Category: Orthopedics
Posted: 6/27/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Should patients with mild cognitive impaired take glucosamine for their knee pain?
Glucosamine is one of the most commonly used dietary supplements in the US.
It is an amino sugar. Made from glucose and the amino acid glutamine.
Approximately 5% of the general adult population reported using glucosamine in the prior week, with higher rates among older adults — up to 9% of elderly men and 7% of elderly women.
Several studies have investigated glucosamine use and risk of Alzheimer’s disease. This literature has suggested either no association or even a protective association (Zhou et al., 2023 & Zheng et al.2023).
A study published this month in Nature Metabolism found a different association.
The research team used AI to comb deidentified health records (65,000) in the University of Florida health system for patients diagnosed with either Alzheimer’s disease and related dementias (ADRD) or mild cognitive impairment (MCI).
24,000 patients with dementia and 41,000 with MCI.
They compared people who took glucosamine with those who didn’t.
Data collected from 2012 to 2024.
8% of both groups of patients reported taking glucosamine. They attempted to control for features such as age, sex and other demographics.
In those with MCI, glucosamine use was associated with a 25% higher likelihood of progression to dementia. There was no increased mortality in this group.
In the ADRD group, glucosamine was associated with a 25% increase in mortality risk (<5 years).
The study found no adverse effects on cognitively healthy adults
If true, these findings suggest that the danger of glucosamine supplementation is unique to the biological environment of an already vulnerable or diseased brain.
The mechanism suggested involves hyperglycosylation.
Glucosamine crosses the BBB and acts as a fuel source adding excessive sugar tagging to proteins thereby affecting proper protein functioning.
To further test this, researchers investigated normal mice or mice engineered with Alzheimer’s symptoms, Feeding glucosamine to the Alzheimer’s mice severely worsened their memory deficits. There was no effect on the healthy mice.
Interestingly, they then chemically blocked the sugar-tagging enzyme that makes sugars like glucosamine and this reversed the cognitive decline (improved dementia symptoms).
They then looked at post-mortem tissue samples of human Alzheimer’s brains and found they possessed a heavy, abnormal accumulation of these sugars as compared to healthy control brains.
As usual, this study needs to be further investigated in an ethically constructed interventional trial before firm conclusions can be made from this association
Hawkinson, T.R., Liu, Z., Ribas, R.A. et al. Hyperglycosylation is a metabolic driver of Alzheimer’s disease. Nat Metab 8, 1410–1425 (2026).
Category: Orthopedics
Posted: 6/13/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
You order repeat plain films of the leg again:
Patient returns to the ED for 3rd visit in the past 3 months for leg pain.
PMH of mid shaft fibular fracture 4 months prior.
Repeat radiographs in the ED shown.
Consider the diagnosis of Complex regional pain syndrome (CRPS)
Diagnosis:
Diagnose using the Budapest criteria
Sensitivity of 0.99 and Specificity of 0.68
1. Continuing pain, which is disproportionate to any inciting event
2. Must report at least one symptom in three of the four following categories:
3. Must display at least one sign at time of evaluation in two or more of the following categories:
4. There is no other diagnosis that better explains the signs and symptoms.
Prognosis:
Approximately 80% of patients have substantial improvement within 18 months after disease onset; however, later improvement is rare.
Goebel A. Complex Regional Pain Syndrome. N Engl J Med. 2025 Dec 11;393(23):2338-2348.
Category: Orthopedics
Posted: 5/23/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
20yo college swimmer presents to the ED with a constellation of non-specific symptoms such as poor sleep, fatigue, depression/anxiety, weight loss.
Despite regular 2/day practices, his coach tells him his performance is worse than ever.
Overtraining syndrome
A maladaptive response to excessive exercise without adequate functional rest
-Results in disturbances of multiple body systems (neurologic, endocrinologic, immunologic and psychologic) which causes a broad constellation of symptoms
- May be caused by systemic inflammation and resultant neurohormonal changes (hypothalamic-pituitary-adrenal axis)
- Multiple hypotheses exist
The ACSM 2025 consensus statement on the adolescent athlete highlights that overtraining risk is particularly elevated in those who specialize in a single sport early, train more hours per week than their age, or maintain a >2:1 ratio of organized sport to free play.
Symptoms
The ACSM/AMSSM consensus statement categorizes these into physical and psychosocial domains:
Physical symptoms:
Psychosocial symptoms:
Decreased maximal heart rate during exercise testing (-3.6 to -7.5 bpm) is the most consistent cardiovascular finding
ED workup may include: CBC, CMP, iron studies, TSH, CK.
The only treatment is reduction in training combined with optimized nutrition, increased sleep, and stress reduction. Subsequent improvement in symptoms and performance confirms the diagnosis but may take months depending on the severity and duration of maladaptation.
Category: Orthopedics
Posted: 5/9/2026 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
How much do you trust your plain film in the evaluation of elderly patients with traumatic hip pain?
A 2020 meta-analysis involving 3000 elderly patients investigated radiographically occult hip fractures.
The rate of surgical hip fracture was reported in each study.
MRI was used as the reference standard.
Mean age, 76.8 years ± 6.0.
The frequency of radiographically occult surgical hip fracture was 39% (1110 of 2835 patients)
The frequency of occult fracture was higher in 3 groups of patients:
Aged at least 80 years
Those with an equivocal radiographic report
Those with a history of trauma
Haj-Mirzaian A,et al. Use of Advanced Imaging for Radiographically Occult Hip Fracture in Elderly Patients: A Systematic Review and Meta-Analysis. Radiology. 2020 Sep;296(3):521-531.
Category: Orthopedics
Posted: 4/11/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
What elements of the history are most helpful for diagnosing a concussion?
An estimated 1.1 million to 1.9 million pediatric concussions occur annually in the US.
OBJECTIVE: To determine the accuracy of clinical history for identifying concussion in children and adolescents.
While most children recover within 4 weeks, approximately 30% experience persistent symptoms beyond 28 days.
Early evaluation and timely management are associated with improved recovery—athletes who immediately reported their injury experienced almost five and half fewer days of symptoms compared to those who delayed reporting.
Key Diagnostic Findings
The review identified the most diagnostically useful symptoms (by likelihood ratio):
| Finding | Likelihood Ratio (LR+) | Specificity |
|---|---|---|
| Mental fog | 11.8–12.0 | 0.96 |
| Noise sensitivity | 6.9 | 0.94 |
| Nausea | 6.7 | 0.93 |
| Light sensitivity | 6.4 | 0.93 |
| Headache | 3.1 | 0.74 |
The ABSENCE of headache was the only finding that substantially reduced the likelihood of concussion (LR, 0.20; sensitivity, 0.86)
Shah SN, Chizuk HM, Fong H, Hannon M, Mannix RC. Does This Child Have a Concussion? The Rational Clinical Examination Systematic Review. JAMA.
Published online April 06, 2026.
Category: Orthopedics
Posted: 3/28/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
https://prod-images-static.radiopaedia.org/images/52314030/8089eeb717fd6d20e108ec2e586ba4.jpg
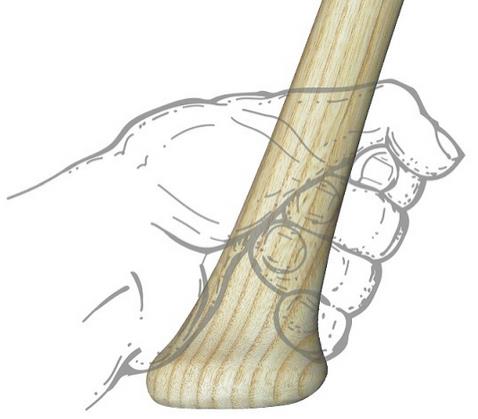
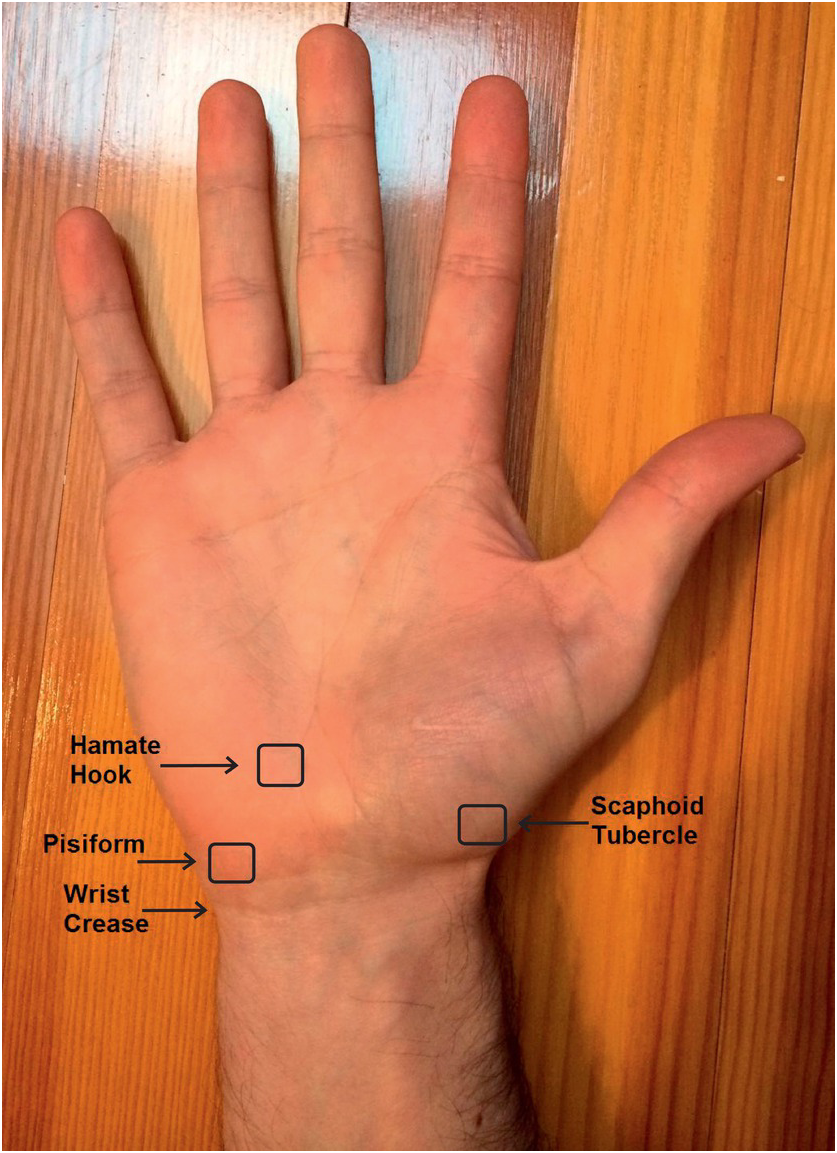
Hamate Fractures:
Rare (2 to 4% of all carpal fractures)
Mechanism: Usually a direct blow from a stick sport (bat, club or racket)
Have increased suspicion in these athletes who present w/ ulnar sided wrist pain
Presents with hypothenar pain and pain with gripping activities
Fractures occur in two locations: the body and the hook of the hamate
On exam you will find:
Hook of Hamate Pull Test
Examiner places the wrist in full ulnar deviation with the fingers flexed.
Examiner pulls on the ring and pinky finger with the patient resisting the pull.
Positive test
Diagnosis:
Category: Orthopedics
Posted: 3/14/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
https://upload.orthobullets.com/topic/322147/images/dorsal_cortical_lateral_pooping_duck..jpg
Triquetrum fracture
The commonly missed ulnar wrist injury
2nd most common carpal bone fracture (15-18 % of all fractures)
Tender just distal to the ulna
X-ray findings are subtle and frequently missed
In one series, only 20% were visualized on plain film!
When seen, most often on the lateral view
Seen as a chip fracture of unclear donor site
Also, one of my favorite named radiologic findings!
https://pbs.twimg.com/media/FskPCbnWYBEk8H2.jpg
Nonsurgical management is indicated for most triquetral fractures.
Volar splint and follow up with hand surgery.
Category: Orthopedics
Posted: 2/28/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Rotational Injury to the Knee
The plain film shows a small, crescent shaped bone fragment adjacent to the lateral tibial plateau.
This fracture is called a Segond fracture
It represents a bony avulsion of the anterolateral ligament (ALL) NOT the ACL
However, this fracture pattern is associated with a tear of the ACL tear 75-100% of the time.
Also associated with meniscal injuries (65-75%)
The ALL runs from the lateral femoral condyle and inserts on the anterolateral proximal tibia near the fibular head
The ALL helps to control tibia internal rotation
Works in concert with the ACL to prevent anterior rotational tibia subluxation
This injury pattern on plain film indicates a significant ligament injury and changes management because ACL reconstruction is often required.
Category: Orthopedics
Keywords: arthrocentesis, septic arthritis (PubMed Search)
Posted: 2/14/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
BOTTOM LINE: Modify WBC threshold for diagnosing septic arthritis is patients who received recent antibiotics (24h to 2 weeks).
The ISDA 2024 guidelines use a WBC synovial fluid count of greater than 50,000 cells/mm to suggest septic arthritis.
A study of 81 patients with culture proven septic arthritis found the average leukocyte count was 40,408 ± 29,433 cells/µL in those who received antibiotics prior to arthrocentesis vs 93,824 ± 73,875 cells/µL in those who received no antibiotics for two weeks prior.
This is a greater than 50% reduction in mean WBC count!
A retrospective study of 383 patients found that patients who received IV or oral abx within 2 weeks before arthrocentesis had an optimal synovial WBC cutoff of > 16,000 (sensitivity 82%, specificity 76%), compared to >33,000 cells/µL (sensitivity 96%, specificity 95%) in the control group who had not received antibiotics within 2 weeks.
Conclusion:
When a patient has received antibiotics before arthrocentesis, a diagnostic value of >16,000 synovial leukocytes may be considered to guide treatment of septic arthritis. Additionally, in this one study, a diagnostic value of >33,000 synovial WBCs yields the highest accuracy for diagnosis of septic arthritis in patients who have not been given antibiotics before arthrocentesis.
Massey PA, et al. Optimal Synovial Fluid Leukocyte Count Cutoff for Diagnosing Native Joint Septic Arthritis After Antibiotics: A Receiver Operating Characteristic Analysis of Accuracy. The Journal of the American Academy of Orthopaedic Surgeons. 2021.
Category: Orthopedics
Posted: 1/24/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
The recommended approach for patients with suspected septic arthritis is arthrocentesis with fluid analysis sent for: Gram stain, culture, WBC count with differential, and crystal analysis before starting antibiotics.
From a classic meta-analysis of 14 studies involving greater than 6,000 patients the only 3 findings that occur in more than 50% of patients with septic arthritis were
Joint pain (sensitivity, 85%; 95% confidence interval [CI], 78%-90%),
Joint swelling (sensitivity, 78%; 95% CI, 71%-85%),
Fever (sensitivity, 57%; 95% CI, 52%-62%).
Vs.
Sweats (sensitivity, 27%; 95% CI, 20%-34%)
and rigors (sensitivity, 19%; 95% CI, 15%-24%) were less common findings in septic arthritis.
The probability of septic arthritis increases progressively with higher synovial WBC counts:
PMN percentage ?90% suggests septic arthritis with LR 3.4 (95% CI, 2.8-4.2)
VS
PMN <90% lowers the likelihood (LR 0.34, 95% CI 0.25-0.47).
Margaretten ME, Kohlwes J, Moore D, Bent S. Does This Adult Patient Have Septic Arthritis? JAMA. 2007;297(13):1478-88.
Category: Administration
Posted: 1/10/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Plain films are often the first imaging test ordered in patient’s with knee injuries.
Plain films do NOT directly show the ACL but may reveal indirect signs of an ACL tear.
Key Plain Film Findings:
1) Effusion
ACL injury generates a large joint effusion (swelling/hemarthrosis). The presence of a fat/fluid interface (lipohemarthrosis) suggests associated bone injury.
This may be seen as joint fluid on the plain film lateral view. This view is best obtained with the patient in the supine position. This allows a layering of fluid in the suprapatellar bursa. A fat/fluid level indicates the presence of a lipohemarthrosis, signifying the likelihood of an intraarticular fracture.
http://radiologykey.com/wp-content/uploads/2019/03/f10-02ad-9781437727791.jpg
( A ) The normal suprapatellar bursa is seen on the lateral view as a line extending obliquely anterior and superior from the superior/posterior surface of the patella to the posterior surface of the quadriceps tendon.
(B) A small to moderate-sized effusion.
(C) A larger effusion.
In (D) the quadriceps tendon is bulged outward by an even larger joint effusion.
In the correct clinical setting, the presence or absence of a new fusion can be highly suggestive of ACL tear. Effusion can usually accurately be assessed on both physical exam and the lateral plain film. The absence of a knee effusion makes acute tear of the ACL unlikely as clinical practice suggests a rapidly developing hemarthrosis. Effusion of the knee may be associated with other entities such as intraarticular fracture or underlying arthritis. Typically, patients with acute ACL tears are young and do not have chronic infusions. Most acute meniscal tears and chondral injuries do not develop acute large effusions due to lack of significant vascularity.
Category: Orthopedics
Posted: 1/10/2026 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Plain films are often the first imaging test ordered in patient’s with knee injuries.
Plain films do NOT directly show the ACL but may reveal indirect signs of an ACL tear.
Key Plain Film Findings:
1) Effusion
ACL injury generates a large joint effusion (swelling/hemarthrosis). The presence of a fat/fluid interface (lipohemarthrosis) suggests associated bone injury.
This may be seen as joint fluid on the plain film lateral view. This view is best obtained with the patient in the supine position. This allows a layering of fluid in the suprapatellar bursa. A fat/fluid level indicates the presence of a lipohemarthrosis, signifying the likelihood of an intraarticular fracture.
http://radiologykey.com/wp-content/uploads/2019/03/f10-01ae-9781437727791.jpg
( A ) The normal suprapatellar bursa is seen on the lateral view as a line extending obliquely anterior and superior from the superior/posterior surface of the patella to the posterior surface of the quadriceps tendon.
(B) A small to moderate-sized effusion.
(C) A larger effusion.
In (D) the quadriceps tendon is bulged outward by an even larger joint effusion.
In the correct clinical setting, the presence or absence of a new fusion can be highly suggestive of ACL tear. Effusion can usually accurately be assessed on both physical exam and the lateral plain film. The absence of a knee effusion makes acute tear of the ACL unlikely as clinical practice suggests a rapidly developing hemarthrosis. Effusion of the knee may be associated with other entities such as intraarticular fracture or underlying arthritis. Typically, patients with acute ACL tears are young and do not have chronic infusions. Most acute meniscal tears and chondral injuries do not develop acute large effusions due to lack of significant vascularity.
Category: Orthopedics
Posted: 12/13/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Midshaft Clavicle Fractures
Have been in the sports headlines over the last several months
http://www.orthopaedicsone.com/wp-content/uploads/2024/06/379191373.png
About 3 - 3.5% of all adult fractures
Typical patient is young and active, usually males < 30 years old
Most clavicle fractures (up to 80%) involve the middle third
Mechanism: Typically direct impact or FOOSH
“S” shaped bone with thinnest & narrowest segment at junction between middle and distal third
Appearance: 2/3 non-displaced
Displaced fractures
Because of the effects of gravity, attempt to get clavicle series in upright position
Otherwise supine view may underestimate degree of displacement
What to look for on plain film
Displacement
Category: Orthopedics
Posted: 11/22/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Turf Toe:
Increased recent attention due to injuries in high profile athletes
Sprain of the first MTP joint
Mechanism: Forced hyperextension of the great toe (most common)
https://briandorfman.com/wp-content/uploads/2015/11/b_12_3_6a.jpg
Causes injury to the MTP joint capsule and surrounding ligaments
Presents as pain, swelling, discoloration, tenderness to palpation, possible joint laxity
Pain with active and passive ROM (both flexion and extension)
Graded 1-3 (Sprain, partial rupture, significant/complete rupture)
Most commonly seen in athletes who compete on artificial turf.
More rigid than natural grass
Synthetic surfaces do not release cleats as easily as natural grass
Improved synthetic surfaces perform more similar to natural grass
Much higher incidence in games vs practices.
In football, quarterbacks and running backs at highest risk
Between 30 and 45% of professional football players claim that they have experienced a turf toe injury, with over 80% of those injuries occurring on artificial turf
The combination of more rigid synthetic surfaces and lighter, more flexible shoes, increase risk of hyperextension injuries
Treatment: usually non operative
Rest/ice/taping after acute swelling decreased/stiff sole shoe/crutches/NSAIDs.
Consider walking boot or short leg splint for severe injuries
Less than 2% of injuries require surgery
Category: Orthopedics
Posted: 11/8/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Chondrocalcinosis is a condition where calcium pyrophosphate crystals form in the joints (particularly the knee and wrist), leading to inflammation and pain.
Appears as a cloudlike radiopacity in the knee’s articular cartilage and meniscus on XR, reflecting abnormal calcium-based crystal deposition.
This can be distinguished from the radiolucent appearance of monosodium urate crystals of gout.
https://www.wikidoc.org/index.php/File:MSUandCPPD.png
These calcium crystals are common in end-stage knee osteoarthritis and have been associated with disease severity.
Due to this well-observed coexistence (chondrocalcinosis and knee osteoarthritis), chondrocalcinosis is commonly considered a manifestation of osteoarthritis pathology.
However, this does not explain the commonly encountered instances where chondrocalcinosis appears in radiographically normal knees. This raises questions of whether chondrocalcinosis is a cause or merely a consequence of end-stage osteoarthritis.
Population studies have identified that about 6.% of individuals have chondrocalcinosis in joints unaffected by osteoarthritis
In a recent analysis including more than 6400 middle-aged to older adults, individuals with knee chondrocalcinosis were 75% more likely to develop knee OA than those without the condition at baseline.
Chondrocalcinosis may contribute to the risk of osteoarthritis through inflammation. These deposited crystals could induce the production of inflammation markers, matrix-degrading enzymes and induce chondrocyte hypertrophy or chondrocyte death. These effects not only damage the joint but also form a positive feedback loop to produce more calcium crystals.
Individuals with chondrocalcinosis may represent a specific subgroup of patients, for which a treatment targeting chondrocalcinosis induced inflammation may present a viable strategy to prevent osteoarthritis in this patient subgroup.
This idea has some support from the 2023, LoDoCo2 trial, (approx. 5500 patients) which showed an association between the use of colchicine, 0.5 mg daily, with a lower incidence of total knee and total hip replacements.
Wu Y, Liew JW, et al. Chondrocalcinosis and incident knee osteoarthritis: findings from 2 large prospective cohorts with 20 years of follow-up. Ann Rheum Dis. 2025 Oct;84(10):1743-1751.
Category: Orthopedics
Posted: 10/25/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Low-Dose Radiation Therapy for Osteoarthritis
Current options for osteoarthritis include NSAIDs, physical therapy, intraarticular steroid injections, and lifestyle modifications, such as weight loss and exercise. After these options have been exhausted, there is joint replacement.
Problems with these options in older patients are that about 25% of all patients will not respond to these therapies or lose their responsiveness over time. NSAIDs also may not be great options in those with renal impairment and increased risk of GI bleeding.
Conventional radiation therapy (RT) in the treatment of malignant disorders relies on its antiproliferative effects. Alternatively, at doses of less than 1 Gray, RT has been shown to have strong anti-inflammatory effects.
RT may be an appropriate option for those with OA who have failed other conservative measures but are not ready for joint replacement…ideally before the onset of bone-on-bone changes at which point RT is less likely to be effective.
Appropriate candidates are older than 50 years. Patients do not typically experience acute side effects. There may be slight redness, milder than a sunburn, on the skin of the area radiated. Malignancy induced by RT treatment remains a small theoretical risk and is mitigated by selection of non central joints (i.e. not for spine OA).
The most commonly treated joints include hands, feet, knees, and elbows.
Pain relief can last from several months to years, with studies reporting that 30%-60% of patients maintain significant pain reduction 1-2 years after treatment. In one study, patients reported 85% decreased use of analgesic medications.
Typical treatment regimens involve 6 sessions of 0.5 Gy each conducted 2-3 times per week.
RT may be an effective modality for patients who have failed conventional treatment and are either not ready for surgery or are poor surgical candidates.
The Use of Low-Dose Radiation Therapy in Osteoarthritis: A Review
Dove, Austin P.H. et al. International Journal of Radiation Oncology, Biology, Physics, Volume 114, Issue 2, 203 - 220
Category: Orthopedics
Posted: 10/11/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Use of Muscle Relaxants in the Elderly
A recent pearl discussed the risks of skeletal muscle relaxants (SMR) in the elderly population.
Risks included sedation, confusion, disorientation, orthostatic hypotension and increased risk for falls and fractures.
The Beers Criteria is a list of medications that older adults should generally avoid due to potential adverse effects.
Two commonly used muscle relaxants, Baclofen and Tizanidine (Zanaflex) are not included in the Beers criterion.
A study published last month investigated the safety profile of these medicines as compared to cyclobenzaprine (Flexeril).
Retrospective cohort study of Kaiser Permanente Southern California patients aged 65 to 99 years between 2008 and 2018.
From a population of approximately 88,000 participants (mean age 71.4 years; 59.8% women), approximately 118,000 study medication episodes were identified: 54.8% participants were dispensed baclofen, 6.3% tizanidine, and 38.9% cyclobenzaprine
Outcomes included injury-related hospitalizations, emergency department visits, and urgent care visits documented in EMR and identified through diagnostic codes for fractures, falls leading to fractures, brain injuries, and dislocation injuries
Compared with cyclobenzaprine, Baclofen demonstrated a 69% greater risk (adjusted Hazard Ratio 1.69, [95% CI 1.51-1.88]) and tizanidine carried a 34% greater risk (adjusted Hazard Ratio 1.34, [95% CI 1.11-1.62]) for composite injury outcomes.
Conclusion: Older adult patients prescribed baclofen or tizanidine have an increased risk of injury when compared with Flexeril (currently included on the Beers Criteria)
George MM, et al. Safety of Baclofen and Tizanidine in Older Adults: A Retrospective Cohort Study in a Large Integrated Health Care System. J Am Geriatr Soc. 2025 Sep 13
Category: Orthopedics
Posted: 9/27/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Use of Muscle Relaxants in the Elderly
A 2023 Cochrane Database review found moderate-certainty evidence that muscle relaxants may increase the risk of adverse events.
Primary adverse events are due to CNS depressant effects (dizziness, sedation) and anticholinergic effects.
Geriatric patients already have baseline unsteady gait, decreased coordination and cognitive changes.
A 2015 study showed that geriatric patients who took muscle relaxants were 2.25 times more likely to visit the ED for a fall or fracture and 1.5 times more likely to be hospitalized for a fall or fracture than patients who did not take these medications.
Risk is greatest in patients >65 years of age. This population was 1.32 times more likely to have an injury compared to patients who did not take skeletal muscle relaxants.
Alvarez CA, et al. Association of skeletal muscle relaxers and antihistamines on mortality, hospitalizations, and emergency department visits in elderly patients: a nationwide retrospective cohort study. BMC Geriatr. 2015;15:2.
Category: Orthopedics
Posted: 9/13/2025 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Epidural abscess
Likely the most serious missed emergent condition in patients diagnosed with non-specific back pain.
Challenging diagnosis to make in the ED
Almost half of patients are initially misdiagnosed and average two ED visits before the diagnosis is made.
At the time of diagnosis, the most common symptom is diffuse spine pain and the most common exam finding is severe local spinal tenderness.
Fever is only present in 30% to 50% of patients at presentation.
In one study, over 65% of patients with spinal epidural abscesses were afebrile on presentation.
Also, consider that the neurological examination is normal in two-thirds of patients at their first ED visit.
Category: Orthopedics
Posted: 8/9/2025 by Brian Corwell, MD
(Updated: 6/27/2026)
Click here to contact Brian Corwell, MD
Scaphoid fractures
Make up almost 2/3rds of all carpal fractures
Fractures tend to be localized to 3 anatomic locations
Waist fractures make up 2/3rds. This may be diagnosed with anatomic snuffbox tenderness
Proximal pole fractures make up approximately 25%. This may be diagnosed with bone tenderness about a fingerbreadth distal to Lister’s tubercle
Distal fractures make up the remaining 10%. This may be diagnosed with tenderness at the volar prominence of the distal wrist crease
Imaging:
In addition to standard views of the wrist (PA/lateral/oblique) consider adding a scaphoid view. This imaging view is a PA film taken with the wrist in full pronation and ulnar deviation. This allows full visualization of scaphoid in its longitudinal axis. Also, this allows visualization of the area in question without the annoying overlap of adjacent carpal shadows
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}