Lidocaine transdermal patches
Frequently used for lower back pain.
A single 5% patch contains 700mg of lidocaine.
There is low systemic absorption.
Data supporting efficacy for lower back pain are limited.
Best benefit in other neuropathic conditions such as post herpetic neuralgia.
Topical capsicum
Underused, safe, non-sedating.
Potential treatment option for acute and subacute back pain (<3 months duration).
Can be OTC or via prescription.
Available in cream, lotion and patches.
Best used 3-4 times per day for maximal effectiveness.
Grade A recommendation from North American Spine Society.
The Pan-Asia Trauma Outcomes Study database was reviewed for differences in in-hospital mortality and functional capacity at discharge between male and female trauma patients. There were 76,000 trauma patients from 12 Asian countries in this study. The authors concluded: “This study indicates no difference in the general trauma outcomes in the Asia Pacific between females and males. Although younger females with less severe injuries had better functional outcomes, this advantage disappeared in severe injuries and those over 50 years.” There were several differences in mechanism of injury and age of presentation. “With females more frequently represented in the ??50 age group (60.13%) compared to males (44.87%) (p?<?0.001). Trauma type also varied between sexes; 95.51% of females experienced blunt trauma compared to 93.65% of males (p?<?0.001). Anatomically, males predominantly sustained injuries to the head, face, thorax, abdomen, and upper extremities, whereas females more frequently suffered injuries to the lower extremities and spine (p?<?0.001).” This is similar toEuropean and North American data
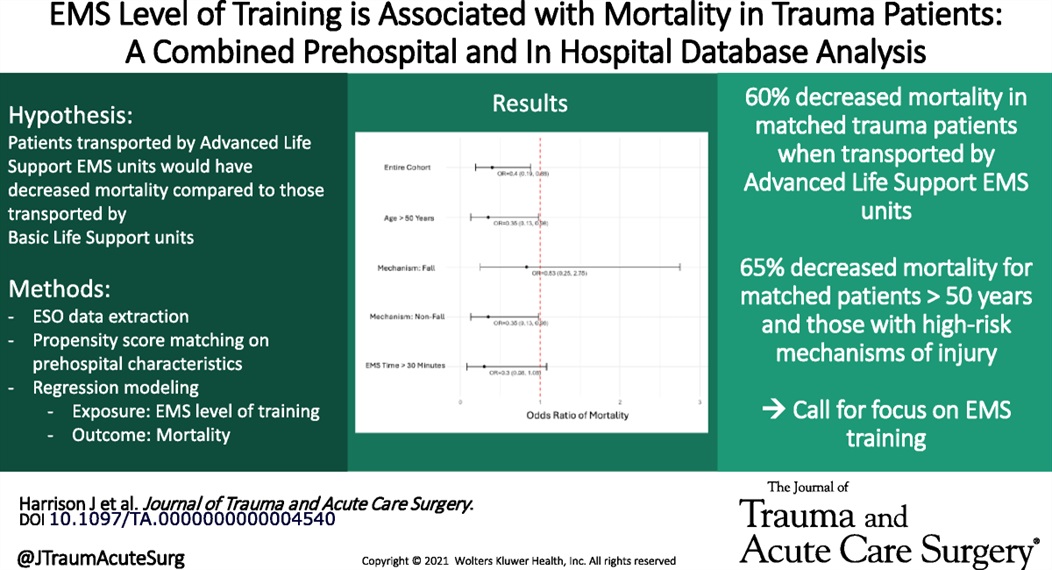
Large retrospective propensity matching study looking at mortality in trauma patients based on ALS vs. BLS transport crew found lower mortality in those attended by ALS crews. The matching was “based on patient age, sex, year, ICD-10-CM based injury severity score, mechanism of injury, AIS based body region of injury, EMS characteristics including time with patient and prehospital interventions performed, prehospital vital signs, and trauma center designation.”
This is different than other studies which showed limited difference. other studies have shown improved survival with police “scooping and running” with penetrating trauma patients.
Intubation and mechanical ventilation of brain injured patients, which is extremely common in the Emergency Department, can be very challenging and subject to significant practice variation. It is often said that brain injured patients “can't take a joke”, meaning that they are less tolerant to hemodynamic and metabolic perturbations, and these perturbations tend to be associated with very large swings in their clinical outcomes. For example, hypo/hyperglycemia, hypo/hypernatremia, hypo/hypertension, hypo/hyperoxia, hypo/hypercapnea, etc are all extremely important to avoid. This is probably the one patient population where “euboxia” (the notion that we obsess too much about making all the numbers pretty in the EMR) is probably not as applicable. As such, there is at least good physiologic rationale, and now increasing empirical evidence, that ventilating these patients very thoughtfully is extremely important and likely to have meaningful impact on patient-oriented outcomes (mortality, neurologic outcome, etc).
The VENTIBRAIN study was a prospective observation trial of 2,095 intubated patients in 26 countries who had TBI, ICH (including SAH), or acute ischemic stroke. Interestingly, they found that patients with lower tidal volume (TV) per predicted body weight had higher mortality (although the majority of their TVs were well controlled and in a fairly tight range), which is contrary to conventional thinking in pulmonary pathologies like ARDS. They also found that higher driving pressure (DP) was associated with higher mortality, which agrees with data from other conditions. PEEP and FiO2 had U-shaped curves, but FiO2 in particular tended to favor lower FIO2, also similar to current thinking for ICU patients in general.
Take Home Points:
A recent study evaluated the accuracy of POCUS in detecting retained products of conception (RPOC) in the emergency department.
In this study, a patient was considered positive for RPOC if they had heterogenous material in the endometrium measuring 10 mm or more. Color Doppler was not used for further evaluation, though it has been cited in obstetric literature as a helpful tool.
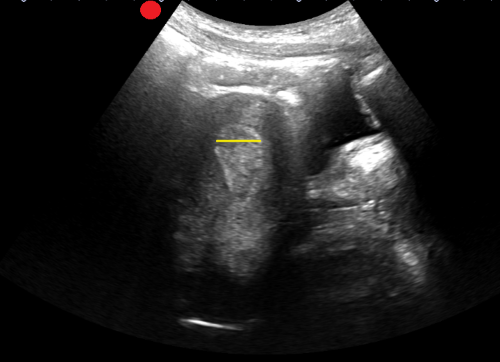
Among the 265 patients included, the prevalence of RPOC was 21.5%. POCUS had a sensitivity of 79.0 % and a specificity of 93.8 %.
The authors caution against the use of POCUS to diagnose RPOC in the setting of early pregnancy, as the endometrium can have a variable appearance, increasing the risk of a misdiagnosis. Of the 22 false positives identified, more than half were potentially viable pregnancies. Uterine fibroids can also lead to a heterogenous appearance of the uterus and can be another potential false positive.
Rib and pelvic fractures are common findings in geriatric trauma patients, even in low impact trauma such as falls from standing. Pain management is vital for improving morbidity and mortality. The IFEM White Paper suggests:
“Use multimodal pain management strategies, including regional anesthesia and non-opioid analgesics, to control pain without compromising recovery.
Monitor closely for complications such as pneumonia or hemodynamic instability, intervening promptly to mitigate risks.
Collaborate with physiotherapists to implement early mobility programs, reducing the risk of deconditioning and promoting recovery.”
A multidisciplinary team proficient in geriatric trauma care leads to better outcomes. This may require transfer to a trauma center.
This white paper reminds us that age is just a number; frailty is a better predictor of morbidity and mortality after trauma.
“Frailty, characterized by reduced physiological reserve and increased vulnerability to stressors, is a significant factor influencing recovery from trauma. Individuals with frailty may experience slower healing, higher rates of complications, and longer hospital stays. Tools such as the Clinical Frailty Scale (CFS) and the Trauma-Specific Frailty Index (TSFI) have been developed to assess frailty systematically, enabling clinicians to predict outcomes and guide treatment decisions.”
Nurse Practitioners and Physician Assistants practice alongside Physicians in Emergency Departments. In 2021, an estimated 17,679 NPs and PAs worked in EDs.
How long do NPs and PAs continue in Emergency Medicine practice?
An analysis of Medicare data reports that over the eight years of the study, the annual attrition rate averaged 13.8%, or almost 1 in 7 leaving Emergency Medicine practice every year. At the time of attrition, the median age for women was 40.2 years (IQR 33.8 to 49.9) and for men was 45.9 (IQR 37.8 to 56.3).
For additional breakdown and discussion of these numbers, see Gettel CJ, Chosh R, Rothenberg, et al. Workforce Attrition Among Emergency Medicine Non-Physician Practitioners. Ann Emerg Med, in press, https://www.annemergmed.com/article/S0196-0644(24)01294-0/fulltext.
Non-Pharmacologic Measures to Prevent VAP
Point-of-care ultrasound (POCUS) measurement of the optic nerve sheath diameter (ONSD) has been shown to correlate with increases in intracranial pressure (ICP).
In adults, an ONSD measurement of less than 5 mm is considered normal, while a measurement greater than 6 mm suggests elevated ICP.
How to Measure the Optic Nerve Sheath Diameter:
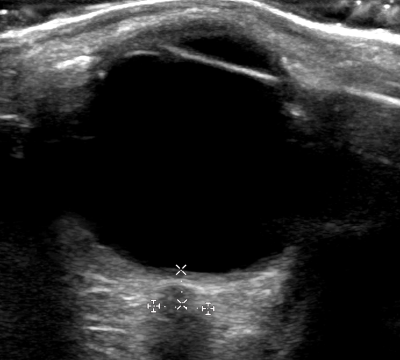
A small cross-sectional study examined whether ONSD measurements varied when taken at different depths. The findings indicated that ONSD increased by 0.32 mm at a depth of 4 mm and decreased by 0.54 mm at a depth of 2 mm.
These variations highlight the importance of maintaining a consistent measurement depth. To ensure accuracy and avoid misinterpretation, the ONSD should always be measured 3 mm posterior to the retina.
This position paper from American College of Surgeons, NAEMSP, and ACEP outlines a literature based approach to prehospital care of traumatic circulatory arrest. It logically could be applied to care in the hospital as well. Care of a traumatic arrest is different than a medical etiology arrest.
“Emphasize the identification of reversible causes of traumatic circulatory arrest and timely use of clinically indicated life-saving interventions (LSIs) within the EMS clinician’s scope of practice. These include:
Epinephrine should not be routinely used, and if used should not be administered before other LSIs.
External chest compressions may be considered but only secondary to other LSIs.
Chest decompression if there is clinical concern for a tension pneumothorax. Empiric bilateral decompression, however, is not indicated in the absence of suspected chest trauma.
Airway management using the least-invasive approach necessary to achieve and maintain airway patency, oxygenation, and adequate ventilation.
External hemorrhage control with direct pressure, wound packing, and tourniquets.”
A previous pearl discussed Spondylolysis. Once clinical concern is sufficient, the question of appropriate imaging arises.
Traditionally, the addition of oblique radiographs was recommended because they showed the pathognomonic “Scotty dog” sign. Recent studies have shown there is no significant increase in diagnosing spondylolysis with the addition of these oblique views. These additional views carry added cost and radiation exposure (approximately double).
AP and lateral radiographs offer similar diagnostic sensitivity to the old four view series.
If plain films are negative and symptoms persist despite 2-3 weeks of rest from offending activities, advanced imaging can be pursued on an outpatient basis. This is also strongly considered if the patient wishes to return to sport.
Despite being primarily osseous pathology, studies have shown that MRI can have similar diagnostic sensitivity to CT particularly in cases of acute injury. MRI may also show signs of stress reaction before complete fracture occurs.
Communicate with radiology and MRI technicians that you are looking for spondylolysis as this may affect the MRI sequences.
If a positive finding occurs on plain film, ordering CT imaging for the entire lumbar spine should be deferred due to added radiation concerns especially in cases where MRI would be available.
If MRI is not practical, consider limiting CT to one level above and one level below the region of concern. This would decrease the radiation exposure by approximately 50%
If advanced imaging is not practical or available and patient has a positive plain film, consider recommending repeat imaging in 4-6 weeks as an outpatient with rest from all offending activities.
This was a retrospective cohort study of the national trauma data bank that included about 64000 pediatric trauma patients in the derivation group and the same amount in the validation group. The authors empirically created upper and lower cut off values for the shock index based on age. They compared the shock index based on age cut offs with major trauma as defined by the standardized triage assessment tool criteria.
The empirically derived age adjusted values had a sensitivity of 43.2% and a specificity of 79.4% for major trauma. The sensitivity of the pediatric shock index (PSI) in that same group was 33.9% with a specificity of 90.7%. The pediatric-adjusted shock index (SIPA) had a 37.4% sensitivity and 87.8% sensitivity for 4-16 year olds.
Shock index = (Heart Rate / Systolic BP)
Pediatric Shock Index (PSI)
For children age 1-12 years
SI > 1.55 - (0.5) x (age in years)
Patients with an elevated shock index had a 5.02 greater odds of major trauma in this study.
This study used age specific cut offs such as:
1 yr to < 3 years = lower limit of 0.73 and an upper limit of 1.40
(see article for a full table).
Patients with a shock index below the lower limit had a 1.55 greater offs of major trauma and patients with a shock index above the upper limit had a 3.97 greater risk of major trauma.
Bottom line: Shock index alone has a limited role in the identification of major trauma in children. Of these three methods for calculating/interpreting shock index, PSI seemed to do better.
Multiple trials have aimed to assess the effect of blood pressure control in the prehospital setting for patients with suspected acute stroke. The INTERACT-4 trial was a multicenter, prospective, randomized, open-label, blind endpoint trial conducted in China, in which 2404 hypertensive patients with suspected acute stroke (based on FAST score >2, symptom onset <2h, SBP >150mmHg) were randomized to receive urapidil versus usual care in the prehospital setting. The primary outcome was modified Rankin score (mRs) distribution at 90 days. Overall, no significant difference in functional outcomes at 90 days were observed in the urapidil versus usual care groups (OR 1.00, 95% CI 0.87-1.15). However, when analyzed by stroke type, improved functional outcomes and lower rates of rebleeding were seen in patients with hemorrhagic stroke (46.5% of all enrolled patients), while worsened functional outcomes and mortality were seen in patients with ischemic stroke. These observations are consistent with standard practices of intensive blood pressure reduction in patients found to have ICH, versus the “permissive hypertension” approach to patients found to have cerebrovascular occlusion. The results of this trial are not practice-changing, but do highlight the importance of prompt stroke recognition, streamlined hospital workflows for expedited diagnostics (CT), and timely initiation of antihypertensive therapy in ICH patients.
Bottom line: Prehospital blood pressure reduction was not shown to improve clinical outcomes in hypertensive patients suspected to have acute undifferentiated stroke.
Previous studies have suggested that a single dose of epinephrine in out of hospital cardiac arrests compared to multiple dose protocols result in a similar survival to hospital discharge rate. This study aimed to see if single dose epinephrine compared to multiple doses improved survival in the subset of patients that were 1) in a shockable rhythm or 2) received bystander CPR.
This study looked at patients from 5 EMS systems in North Carolina before and after a protocol change from multiple dose epinephrine to single dose epinephrine in cardiac arrest. 1690 patients were included, 19.2% with a shockable rhythm and 38.9% who received bystander CPR.
The study found:
- Survival to hospital discharge was higher in the single dose epinephrine group who received bystander CPR
- Survival rates were similar in the single and multiple dose epinephrine groups for patients who were initially in shockable rhythms, in asystole/PEA and who did NOT receive bystander CPR.
Bottom Line: More studies are needed to support prehospital protocol changes.
Arterial lines are essential tools in managing critically ill patients, but it is frustrating when they are not working as expected. It can be hard to tell when an unexpected waveform or pressure reflects the patient's physiology versus a problem with the line. Recognizing common issues and systematic troubleshooting will optimize your hemodynamic monitoring.
Types of arterial line problems
Troubleshooting Steps
By following these steps, you can systematically identify whether waveform or pressure abnormalities are due to technical issues or true patient physiology.
Looking at 416 patients aged 12-16, 48% at a Peds trauma center vs 20% at adult Level 1 center vs 34% at an adult level 2 center, there was no difference in in hospital mortality between adult and pediatric centers.
The authors conclude “These findings suggest that severely injured adolescents aged 12 to 16 years may be safely treated at either adult or pediatric trauma centers.”
Background:
Approximately 10% of patients presenting to the emergency department (ED) report penicillin allergies, which may lead to use of second- or third-line agents. Alternative therapies (such as aztreonam, clindamycin and fluroquinolones) carry an increased risk of mortality and complications such as Clostridioides difficile infection. Considering that less than 10% of penicillin allergies may be confirmed by formal testing results, the PEN-FAST clinical decision tool was created to identify patients with low risk of true penicillin allergy who do not require formal skin testing for rechallenging with a beta-lactam:

Though PEN-FAST has only been validated in the clinic and inpatient settings, a study from Tran et al. published this January sought to determine the safety and efficacy of utilizing this tool to assess penicillin allergies and re-challenge patients in the ED.
Study design:
This was a single-center, prospective, observational cohort study. Emergency medicine (EM) pharmacists screened patients in the ED with:
Screened patients were excluded from the study if orders were placed by a non-EM physician, if they previously tolerated a penicillin/cephalosporin within the healthcare system of the study site, if they were unable to participate in bedside interview, if the antibiotics selected were appropriate despite the penicillin allergy or if there were time constraints that would delay care if the PEN-FAST assessment needed to be completed.
Study Intervention:
EM pharmacists completed the PEN-FAST assessment for all included patients. They recommended rechallenging with an appropriate beta-lactam for patients with a score of 0-2, recommended to consider rechallenging for patients scoring 3, and did not recommend rechallenging for scores of 4-5 or if it was confirmed patients previously experienced anaphylaxis, angioedema or severe cutaneous reactions with a beta-lactam. Orders for any change in therapy were only placed with discussion and agreement from EM physicians. Rechallenged patients were assessed at bedside for any immune-mediated reactions 45 to 75 minutes after initiation of antibiotics. The primary outcome was the percent of patients with a PEN-FAST score of 0-2 who tolerated a beta-lactam after being rechallenged.
Patient Characteristics:
After screening, one hundred patients were included in this study.
Results:
Primary Outcome:
Secondary Outcomes:
Key Takeaways:
Background
Diagnosed by continuous seizure activity that lasts for 5 minutes or more and/or multiple seizures that occur without returning to baseline in-between each. Further classified as being convulsive or non-convulsive. Refractory status epilepticus can be defined as status epilepticus that does not respond to an adequately dosed benzodiazepine and another anti-seizure medication. The primary objective in management is to stop both clinical and electrographic seizures which can become an important point for those patients who require intubation and receive neuromuscular blockade. Essential to evaluate early for reversible causes (electrolytes, liver function, glucose, ammonia, medications) and for other precipitating causes with toxicology screening and CT head imaging with consideration for angiography and venography.
Management:
First-Line/Initial Therapy:
Lorazepam IV 0.1 mg/kg up to 4 mg per dose is the preferred agent, can be repeated after 5 minutes if seizures persist
Diazepam 0.15 mg/kg IV/0.2 mg/kg PR up to 10 mg, or midazolam IM 0.2 mg/kg up to 10 mg are also alternatives
Second-line/Urgent control: (Provided to all patients with SE after initial therapy)
- Levetiracetam 60 mg/kg, Valproate 40 mg/kg, and fosphenytoin 20 mgPE/kg were studied by Kapur et al., and they found similar rates of resolution of status epilepticus with similar rates of adverse events.
- Phenobarbital 15-20 mg/kg is another agent that has good efficacy and is remerging as an effective agent. Can cause respiratory depression at high doses.
- Keppra may have the best side-effect profile to consider.
- Valproate can cause hepatotoxicity, elevated ammonia and thrombocytopenia.
- Fosphenytoin can cause hypotension and arrhythmias.
Third-line:
Midazolam 0.2 mg/kg load followed by 0.05 – 2 mg/kg/hr infusion
Propofol 1-2 mg/kg load followed by 20-200 mcg/kg/min infusion
Ketamine 0.5 – 3 mg/kg load followed by 1.5-10 mg/kg/hr infusion
Pentobarbital 5 mg/kg load followed by 0.5-5 mg/kg/hr infusion
- Propofol carries the risk of propofol infusion syndrome with high doses or prolonged infusions, some favor midazolam because of this.
No conclusive data to support one over another.
Important Considerations
- A common mistake is to under-dose benzodiazepines for initial therapy, give the full weight-based dose as described above.
- Following initial management it is important to monitor patients with continuous EEG if they have not returned to their neurologic baseline
- Propofol, midazolam or ketamine are good options for induction for intubation.
- Consider against using etomidate for induction of intubation since it can cause myoclonus which can complicate the picture if you are already worried about seizures, can be hard to differentiate.
- If intubation is required and EEG is not readily available consider reversal of neuromuscular blockade after intubation to better monitor for continued seizures.
- If in refractory status epilepticus despite using a second-line agent and a third line agent then consider adding a second agent from the second-line/urgent control that was not previously started (fosphenytoin, valproate, levetiracetam, or phenobarbital).
In the last few months, there have been multiple articles published regarding the use of prophylactic TXA to prevent postpartum hemorrhage. While almost none of us want to ever be in the situation where we have to deliver a baby in the ED, we need to be prepared for all outcomes.
A meta-analysis by Ker et. al (Oct 2024) and a RCT, blinded study by Zhang et. al (Dec 2024) both demonstrated that giving 1g TXA immediately after delivery of a baby can reduce the rate of severe postpartum hemorrhage in patients with risk factors. These studies had a wide variety in what they considered risk factors, but a few that showed particular significance included: hx of postpartum hemorrhage, history of anemia, gestational diabetes, and placental adhesion.
So next time you've scooped that screaming baby out into your already chaotic emergency department, ask your patient (not the baby) a few questions about their birth history and think about giving 1g of TXA to prevent a horror show for whoever is coming on for you next.
Caveat: These studies were done in delivery rooms and not emergency rooms, but I think we can extrapolate since it would be very hard to find enough patients to conduct a study like this in the emergency department.