This review article in the Journal of Trauma and Acute Care Surgery states:
“In obtunded patients, an adequate and normal high-quality CT supports collar removal without the need for adjunctive imaging.”
In a randomized multicenter trial comparing direct vs video laryngoscopy in trauma patient intubation, video had a higher first pass success rate and equal complication to direct laryngoscopy.
This single center prospective study asked residents to determine if their patient had barriers to post ED discharge health care such as having a PCP, transportation issues, affording medications, and need for assistance with activities of daily living. They then compared the physicians’ answers to patient’s answers and found: “Physicians had poor sensitivity for accurate identification of patient barriers.”
Some of our discharged patients are struggling more than we realize.
This multicenter study looked at trauma patients with a hemothorax who underwent early tube thoracostomy vs. being observed. They found volume of over 300 ml predicted observation failure. Those observed had shorter hospital stays and less ICU admissions. Twenty two percent of observation patients required tube thoracostomy. The failed observation group had similar outcomes except longer hospital stays.
Expert consensus recommends not prescribing these eight classes of medications to older adults mostly due to sedative affect and fall risk. 1. Benzodiazepines 2. Barbiturates 3. Muscle relaxants 4. 1st generation antihistamines 5. Sulfanylureas 6. 1st generation antipsychotics 7. Zolpidem 8. Metocloprimide
A recent study shows marginal improvement in not prescribing these medications to older ED patients.
This single center study looked at diabetic patients who had a POC glucose over 300 and POC ketone over 1.1 and reviewed their diagnosis vs the laboratory accepted diagnosis of DKA.
“The most recent international consensus laboratory definition of (non-euglycemic) DKA includes a glucose of >?250; a pH <?7.3 or a bicarbonate ??18?mmol/L; and a beta-hydroxybutyrate (BOHB) ??3.0?mmol/L or urine ketone strip ??2+”
This nice review article reminds us “The AO-Spine classification is the most frequently utilized system for thoracic and lumbar fractures, and it categorizes fractures into three types. Type A fractures are compression injuries. In these fractures, the assessment of the involvement of the posterior elements of the vertebral body is essential. Type B fractures are distraction injuries implying tension band involvement, whereas type C fractures are translational or dislocated injuries. The AO-Spine Upper Cervical Injury Classification System… In this classification system, type A injuries have no ligamentous involvement and are considered stable. Type B injuries have tension band or ligamentous injury and may be unstable. Type C injuries are characterized by significant translation and loss of anatomic integrity and are considered unstable."
These authors argue that bystander interventions in the early minutes (they call them the diamond minutes) can have an impact on trauma survival. Particular attention to External hemorrhage control; Airway opening and maintenance; Safe positioning of unconscious patients; Mitigation of early hypoxia and hypothermia could improve survival. We need to publicize this information and undo the years of teaching not to move these patients due to concern of secondary spinal cord injury. Many studies have dispelled that concern.

This article suggest that freeze-dried plasma (FDP) is an acceptable adjunct to whole blood for prehospital resuscitation of trauma patients. “FDP is pathogen-reduced, shelf-stable for up to two years at room temperature, lightweight, and rapidly reconstituted at the point of care.” This method offers an advantage when caring for patients in remote areas with long transport times and has been used by NATO and Canadian armed forces.
Of the 215 Norwegian patients on oral anticoagulation seen for a head injury and having a normal initial head CT, none developed delayed hemorrhage. Median age was 83 years.
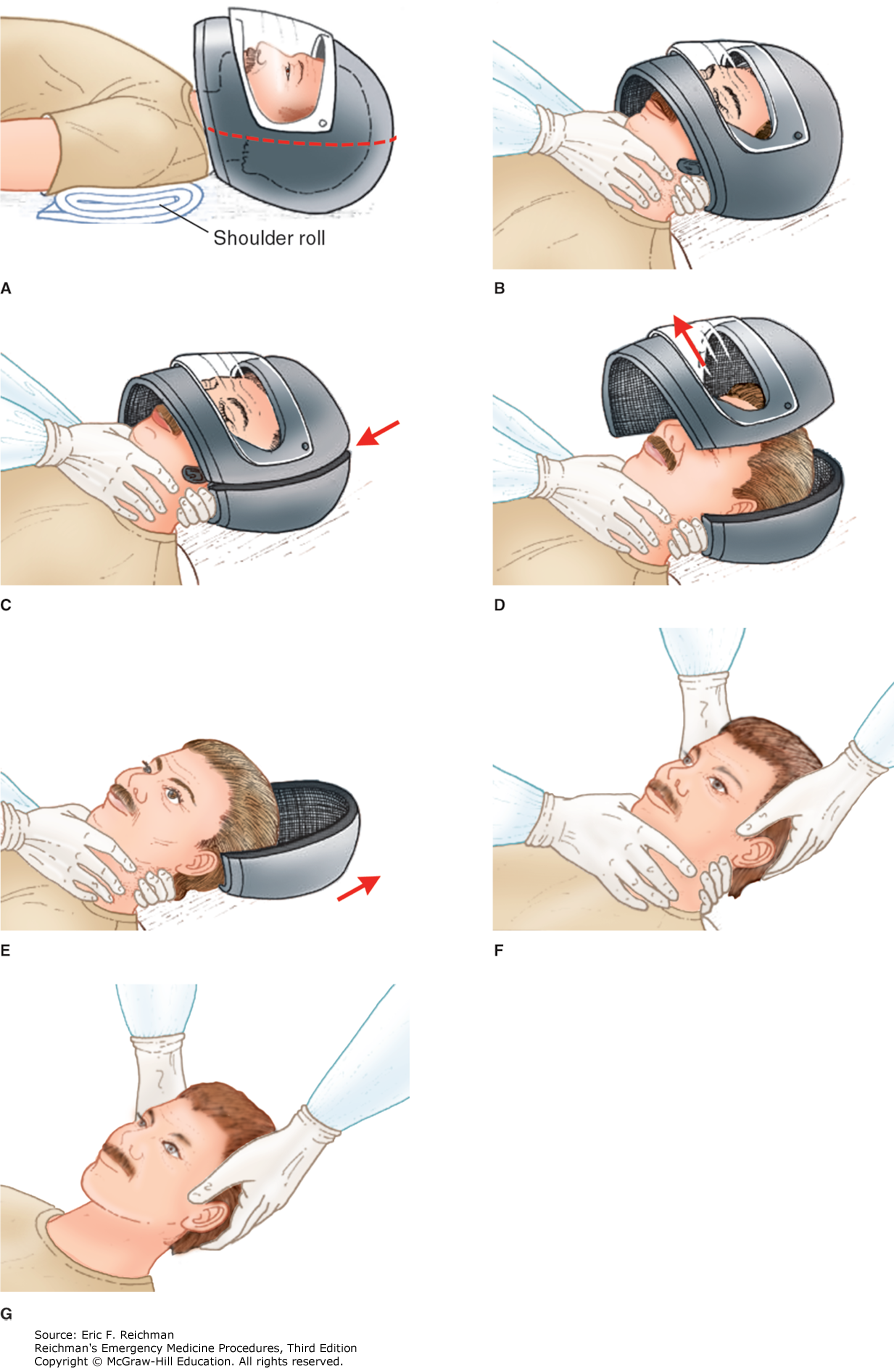
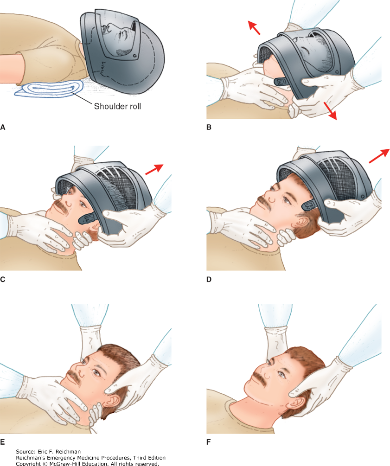
Here are two techniques to remove a helmet from an injured motorcyclist. The first uses a cast saw to bivalve the helmet. A link for a video is also provided.
In 290 trauma patients diagnosed with dementia prior to injury, when compared to 3000 patients over age 65 without dementia and similar injury severity score, the dementia patients had a much higher rate of discharge to an institution instead of back to home living. This was particularly true of older women.
This article describes a paramedic run community health initiative to assist people with dementia transition to home after an ED visit. They describe:
“Persons living with dementia (PLWD) frequently use the emergency department (ED) for unscheduled care and experience significant challenges during the ED-to-home transition.
The Community Paramedic-led Transitions Intervention (CPTI) is a structured, coaching-based program delivered by community paramedics that includes a home visit and follow-up calls to support PLWD and care partners during the 30?days after ED discharge.”
Could your ED use a program like this to prevent readmissions?
A retrospective study looking at use of transdermal Buprenorphine in older trauma patients with rib fractures found a good safety profile (less naloxone use) and less overall opioid use however no change in overall length of stay or mortality. Adding this to your multimodal pain strategy in older patients with rib fractures seems like a reasonable plan.
A narrative review of literature involving older patients and constipation found:
“Major contributing factors include physical inactivity, sarcopenia, dehydration, inappropriate defecation posture, and polypharmacy, particularly opioids and anticholinergic agents. Importantly, these factors interact through the brain–gut–microbiota axis, contributing not only to gastrointestinal dysfunction but also to systemic outcomes such as frailty, cognitive decline, and increased healthcare burden, thereby supporting a multidimensional disease framework.”
It isn’t as simple as adding a laxative.
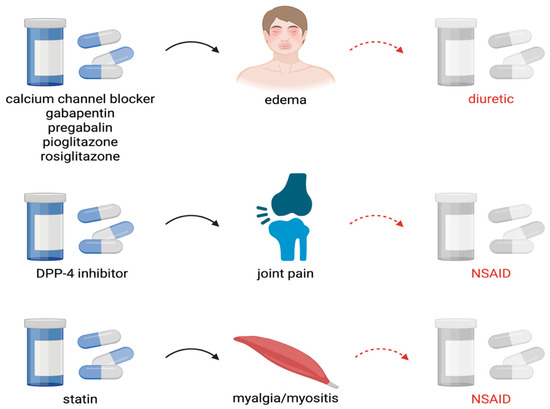
The article outlines how instead of looking at medications as the cause of symptoms, we often add more medications to treat the medication induced symptoms. Here is an example of how we get to polypharmacy in older patients
Body armor/ bullet resistant vests used by law enforcement are designed to stop penetration by handgun rounds. These rounds have less velocity than rifle rounds. When caring for someone who has been shot while wearing body armor, verify no penetration has occurred and then look for blunt injuries such as rib fractures, liver injuries, pneumothorax, cardiac contusion, vertebral injury, etc. Behind Armor Blunt Trauma (BABT) is the technical term for injuries caused by the transfer of kinetic energy that occurs when these vests are struck.
This narrative review of the trauma literature looking at chronic pain after trauma found:
This German retrospective review of 1500 level one trauma center patients (ICU level or ISS over 9) found obesity was an independent predictor of ARDS, multisystem organ failure, and sepsis but not pneumonia or mortality.