There is a growing trend toward the development of specialty-specific emergency services, such as Geriatric or Oncologic EDs.
Will this trend continue? Is the segmentation of emergency care in our future? The author of this article opines that the answer depends on future outcomes research in this area.
Historically, guideline recommendations have been to use a transfusion threshold of hemoglobin < 7 g/dL for patients unless they are a) undergoing orthopedic surgery or b) have cardiovascular disease (CVD).
Applefeld et al conducted a meta-analysis in 2018 which suggested that restrictive (i.e. lower hemoglobin trigger, typically 7-8) transfusion targets lead to worse outcomes in CVD patients than liberal (i.e. higher hemoglobin trigger, typically 9-10) targets, and those authors have updated this analysis to include data from newer trials. Interestingly, the conclusion remains similar: that when you look at the larger studies on restrictive vs liberal transfusion targets, CVD plays an important role, as patients with CVD tend to do better with liberal targets, and patients without CVD tend to do better with restrictive targets. Of note, CVD is variably defined in these studies, and sometimes limited only to active Acute Coronary Syndromes, and other times refers to all patients with acute or chronic CVD. However, according to their analysis, the aggregated data suggests that we should continue having higher transfusion targets in patients with CVD, and perhaps even more in the 9-10 range, as opposed to the goals of 7 or 8 which are common.
Bottom Line: We will likely continue to see different transfusion targets recommended for patients with cardiovascular disease (CVD), and may even see guideline and blood bank recommendations raise the target for these patients more into the 9-10 range, or expand this group to include chronic CVD. This would mean a substantial increase in recommended RBC transfusions, and as emergency physicians it is important for us to monitor these recommendations, especially since transfusions are not harmless and raising hemoglobin thresholds could lead to complications that are difficult to measure in the literature.
Starting a study? Frame your research question in the PICO format:
Patients (consider severity of presentation, setting, demographics)
Intervention (either something you propose or something in use)
Comparison (another group, the same group without intervention, or a benchmark)
Outcome (a measurement)
This classic format has been used to evaluate studies, as in Journal Club (by our esteemed Dr. Wilkerson), as a literature search tool, or by the Cochrane review.
Starting with a PICO research question can help you narrow your focus and maintain it.
In this podcast, the concept of vasopressor use in hemorrhagic shock is discussed. Key take away points:
This was a cross sectional study examining insurance data to determine if there is seasonality related to ED visits and psychiatric hospitalizations related to suicidality.
Suicidality includes both suicidal ideation and suicide attempts (but not suicide). One survey showed that up to 12% of US adolescents reported serious thoughts of suicide. This study included 73,123 patients where 19.4% were direct inpatient admissions and 80.6% were ED visits, 44% of whom were subsequently admitted.
Metrics for suicidality in 10-18 year olds peaked in April and October with a nadir in June. Incidentally, in the Spring of 2020 when US schools closed due to COVID, there was a decrease in both ED visits and hospitalizations with April and May having the lowest rates across the study period.
School is believed to increase stress with risk factors such as bullying and peer pressure, academic and extracurricular stressors and poor sleep hygiene.
Bottom line: There has been an increase in adolescent suicidality over the recent years, many of whom present to the ED for evaluation. More mental health resources are needed, especially during the school year.
Maternal morbidity continues to increase in the US with a mortality rate in 2021 of 39.2 deaths/100,000 live births. There has been an intense focus on training and quality improvement within hospitals, but not much has changed in the prehospital education arena. This study aimed to quantify the complications encountered by EMS clinicians.
In the 2018-2019 EMS dataset used, there were a total of 56,735,977 EMS activations which included 8641 out of hospital deliveries, 1712 documented delivery complications and 5749 records of newborns.
1% of the out of hospital deliveries had a documented complication for the mother. Of these complications, 94% were for hemorrhage, 6% for abnormal presentation, 0.2% for shoulder dystocia, and 0.4% for nuchal cord.
Few patients had medications given, including 0.4% receiving oxytocin. no patients received prehospital blood transfusion or TXA. Of note, in the years since this data was obtained, TXA and whole blood have started to appear on more medic units, but it is still not necessarily commonplace.
Bottom line: While still rare, prehospital delivery does occur and EMS should be prepared for any possible complications. Medical directors should look at their jurisdictional/state protocols to see if oxytocin/TXA or whole blood should be included (if not already available). EMS clinicians should be educated on up to date management of OB emergencies.
This retrospective study looked at patients diagnosed with urinary tract infections receiving an IV dose of antibiotics prior to discharge and compared ED length of stay and return visit rate. They found:
“Parenteral antibiotic administration in the ED was associated with a 60-minute increase in ED LOS compared with those who received an oral antibiotic (P < 0.001) and a 30-minute increase in ED LOS compared with no antibiotic (P < 0.001). No differences were observed in revisits to the ED at 72 hours”
Appears no benefit to the practice of IV antibiotics prior to discharge in UTI patients.
Hemodynamic instability in trauma patients is most often associated with hemorrhagic shock, however, there is an entity known as brain injury associated shock (BIAS). BIAS is thought to be associated with catecholamine surges secondary to brain injury. BIAS is found in both isolated head injury pts as well as multi-trauma patients. Studies have identified BIAS in 13% of adult trauma patients and up to 40% of pediatric major trauma patients.
We know hypotension in brain injury worsens outcome. We should assume hemorrhagic etiology until we prove otherwise. Once we suspect BIAS and have excluded hemorrhagic etiology our strategy should switch to blood pressure support using non-blood product management.
Concussion Visits to the Emergency Department
In a study looking at concussion discharge instructions in the ED:
A 2020 study looked at patients aged 6-18 years diagnosed with concussion on either first or subsequent ED visit.
Those patients with delayed diagnosis required more medical visits during recovery, had a significantly longer time to symptom resolution (21 vs. 11 days), and had a higher likelihood of having persistent concussion symptoms.
Take home: Consider printed concussion discharge instructions in the appropriate ED patients as this has downstream benefits for health and recovery.
Intranasal medications are an increasingly popular option for pediatric patients, particularly for analgesia and anxiolysis, with an increasing number of medications being used via the intranasal route of administration.
Fentanyl has been shown in prior studies to be a safe and effective pain management strategy for children, but is likely under utilized. In sickle cell patients, studies have shown that time to analgesia may improve outcomes including hospitalization.
In 2023, Rees et al. showed that in the sickle cell patient population IN fentanyl can be a very effective tool for patient's experiencing a Vaso-occlusive episode (VOE). This study looked at 400 children with a mean age of 14.6 years. Of these 19% received IN fentanyl.
Ultimately, the IN fentanyl patient population had a shorter time to initial administration of analgesia and a lower chance of admission to the hospital.
Notably, this was not a randomized study, so there is limitations in assessment of the causality of the lower discharge rates. However this is a tool that could likely be used more regularly in the pediatric sickle cell patient population to allow for more rapid pain management in the emergency department.
Myasthenia gravis (MG) is an autoimmune neuromuscular disorder that affects an estimated 14 to 20 patients per 100,000 in the United States. Most patients with MG have autoantibodies against acetylcholine receptors (AChRs), which disrupt neuromuscular transmission through downregulation, destruction, blocking of AChRs or disrupting receptors in the postsynaptic membrane.
Several medications may worsen MG or precipitate myasthenic crisis, however, incidence is difficult to describe as literature is largely limited to case reports and there is often presence of other confounding factors. There are two proposed mechanisms for medications to cause or exacerbate MG:
Several medications commonly used in the emergency department are known to impair neuromuscular transmission and may induce or worsen MG. The following medications should be avoided, or used with extreme caution in patients with MG*:

*This list contains several common medications utilized in the emergency department, but is not an all-inclusive list of medications that may exacerbate MG. Please refer to the reference section for additional information.
Oftentimes, CT imaging is used in diagnosis of emergent abdominal pathology. However, there may be instances where there is hesitancy to use IV contrast, whether due to patient factors or extrinsic factors (remember the contrast shortage during covid?)
This study examines the diagnostic accuracy of dry CT. 3 quaternary centers with residency training programs participated, and contrasted images underwent further processing to remove any IV or oral contrast. Both residents and faculty reviewed the images, and findings were compared to both the initial read by radiologist as well as independent reads by a panel of experts. They looked for both primary findings (those that explained the abdominal pain) as well as actionable secondary findings (ie incidental findings requiring additional imaging or further management).
When compared to contasted imaging, the accuracy of dry CT was 70% (faculty, 68% to 74%; residents, 69% to 70%). Faculty had higher accuracy than residents for primary diagnoses but lower accuracy for actionable secondary diagnoses.
Thus when considering the necessity of contrast, please consider the potential for missed diagnosis.
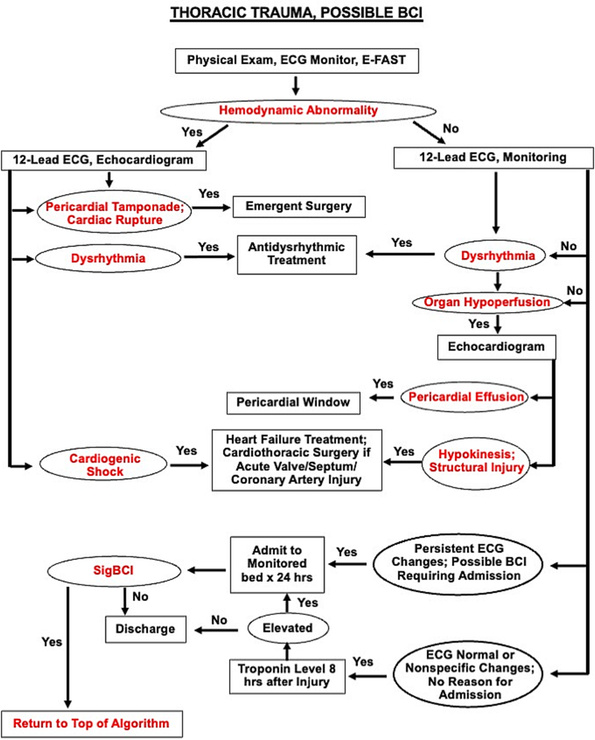
Blunt Cardiac Injury is a continuum from asymptomatic, not clinically relevant to catastrophic, life ending disease . Consider blunt cardiac injury in patients with significant force to the chest wall or sudden deceleration injuries (motor vehicle crashes, motorcycle crashes, falls from height etc.). This algorithm is helpful when working up patients suspected of having significant blunt cardiac injury.
BACKGROUND:
Prehospital administration of whole blood involves some areas of controversy. Though theoretical benefits are clear, concerns about logistics and timing of blood often dominates the discussion. This study was a retrospective analysis of prehospital blood administration within an urban EMS system from 2021-2023. Primary endpoints included: time to administration and in hospital mortality.
PATIENTS/METHODS:
The study population included patients presenting to the EMS system with signs and symptoms of hemorrhagic shock (SBP<70 or SBP<90 + HR> 100, n=61) and who received at least 1 unit of prehospital blood (PHB). The EMS system administered blood in conjunction with an advanced resuscitative bundle (calcium, TXA, blood). Isolated head injuries and blunt trauma patients were excluded from the analysis. The control group (n=82) was comprised of patients in the system's trauma registry presenting to EMS PRIOR to the initiation of whole blood and who exhibited similar clinical crtieria.
RESULTS:
BOTTOM LINE:
In this prospective study conducted within an urban EMS system, patients receiving prehospital whole blood demonstrated improved vital signs and reduced mortality when compared to a control group. Slightly extended prehospital time intervals for patients receiving PHB may be offset by the measured benefits of whole blood therapy.
Perinatal mental health problems are unfortunately quite common: according to the World Health Organization, approximately 10% of women in high-income countries and approximately 30% in low- or middle-income countries are affected.
It's important to be able to distinguish “baby blues” from more significant mental health issues. Typical symptoms of the “baby blues” include mild and short-lived changes in mood, as well as feelings of exhaustion, worry, and unhappiness in the weeks that follow giving birth.
Symptoms that are more severe or lasting >2 weeks post-partum should prompt further investigation and discussion with a mental health professional. Symptoms of perinatal depression may include: feeling persistently sad, feelings of hopelessness, loss of interest or pleasure in hobbies/activities, trouble bonding with the infant, appetite changes, and can even become as severe as wanting to harm onself or one's child. There are specific DSM-5 Criteria used to diagnose postpartum depression.
Universal screening for all pregnant and postpartum patients is highly recommended, and can be life-saving.
Title: Safety and Efficacy of Reduced-Dose Versus Full-Dose Alteplase for Acute Pulmonary Embolism: A Multicenter Observational Comparative Effectiveness Study
Settings: Retrospective observational study from a combination of Abbott Northwestern Hospital and 15 others as part of the Mayo Health system.
Participants: Patients between 2012 – 2020 who were treated for PE. Patients were propensity-matched according to the probability of a patient receiving a reduced- dose of alteplase.
Outcome measurement:
Study Results:
Discussion:
Conclusion:
In this retrospective, Propensity-score matching study, the full-dose regimen but is associated with a lower risk of bleeding.
How do you look for signs of a pleural effusion with ultrasound?
Place your ultrasound probe in the mid axillary line with the probe marker placed towards the patient's head.
Find the movement of the diaphragm and scan just above the diaphragm.
In normal lung, air scatters the ultrasound signal, and you are not able to see structures above the diaphragm.
With a pleural effusion, you can see:
In a cohort of 93,512 ED patients discharged with a diagnosis of hypertension there were 4400 who received a prescription for antihypertensives. The group receiving a prescription had fewer 30 day revisits and adverse events such as MI, CHF, etc.
Previous study’s have found it is safe to prescribe antihypertensives from the ED.
This study is limited by the fact it is not a randomized control trial and there are many variables as to why the select patients received prescriptions
The authors conclude: “Prescription antihypertensive therapy for discharged ED patients is associated with a 30-day decrease in severe adverse events and ED revisit rate.”
New progress in head injury prevention in football
A Guardian Cap is a soft padded soft shell worn over football helmets.
Think of it like a shock absorber
It is intended to mitigate energy transfer to the head and neck during player impacts.
It retails for about $70 on amazon!
https://www.pinkvilla.com/pics/855x855/236466742_untitled-design-2024-04-27t133219-626_202404.jpg
Most NFL players have worn these caps during preseason practices for the past 2 years.
The NFL found a 52% reduction in preseason concussions (at the same position) between players who wore the cap versus those who did not.
In laboratory testing the Guardian cap reduced head impact forces by up to 1/3rd in certain impacts.
Per NFL analytics, the Guardian cap absorbs 10% of the traumatic force.
Additionally, if two players suffer a helmet to helmet hit in which each wears the cap, the impact force is reduced by 20%!
The NFL has allowed players to wear the caps this year
They will have the team logos on them
2024 season: Players will wear the caps or one of 6 approved helmets (position specific) that provide equal or better protection.
If your child plays football, consider investing in this product as a potential means to reduce head impact forces and concussion.
More data is needed during regular season games with full speed collisions.
A small study retrospectively looking at recorded calls to a level 1 trauma center transfer line specifically looking at patients who died or were discharged to hospice without surgical intervention found only 10% had goals of care discussed prior to transfer. Most were brain hemorrhage patients.
As a transferring facility, clearly outlining goals of care and addressing futility of care can have a major impact on trauma transfers and the cost and family burden associated with transfers.
{kind=link}