Lactational mastitis (inflammation of the breast in individuals who are lactating) affects up to 20% of breastfeeding individuals. It is characterized by localized breast pain with erythema, edema, and systemic symptoms such as fever/chills and malaise. Supportive treatment measures include the use of NSAIDS, heat and/or ice, and continued feeding or emptying of the breast (stagnant milk can allow for progression of infection). If there is no response to supportive measures within 24 hours, pursuing antibiotic therapy is appropriate. Staphylococcus and Streptococcus species are common organisms responsible for bacterial mastitis; first-line treatment options include Dicloxacillin 500 mg QID or Cephalexin 500 mg QID for 10-14 days. If there is a concern for MRSA, Clindamycin or Bactrim may be used but are considered second-line. Bactrim should be avoided in breastfeeding individuals with infants <1 month or infants who are jaundiced or premature.
Complications of mastitis can include early termination of breastfeeding, breast abscess, and systemic infection if untreated. Ultrasound can be used to assess for breast abscess in patients who do not respond appropriately to antibiotics.
A cut-off of 35mm on CT scan has been shown to be predictive of which traumatic pneumothoracies require thoracostomy tube placement vs. safety of observation. This retrospective study looked at chest X-ray findings to see if there was a similar size cut-off where patients could be safely observed rather than undergo this invasive procedure. They found 38mm was the size over which observation failed. Of note, lactic acidosis and need for supplemental oxygen also predicted the need for chest tube placement
POCUS for DVT is a tricky examination.
Exam of positive study on transverse:
Longitudinal Image showing clot:
![]()
In this prospective, observational study of trauma patients with isolated head trauma, 62% of patients developed post-intubation hypotension. Comparing patients receiving hypertonic saline, vasopressors, crystalloid, or blood those receiving hypertonic saline and vasopressors had less post-intubation hypotension.
TBI patients who develop hypotension have worse outcomes. This study reminds us the use of vasopressors in trauma patients to maintain blood pressure is appropriate in the correct circumstances.
The Infectious Disease Society of America in 2023 recommended a single dose of an aminoglycoside for uncomplicated cystitis treatment in those with resistance or other contraindications to first line oral agents who were otherwise well enough to be discharged. This very small study (13 participants) suggest this strategy works for complicated (“male sex, urinary flow obstruction, renal failure or transplantation, urinary retention, or indwelling catheters”) cystitis patients who could otherwise be discharged home.
What is the best provocative test for the diagnosis of carpal tunnel syndrome?
A 2022 study included 37 observational studies to assess the diagnostic accuracy of these provocative maneuvers.
Meta-analysis totaling 2662 wrists of patients with carpal tunnel syndrome.
Surprisingly, the winner was a test that is less familiar to some of us who were taught the traditional tests such as the Phalen test, Tinel test or the carpal tunnel compression test.
Hand elevation has been known to reproduce the symptoms of carpal tunnel syndrome.
The hand elevation test demonstrated the best clinical performance for the diagnosis of carpal tunnel syndrome.
The beauty of the test is that it is as simple to perform as the name suggests.
Have the patient raise their hands above their head for one minute.
Hands are raised actively and without strain, keeping the elbows and shoulders relatively loose. That’s it!
A positive test reproduces the symptoms of carpal tunnel syndrome
The hand elevation test has a high sensitivity (75%-86%) and specificity (89%-98.5%)
Take home: Consider adding this bedside provocative test as the first screening test for patients with suspected carpal tunnel syndrome
Free Biostatistics Software Options
EpiCalc 2000 – available for Windows. Capabilities include sample size calculation, inferential statistics (p values, 95% CI), simple stratified analysis, paired and independent analyses. Right clicking allows you to do many things. (http://www.brixtonhealth.com/epicalc.html). I've had the most experience with this one.
Epi Info – supported by CDC. Available for Windows and for hand-held. (https://www.cdc.gov/epiinfo/index.html)
P/S – Power and Sample Size Calculation – available for Mac and Window. Supported by Vanderbilt biostatistics. (https://biostat.app.vumc.org/wiki/Main/PowerSampleSize)
Participation in meetings is an expected part of most (if not all) of our jobs. How many of these meetings are necessary? Could some of the “work” of meetings be accomplished with a few emails or other asynchronous forms of communication? Are meetings cluttering your schedule and making it impossible to get any real work done?
Some answers to these questions are offered in a Harvard Business Review article from March 2022.
Key points include:
Advantages to fewer meetings:
Authors recommend holding meetings only when “absolutely” necessary. That typically includes:
Do Sepsis Alert Systems Work?
Researchers in Korea completed a high quality systematic review and meta-analysis of sepsis alert systems for adult ED patients
Using high quality methods, they identified over 3000 studies with 22 meeting criteria.
They found these systems were associated with:
Electronic alerts were further associated with:
Summary (+ a little editorialization)
As annoying as we may find these systems in our daily practice, there is growing evidence that they do provide some benefit with impacts on task saturation and decreasing cognitive load in addition to real patient benefit. While there is also recent evidence that physician gestalt performs well against these systems, there is a suggested benefit in their inclusion in clinical decision making as a safety net or as an “assist”.
The incorporation of rule-based algorithms like these in more advance machine learning methods are covered quite well in a recent opinion piece on “The AI Future of Emergency Medicine”. However, it is important to always know the source of any “algorithm” that you are using, whether rule or mathematically based, given real concerns for bias and error.
Iron-deficiency anemia affects 10% of women of child-bearing age. Guidelines to treat iron deficiency recommend daily oral iron, but this may decrease fractional iron absorption and increase side effects which also impacts medication adherence. A double-masked, randomized, placebo-controlled trial, which included 150 women demonstrated that:
at equal total iron doses, compared to consecutive day dosing of iron, alternate day dosing did not result in higher serum ferritin but reduced iron deficiency at 6 months and triggered fewer gastrointestinal side effects.
Take home point: Dosing iron every other day had similar effect with less side effects. Consider prescribing it this way to your patients, especially if they have had issues with side effects in the past!
According to this study, no TXA 2g bolus was not found to increase the number of seizures in TBI pts.
TXA has been shown to improve mortality in inter cranial hemorrhage trauma patients if given within 2 hours. TXA is also known to lower seizure threshold. This study was a secondary analysis of a larger study comparing placebo to 1 g TXA bolus plus 8 hour infusion or 2g bolus TXA in the prehospital setting. There was no difference in the number of pts experiencing seizure or outcome in those receiving the 2g bolus of TXA.
Emergency department visits for pediatric mental health and behavioural concerns have been increasing. This study attempted to further characterize medications, both home and for sedation, that were given to these patients.
This study included 670,911 youth with a mental or behavioral health diagnosis over a 9 year inclusion period. The most common diagnses were depressive disorder, suicide or self injury and disruptive, impulse control and conduct disorder. During this time, a total of 12.3% of patients had a psychotropic medication given while in the ED. The percentage and odds of administering these medications increased from 7.9% in 2013 to 16.3% in 2022. Those with intellectual disability and autism spectrum disorder had the highest frequency of medication administration.
Bottom line: As mental health visits in pediatrics continue to increase along with boarding times, clinicians should become more familiar with psychotropic medications used in this population and become comfortable in making sure that these patients have their home medications and have a plan for chemical sedation if other areas of de escalation fail.
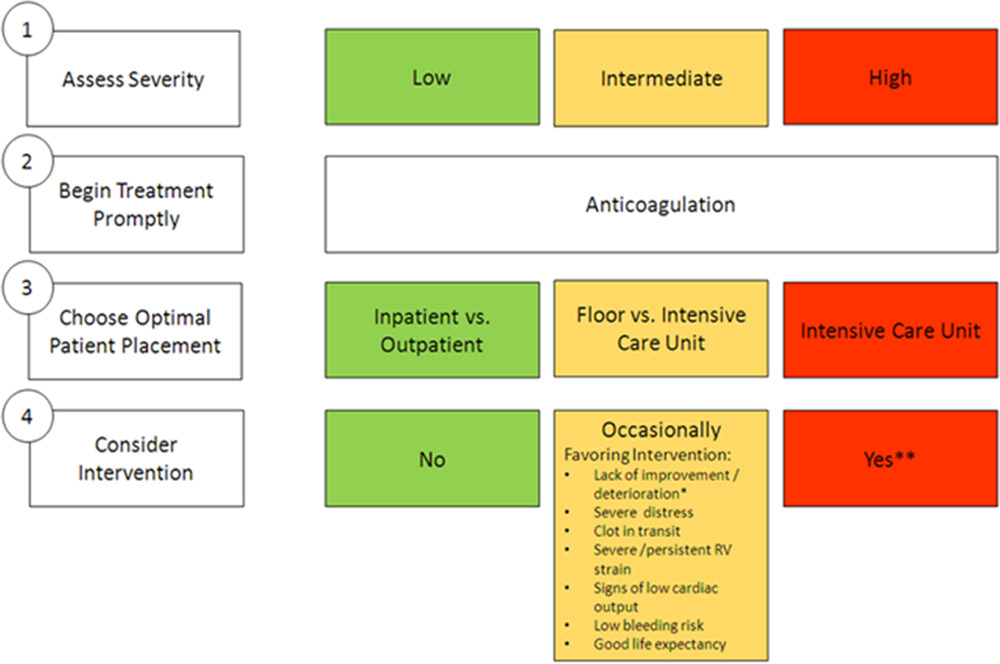
Deciding which pulmonary embolism patient needs thrombolytics/catheter based intervention is a shared decision among emergency physicians, intensivists, interventionalists, hospitalists, and the patient/family. This article provides evidence to help guide this decision. Keep in mind “The use of either CDL or catheter-based embolectomy in patients with intermediate-risk PE has, thus far, been correlated only with more rapid improvement of RV dysfunction than anticoagulation alone, not short- or long-term clinical or functional outcomes.”
"1. Massive (AHA) or high risk (ESC): Hypotension, defined as a systolic blood pressure <90 mm?Hg, a drop of >40 mm?Hg for at least 15 minutes (this latter criterion may be difficult to ascertain in some clinical circumstances), or need for vasopressor support, identifies these patients. They account for ?5% of hospitalized patients with PE and have an average mortality of ?30% within 1 month.
2.Submassive (AHA) or intermediate risk (ESC): RV strain without hypotension (see above) primarily identifies these patients. RV strain includes RV dysfunction on computed tomography pulmonary angiography or echocardiography (RV/left ventricular [LV] ratio >0.9)6,7 or RV injury and pressure overload detected by an increase in cardiac biomarkers such as troponins or brain natriuretic hormone.
3.Low risk (ESC and AHA): These patients do not meet criteria for submassive (AHA) or intermediate-risk (ESC) PE"
Early administration of antibiotics for open fractures can reduce serious bone and soft tissue infections, with a common goal being antibiotic administration within one hour of injury.
In this study, there were 523 patients treated by EMS who had an open extremity fracture.
The median time from EMS dispatch until antibiotic administration was 31 minutes. 99% of the patients who received antibiotics received them within one hour of EMS dispatch. Prehospital times were on average 10 minutes longer for those patients who received antibiotics. The majority of these patients received cefazolin, followed by ceftriaxone, ampicillin, gentamicin and piperacillin/tazobactam. None of these patients required management for an allergic reaction or anaphylaxis. Five patients (1%) who received prehospital antibiotics and 159 patients who did not (1.4%) had a subsequent infection based on ICD codes.
Bottom line: In this small group, it was safe to administer antibiotics to a patient with an isolated open extremity fracture and the medication was able to be delivered earlier. Larger studies will be needed to see the impact of this practice on the development of osteomyelitis or soft tissue infections.
The CLOVERS trial (NEJM 2023) examined one of the eternal questions of critical care, liberal vs restrictive fluid management in sepsis… and found no difference. But there are criticism of CLOVERS, and while some other trials agreed with this result, there are also signals in the literature that restrictive fluid strategies are beneficial. Furthermore, we know that these trials suffer from issues of heterogeneity, and often lump together very different patients.
Jorda et al recently published in Critical Care a posthoc re-analysis of CLOVERS looking specifically at patients with advanced CKD (eGFR < 30). This is a challenging group of patients to manage. On the one hand their renal function is already marginal, so the last thing we want to do is potentially deprive starved kidneys of necessary intravascular volume, but on the flip side their septic shock puts them at high risk of full blown renal failure (transient or permanent) and they're thus at very high risk of fluid overload with aggressive resuscitative fluids and potentially limited ability to clear those fluids renally in the next few days. So how did these patients do in CLOVERS?
They did significantly better with the restrictive fluid strategy (mortality 22% vs 39%, HR CI 0.29-0.85). They also had more pressor free days and vent free days.
Bottom Line (my opinion): While a restrictive vs liberal fluid strategy in septic shock remains a bit up for debate, the evidence continues to slowly tip towards restrictive fluids (i.e. earlier pressors) as the preferred approach. In patients with advanced CKD (eGFR < 30), there is probably now sufficient evidence to favor vasopressors over IV fluid administration when resuscitating septic shock.
Many may look at the Inferior Vena Cava (IVC) to get a sense of a patient's “fluid responsiveness.” However, there are many pitfalls to using the IVC. An article by Via et al outlines these pitfalls and is an interesting read!
To summarize, IVC can be affected by:
Bottom Line: Think twice before using IVC to evaluate for fluid responsiveness.
The Bova score has been validated to predict mortality and complications in hemodynamically stable patients with intermediate to high-risk pulmonary embolisms. There is some literature on using the Bova score to decide on thrombolytics/interventional therapy as well.
Scoring Criteria:
Interpretation:
A 2020 meta-analysis attempted to estimate the frequency of radiographically occult hip fractures in the elderly population.
26 studies evaluated the rate of surgical hip fractures with no obvious findings on plain film.
Median age 80.3 years (67-82 years).
MRI used as gold standard.
The overall rate of radiographically occult hip fracture requiring surgery was 39%.
This percentage is higher than reported in other studies which may have included non-elderly patients, retrospective bias or other issues.
Overall, 18% had femoral neck fractures, 17% had intertrochanteric fractures and 1% had subtrochanteric fractures.
Elderly patients with acute hip pain and negative or equivocal findings with initial plain film imaging have a high frequency of occult hip fractures. Strongly consider advanced imaging in this population
At our institution we have developed a guideline for the use of hypertonic saline in hyponatremia.
Administration of 3% sodium chloride for acute or symptomatic hyponatremia
Acute hyponatremia with severe symptoms
Acute hyponatremia with moderate symptoms
Hyponatremia Fluid Rate Calculations (**Be Careful with Online Calculators**)
FYI: 3% Sodium Chloride (1.95 mL/mEq; 513 mEq/1 L); 0.9% Sodium Chloride (6.5 mL/mEq; 154 mEq/1 L)
Equations for Calculations
***See Visual Diagnosis for an Example with Calculations***
I don't know about you, but I'm always eager to hear new and alternative methods of pain control…
This study examined the effectiveness of transcutaneous electrical nerve stilumlation (TENS) in patients with abdominal pain. Patients were randomized to TENS or sham applied to the abdomen. The primary outcome of interest was change in pain score 30 min after the intervention, and secondary outcome was percentage of patients requiring rescue analgesia. Pain scores were measured on a verbal numeric score scale with a range from 0 to 10, with any adult patients with a minimum score of 5 being eligible.
The mean reductions in pain scores after the intervention were also similar in patients treated with TENS and sham TENS (1.9 vs. 1.7 respectively, p = 0.81). THe use of rescue analgesia was 49% in patients treated with TENS and 51% in those who received sham TENS (p=0.66). No adverse events were noted.
The authors did note that there is a challenge in blinding due to toeh absence of electrical stimulation in the sham group; nonetheless, TENS was not found to be more effective than sham. It also did not reduce the need to rescue analgesia.
Guess I'll keep looking…