “65” Trial, published in JAMA in 2020. This trial compared a MAP target of 60-65 to the usual goal of >65, in critically ill patients age 65 and older. It included 2,455 patients in 65 ICUs in the UK, and found no difference between the groups.
Bottom Line: Although most intensivists still target a MAP > 65 regardless of patient age, you do have some evidence to support you if you want to target 60-65 in patients over age sixty-five. However, there are some important limitations (well outlined in the PulmCrit article linked below), and therapy should always be optimized to the patient and markers of end organ perfusion.
An open label pragmatic study in 29 Japanese hospitals randomized septic shock patients over age 65 to either a high (MAP 80-85) or control (65-70) group. They then looked at all cause 90 day mortality. The study was stopped early due to a significantly higher percentage of mortality in the higher MAP group.
The study isn’t blinded and is only done in one country, however it does raise the question of what is the ideal MAP for older septic shock patients.
This study from Great Britain compared fatalities for pedestrians and cyclist struck by motor vehicles based on vehicle body type. They found :
“We conclude that in Great Britain, being hit by an SUV as opposed to a passenger car increases injury severity among pedestrians and cyclists, with the strongest effect in children.“
https://the.emergencyphysio.com/wp-content/uploads/knee-lip-lateral.png
What do you see?
There is no clear fracture line
Much like ice floats on water, fat also floats on water/blood because it is less dense.
An intra-articular fracture may allow for blood and fat to exit the bone marrow and settle in the joint space.
This is called a lipohemarthrosis.
Best seen with a cross-table horizontal lateral view x-ray.
Go back to the image and examine the supra patellar pouch.
Most commonly seen in the knee in presence of a tibial plateau fracture.
Seen in approximately 1/3rd of tibial plateau fractures
If you see this without a clear fracture, consider CT of knee which can help detect the hidden fracture.
Remember the DDx of knee hemarthrosis with negative plain films:
Meniscal tear, ligament tear (usually ACL), patellar dislocation and osteochondral fracture.
Except for meniscal tearing (>6h) these other pathologies cause rapid onset swelling (<2h).
The presence of an endotracheal tube by itself does not mandate sedation and many patients require no sedatives while intubated in the ICU. However, patients intubated in the emergency department usually require initial sedation while still paralyzed from RSI. Sedation can also help facilitate procedures and imaging in critically ill patients during initial management.
Current literature has found increased mortality and length of ventilator requirement in oversedated ED patients. The target sedation level for the general population remains a goal RASS (Richmond Agitation-Sedation Scale) of 0 to -1. Society of Critical Care Medicine guidelines from early 2025 recommend dexmedetomidine over propofol as the preferred sedative for light sedation and reducing delirium risk in intubated critically ill patients. A recent trial re-examined other clinical outcomes between these two common sedative agents.
A2B Randomized Clinical Trial - JAMA 2025
Clinical Question: Does alpha 2 adrenergic receptor agonist sedation (dexmedetomidine or clonidine) reduce duration of mechanical ventilation in mechanically ventilated patients compared to a propofol based regimen (usual care)?
Where: 41 UK ICU’s from December 2018 to October 2023
Who: 1438 adults receiving mechanical ventilation for less than 48 hours, receiving propofol and opioid for sedation/analgesia, expected to require mechanical ventilation for greater than 48 hours
Intervention: protocol driven sedation to reach a RASS score of -2 to +1 (either dexmedetomidine, clonidine, or propofol). Of note, propofol could be added to achieve deeper sedation goal if deemed necessary by care team.
Outcomes:
Bottom Line:
While either dexmedetomidine or propofol, with appropriate use of opiates for pain management, are appropriate agents in non-paralyzed mechanically-ventilated patients, propofol may be a more appropriate choice in patients with greater agitation while boarding in the emergency department. However, close attention is needed to avoid the overly deep analgosedation associated with increased mortality. Maintain a goal RASS of 0 to -1 with frequent re-evaluation of your ICU boarders.
Digital nerve blocks are commonly used to provide anesthesia for finger injuries such as lacerations and dislocations. However, the procedure can be painful, as it often requires multiple injections into sensitive areas.
A recent single-center, unblinded randomized study compared the subjective discomfort and analgesic efficacy of traditional digital nerve blocks with ultrasound-guided peripheral nerve blocks. The study included 106 patients, with 53 in each group.
Results showed that patients in the peripheral nerve block group reported higher satisfaction rates. They also experienced less pain during the initial injection and longer-lasting analgesia compared to those who received digital nerve blocks. While digital blocks had a faster onset of anesthesia, they were associated with a higher rate of block failure.
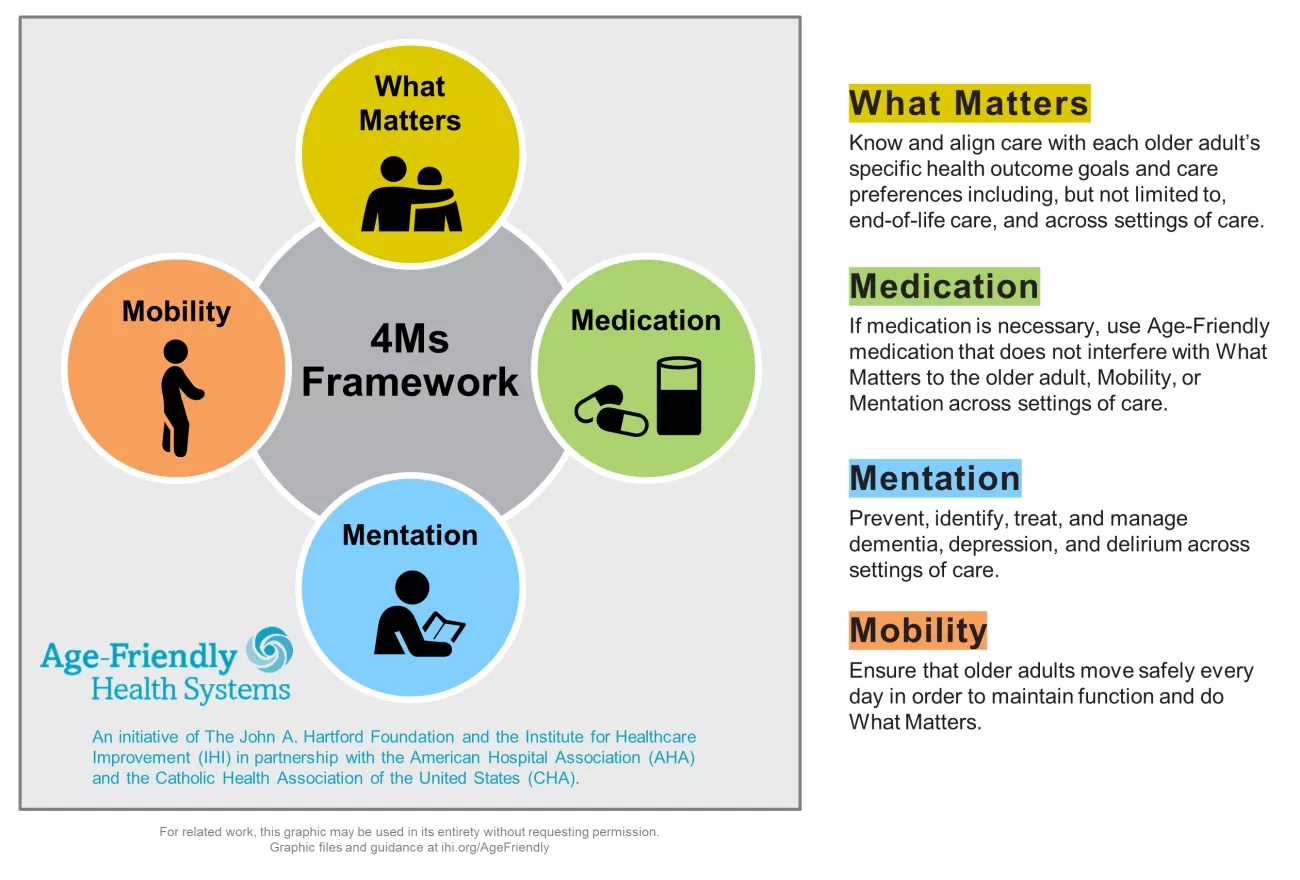
In mid-2024 the Center for Medicare and Medicaid Services introduced a new quality measure entitled Age Friendly Hospital Measure. The initial phase went into effect 1/1/25. It is built around programs from the American College of Surgeons, the American College of Emergency Physicians as well as the Institute for Healthcare Improvement (IHI). It is modeled around the IHI’s 4M Framework.
These authors looked at 5958 trauma patients arriving at their trauma center with a systolic blood pressure greater than 90. They calculated shock index (heart rate /sbp) for all of these and then looked at who received a blood transfusion within one hour of arrival. 211 patients received blood in that time frame. “Patients were stratified by SI using the following thresholds: ? 0.7, > 0.7 to 0.9, > 0.9 to 1.1, > 1.1 to 1.3, and > 1.3.”
“A main effect was observed for shock index with increased risk for required transfusion for patients with admission shock index >0.7 (P < 0.001). In comparison to shock index of ? 0.7, odds ratios were 2.5(1.7 - 3.8), 8.2(5.4 - 12.2), 24.9(15.1 - 41.1), 59.0(32.0 - 108.6) for each categorical increase in SI.”
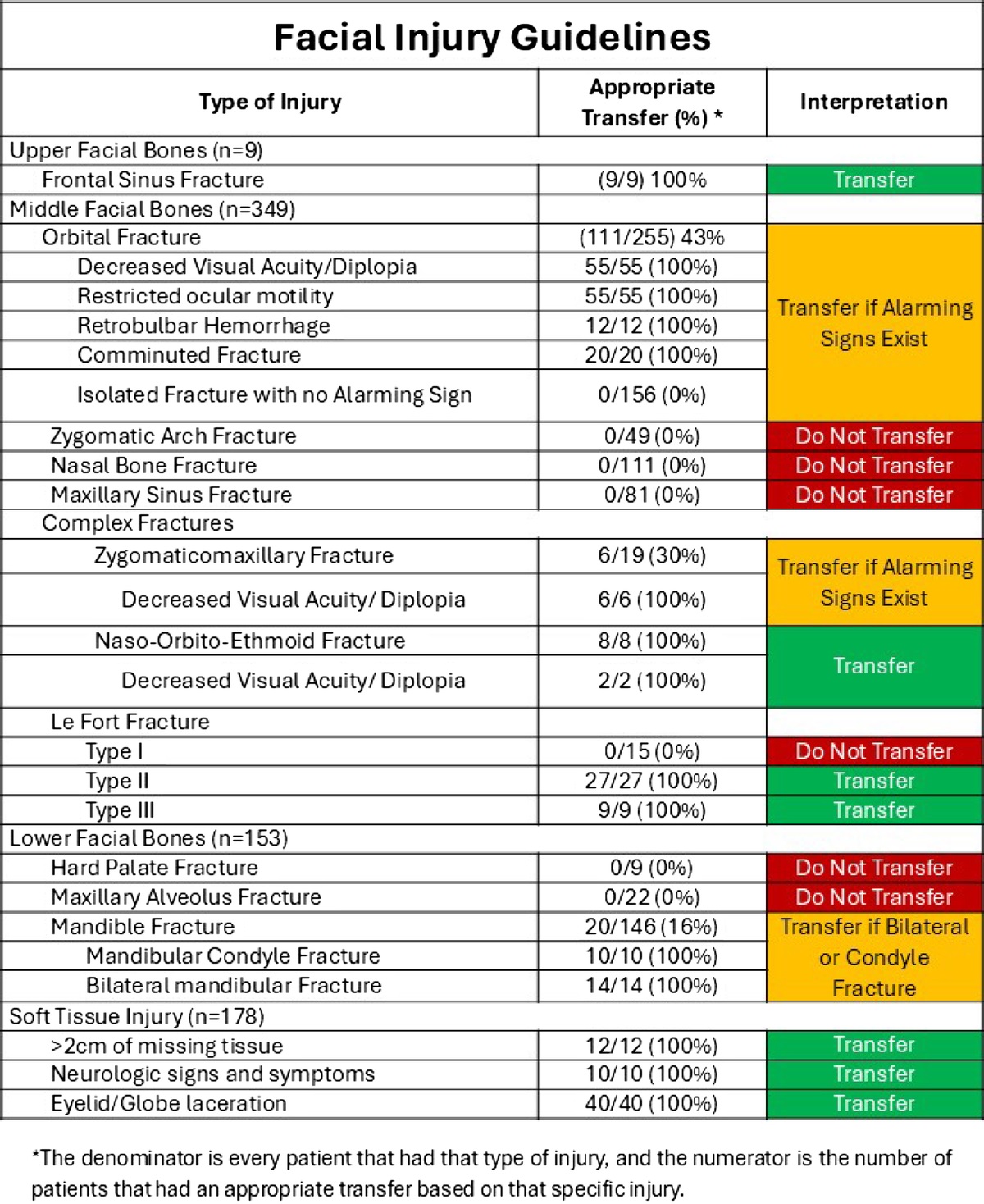
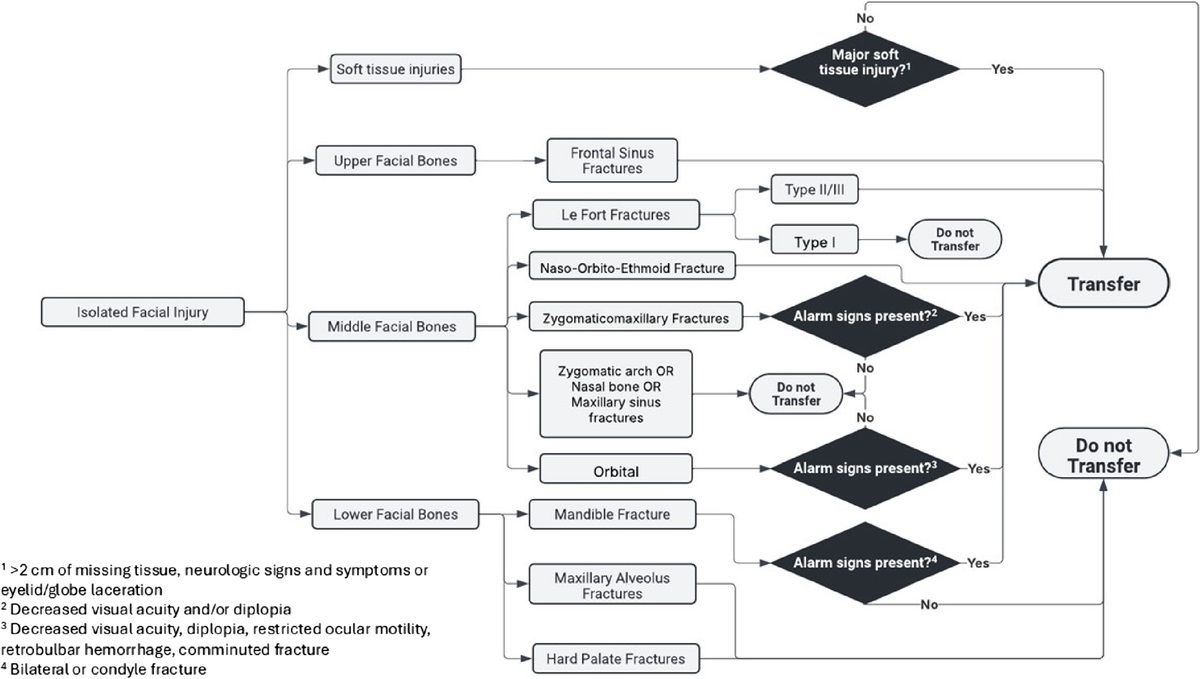
Based on a review of 511 patients transferred to a level one trauma center for evaluation of facial fractures, this group developed the Facial Fracture Transfer Guidelines. they found that over half of the patients transferred to them did not require intervention and were discharged within 6 hours. These guidelines are meant to decrease unneeded transfers yet provide appropriate care to those with traumatic facial injuries.
When To Initiate RRT in the Critically Ill Patient
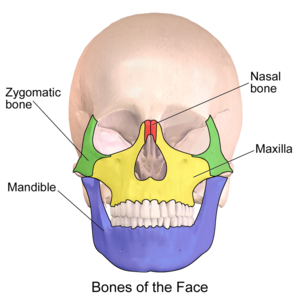
Most common facial fracture is the nasal fracture followed by the zygomatic arch fractures.
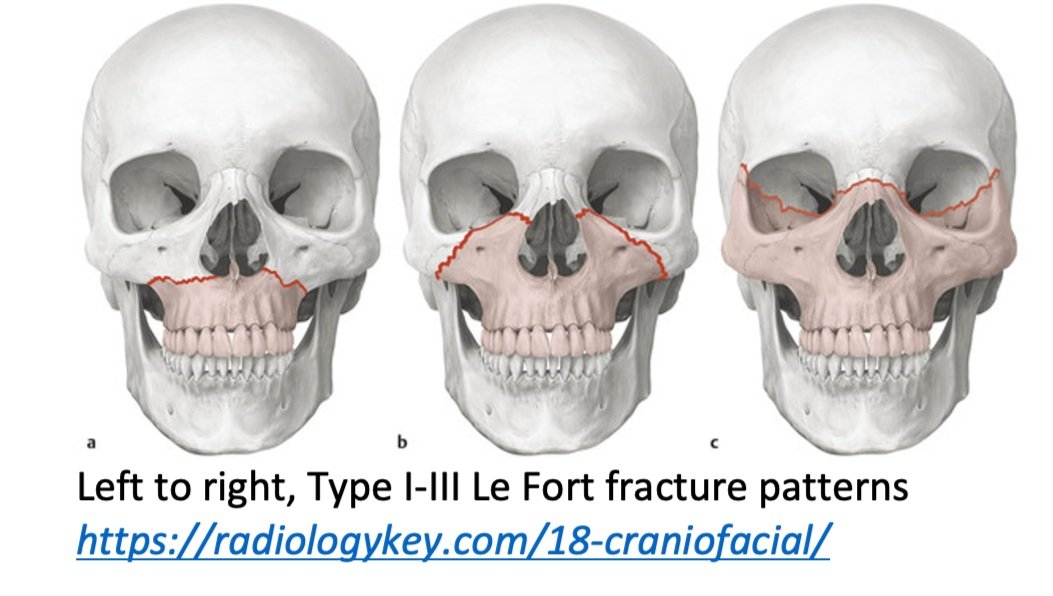
Le Fort Classification of facial fractures/facial stability. The higher the number, the more unstable.
Orbital blow out fractures may entrap the ocular muscles leading to eye immobility in various directions.
Haglund’s deformity
Calcaneal bony growth at the Achilles insertion
Also known as a “pump bump”
Risks: Tight & rigid shoes. Shoes with a hard heel counter. High arches. Tight Achilles tendon. Repetitive heel stress (jumping). Genetically prone bone structures.
Most common in woman between the ages of 15 and 35. Wearing heels. Runners.
Hx: Heel pain and tenderness with a noticeable bump at back of heel. Worse with walking and with certain footwear.
PE: Swelling and redness around bony prominence.
Pain and tenderness in the posterior heel, especially when pressure is applied.
Imaging: Excessive traction and abnormal biomechanics lead to insertional calcifications and bone spurs.
Over time, an exostosis may develop at posterior superior calcaneus as shown in the attached film.

Tx: Physical therapy and orthotics that alter heel height in shoe.
Surgery for chronic cases.
Malpractice Insurance comes in two varieties: Occurrence and Claims-made.
Occurrence covers lawsuits for which the event occurs while the insurance is active.
Claims-made only covers lawsuits for which the insurance is active both during the event and when the lawsuit is announced. It’s less expensive because the coverage period is both shorter and more definitive.
This is an important distinction when an event and a lawsuit may be separated by years, as happens with medical malpractice.
Occurrence is the “good” kind.
Claims-made requires a tail to cover any claims brought after the insured period ends.
Read how this can go awry in Emergency Medicine at Leon Adelman’s April post here, https://substack.com/home/post/p-161044772.
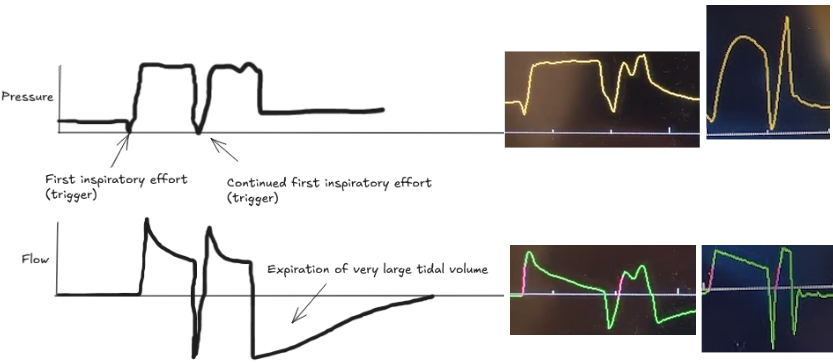
Patient-ventilator dyssynchrony is a sign of a disagreement between the patient's breathing and the ventilator's settings. Recognizing and fixing it is a critical skill to prevent lung injury and improve comfort. Ineffective triggering and double-trigger are two common types of dyssynchrony.
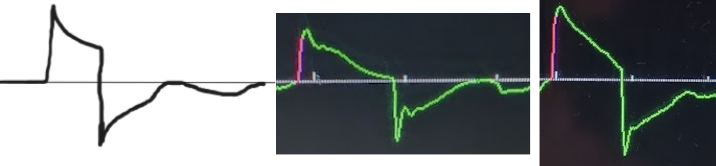
The patient tries to take a breath, but they are too weak to trigger the ventilator. This is the most common type of dyssynchrony. It causes increased work of breathing and discomfort.
Look for a small dip in the pressure waveform and a simultaneous scoop out of the expiratory flow waveform that is not followed by a delivered breath.
Troubleshooting options:
The patient's own breath outlasts the ventilator's set inspiratory time (Ti), causing one patient effort to trigger two stacked breaths. This results in delivery of large tidal volumes, risking lung injury (volutrauma).
Look for two consecutive breaths on the ventilator screen without a full exhalation in between.
Troubleshooting options:
Dyssynchrony means the ventilator settings do not match the patient's needs. Watch the waveforms to diagnose the mismatch, then either adjust the ventilator or treat the underlying problem.
Brain injury guidelines were designed to decrease transfers and neurosurgical consults for adults with head injuries.
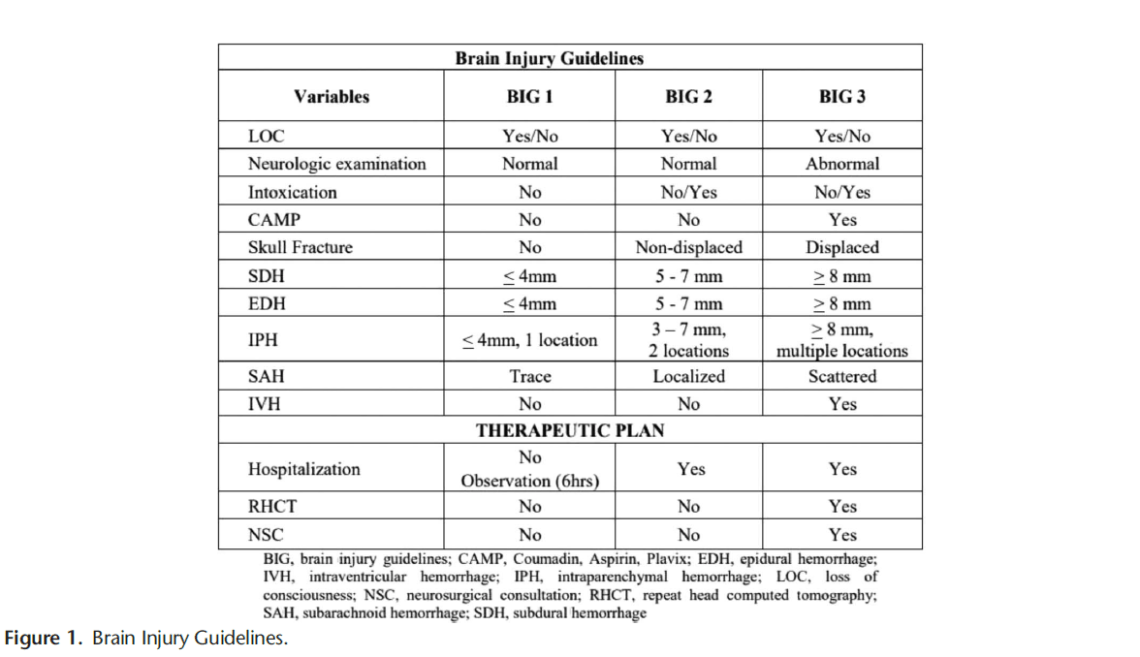
A new retrospective study suggests that modified guidelines may be feasible in the pediatric population as well. More data is needed but this is an important step in assuring safe resource utilization in pediatric head injury patients.
{kind=link}