The first step toward developing a healthy ED is to develop a vision of the way emergency medicine should be practiced. The second is to analyze the way it is practiced within a physician group or department. The third is to generate a plan for transitioning from the way it is to the way it ought to be.
A robust department begins with principled physician and nursing leadership.
- Laura Pimentel, The Healthy Emergency Department, in Croskerry P, Cosby KS, Schenkel SM, Wears RL (editors), Patient Safety in Emergency Medicine, Wolters Kluwer, Philadelphia, PA, 2009; 41-44.
A mentor, a colleague, a leader, and a friend, Dr. Laura Pimentel died on June 23, 2026. She led the Emergency Departments at Bon Secours (1993-94), Mercy Medical Center (1995-2007), and Upper Chesapeake Medical Center (2007-08). She was Vice President and then CEO of the Maryland Emergency Medicine Network and, from 2011-2013, President of Maryland ACEP. She will be greatly missed. Her legacy of caring and clarity live on.
This study found that of all 283 EM residencies in the US, only 4% listed pronouns on resident webpages, 3% had LGBT+ dedicated sections of their website, and only 31% had DEI sections of the website at all.
In the post COVID era of residency interviews, the programs' websites become a vital source of information for the applicants. There is still a large gap in the visibility of the LGBTQIA+ population in the majority of program websites.
This single center prospective study asked residents to determine if their patient had barriers to post ED discharge health care such as having a PCP, transportation issues, affording medications, and need for assistance with activities of daily living. They then compared the physicians’ answers to patient’s answers and found: “Physicians had poor sensitivity for accurate identification of patient barriers.”
Some of our discharged patients are struggling more than we realize.
A recently published commentary highlights the importance of looking beyond the numbers and remembering the core mission of emergency practice. It warns against “gaming” the system to create processes that give better metrics using the example of rates of patients who leave without being seen (LWBS). In the author’s words, efforts aimed at improving this metric create strategies that “raise concerns about distributive justice, beneficence, and professional integrity.” See link for key take home points.
This is a small qualitative study that focused on barriers to care and how to overcome them when dealing with patients with dementia, who are primarily Spanish speaking. The authors found to big themes that patients and caretakers thought would improve their care:
1- use of a certified translator, either telephonically or in person, eased social dynamics in communication
2- those same translators tended to only be used in an episodic manner- during HPI, exlaining results or discharge planning. But the patients and caretakers would prefer to have access to them in the “in between” periods so that it would be a more patient centered experience
Ambient Artificial Intelligence based scribes that create visit notes based on the conversation in the room during patient evaluation may save documentation time and reduce total time in the health record but may not perform as well as human scribes in some circumstances, at least for pediatric patient charts.
Multiple past studies have shown that Black and female patients tend to be prescribed fewer opioids than White and male patients. This study looked at the rates of opioid usage post RSI.
They found that while Black patients received opioids at a higher rate, they were given lower doses than white patients. Older patients were less likely to receive opioids post RSI than younger patients. They did not find a difference in rates of opioid usage between genders, but female patients received lower doses of opioids overall.
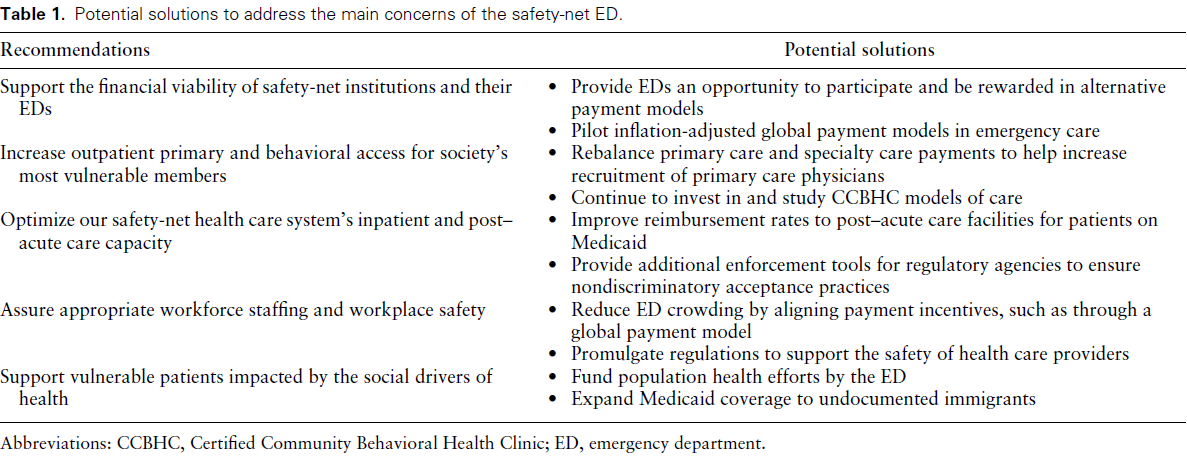
Bottom Line: Safety-net hospitals are those that see a substantial share of uninsured, Medicaid, or low-income Medicare patients. Their emergency departments (EDs) deliver disproportionally more undercompensated and uncompensated care, yet have similar operating costs as other EDs. Authors convened a group of 15 administrators of academic safety net EDs to identify and
develop a consensus understanding of barriers to delivering optimal care. See the link for details of their conclusions.
Educational Pearls for the ED:
Many Muslim patients with diabetes will fast despite medical advice. Studies show a significant number continue fasting even when they are considered high risk.
Key medical risks during Ramadan fasting include:
- Hypoglycemia
- Hyperglycemia and diabetic ketoacidosis
- Dehydration
- Medication nonadherence or altered dosing schedules
BOTTOM LINE: ED Boarding is now publicly reported in one state (Connecticut). Public reporting of boarding data may encourage new approaches to remedy the problem.
Bottom line: Good news! In 2022 and 2023, at ACEP, SAEM and AAEM, invited speakers were evenly split 50/50 women and men (with a small percentage nonbinary) showing no significant gender bias toward speaker invitation.
How well does your ED care team communicate? For some high yield strategies and reasons for improvement, read on…
To explore effective and ineffective communication in the ED and its impact of patient care, physician and nurses from several academic EDs completed an online anonymous survey, then attended focus group sessions. Responses highlighted the following themes:
1: Situations, built physical environment, and medium of communications all impact quality of communication.
2: Core elements of desired professional communication include respect, closed-loop communication, and attention, often conveyed through non-verbal behaviors.
3: Poor communication begets poor communication in later interactions
4: Effective communication is seen as fundamental to patient care but also has impacts beyond patient care
5: Clinician gender and gender dyads influence communication dynamics, age and experience dyads did not.
Do any of these themes resonate with you? What can you do within your department to improve physician-nurse communication and the care you provide?
Plain films are often the first imaging test ordered in patient’s with knee injuries.
Plain films do NOT directly show the ACL but may reveal indirect signs of an ACL tear.
Key Plain Film Findings:
1) Effusion
ACL injury generates a large joint effusion (swelling/hemarthrosis). The presence of a fat/fluid interface (lipohemarthrosis) suggests associated bone injury.
This may be seen as joint fluid on the plain film lateral view. This view is best obtained with the patient in the supine position. This allows a layering of fluid in the suprapatellar bursa. A fat/fluid level indicates the presence of a lipohemarthrosis, signifying the likelihood of an intraarticular fracture.
http://radiologykey.com/wp-content/uploads/2019/03/f10-02ad-9781437727791.jpg
( A ) The normal suprapatellar bursa is seen on the lateral view as a line extending obliquely anterior and superior from the superior/posterior surface of the patella to the posterior surface of the quadriceps tendon.
(B) A small to moderate-sized effusion.
(C) A larger effusion.
In (D) the quadriceps tendon is bulged outward by an even larger joint effusion.
In the correct clinical setting, the presence or absence of a new fusion can be highly suggestive of ACL tear. Effusion can usually accurately be assessed on both physical exam and the lateral plain film. The absence of a knee effusion makes acute tear of the ACL unlikely as clinical practice suggests a rapidly developing hemarthrosis. Effusion of the knee may be associated with other entities such as intraarticular fracture or underlying arthritis. Typically, patients with acute ACL tears are young and do not have chronic infusions. Most acute meniscal tears and chondral injuries do not develop acute large effusions due to lack of significant vascularity.
This study looked at industry sponsored payments to EM physician through non-covered entities (ie not directly to physician or through an academic institution). It found a $100 million increase from 2015-23 in this payment model. It appears that private equity is not the only money entering emergency medicine in the past decade.
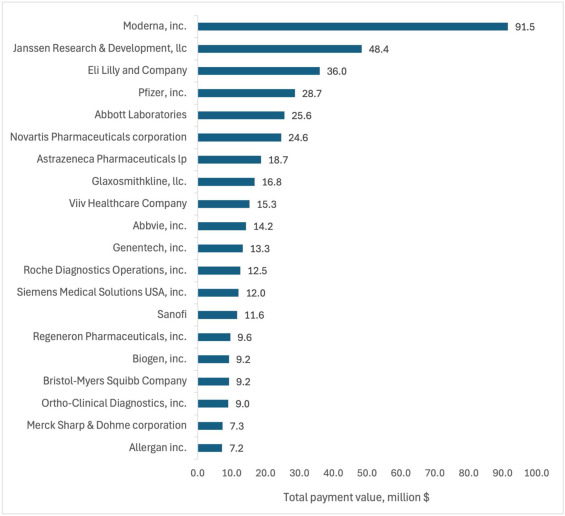
Total value of Industry-Sponsored Research Payments (ISRPs) by company. The 20 companies with highest total ISRPs awarded to emergency physician PIs.
How do ED volumes change around the winter holidays?
The anticipated US pattern is one of lower volumes on the holidays themselves followed by increased volumes on the first weekdays after.
Behavioral health visits show similar patterns – a drop before the holidays and perhaps an increase after the holiday.
Many departments adjust scheduling accordingly, reducing staff on major holidays, which has the added benefit of allowing more people to enjoy the holiday.
This pattern isn’t necessarily what happens everywhere, though. At least one Australian ED reported increased visits over the holidays.
While not perfect, the best guide to future holiday volumes remains past experience thoughtfully applied.
This study looked for differences in prescribing patterns of suboxone for different opioid related complaints- withdrawal, overdose, and other related complaints.
In the overall cohort, all racial minorities, except Native American, and female patients had a lower likelihood of being prescribed suboxone for any opioid related complaint compared to white, male patients.
However, when they did subgroup analysis, patients presented for withdrawal symptoms had increased rates of buprenorphrine administration and prescribing that eliminated the racial disparities, but the gender disparities remained.
MOUD remain a key factor in allowing patients with OUD to achieve long-term sobriety, but there are still persistent barriers to appropriate prescribing
Food for thought on this Thanksgiving eve…
AI is rapidly being integrated into the practice of emergency medicine, as well as many other medical specialties. Similar to the adage, "you are what you eat," AI is what we feed it. See below for an introduction to the various levels of bias contributing to the machine learning process:
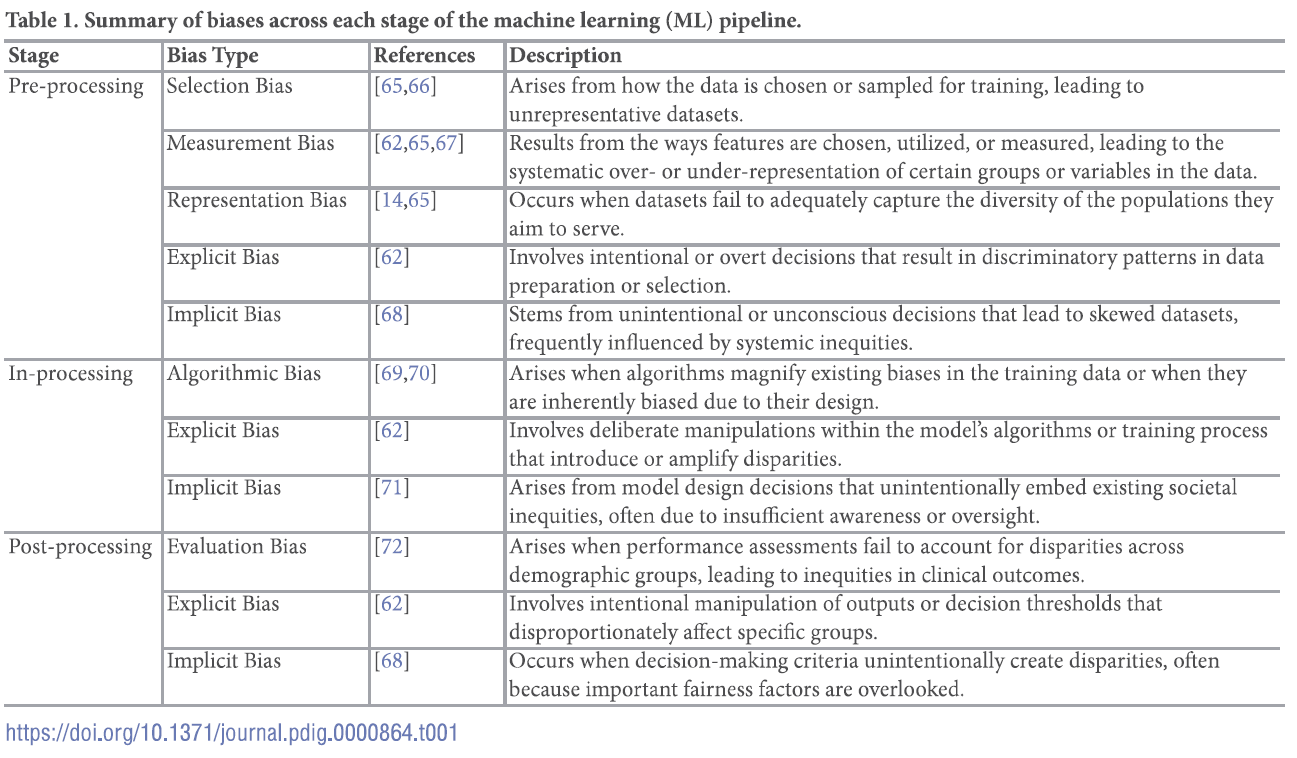
For a deep dive into the world of bias in AI, see referenced article.
This abstract from ACEP's most recent research forum looked at the effect a patient's preferred language had on ED LOS, rate of admission, hospital length of stay and resource utilization both in the ED and the hospital.
Overall, those patients who spoke English as their primary language had lower ED LOS, less testing done in the ED, but if they got admitted they had the longest hospital LOS. Patients who preferred Spanish language had the shortest hospital LOS and were most likely to be discharged home with no services. Non-English/non-Spanish languages had the longest ED LOS and highest admission rates and had similar resource use as patients who preferred Spanish
This abstract opens the door for further research into what the underlying cause of these disparities are.
Do you ever have to manage a complaint? Perhaps a patient complaint?
It can be tough to hear a complaint. Emotions can run high. And then the ability to listen and respond can fade.
It helps to have a shorthand to guide the response.
Customer service literature provides one that often works well: LAST, for Listen, Apologize, Solve, and Thank.
This article gets at the basic idea (while adding one or two additional items): Steinman, HK. A Method for Working with Displeased Patients—Blast. J Clin Aesthet Dermatol. 2013 Mar;6(3):25–28. https://pmc.ncbi.nlm.nih.gov/articles/PMC3613270/.
This publication is a retrospective cross-sectional study conducted based on data collected during January 1–December 31, 2019 from a large, academic ED in the Southeastern US with the following research questions and results:
Interesting point regarding how disposition decisions are different from the ample evidence on disparities within triage decisions: The presence of disparities in disposition decisions is noteworthy not only because of their potentially long-term effects on patients’ health, but also because unlike some of the other decisions made in the ED such as triage, they are typically made under relatively less time pressure with deliberation and input from multiple individuals, conditions that are known to make biases less likely.
Authors propose pursing further research to elucidate the factors that contribute to these findings, instituting systems to alert providers in real time to the presence of conditions that could exacerbate disparities in ED care, and including the measurement of disparities along sex, race and ethnicity into health care operations data.
{kind=link}