When it comes to walking, recent research and public health strategies have focused on how much you do that helps. This idea frequently comes up in the form of the 10,000 step goal.
A recent study in the British Journal of Sports Medicine found that walking between 9,000 and 10,000 steps/day could reduce the risk of death by 39% and cardiovascular disease by 21%.
For both outcomes (all-cause mortality and incident CVD), approximately 50% of the benefit was achieved between 4,000-4,500 steps per day.
Study accessed data on greater than 72,000 individuals (avg age 61, 58% female) using accelerometer data over an average of 6.9 years.
Instead of volume, a recent study in the same journal looked at the benefits of walking speed.
The study looked at pooled data from 10 studies involving more than 500,000 people from the U.S., Japan and the U.K.
Walking speed definitions:
Easy or casual walking - less than 2 mph.
Average or normal pace was defined as 2-3mph.
A “fairly brisk” pace was 3-4 mph
A “brisk/striding walking pace” was greater than 4mph
Compared with people who walked at a casual/easy speed, those who walked at a normal/avg speed (2–3 mph) had a 15% lower risk of Type 2 diabetes.
Walking at a fairly brisk pace (3–4 mph) was associated with a 24% lower risk of Type 2 diabetes.
Walking at a brisk or striding pace (over 4 mph) was associated with a 39% reduced risk of Type 2 diabetes.
Globally, 537 million adults have type 2 diabetes, a figure that is expected to reach 783 million by 2045.
Take home: Consider recommending tips on walking pace and distance for our sedentary patient population to optimize health.
“I’m not going to the hospital, my father died in a hospital.”
In planning a study it’s a good practice to consider what confounding variables you may need to look out for.
Confounding variables are associated with the predictor (independent) and outcome (dependent) variables, but they are not in the causal chain. In the above example, disease is likely the predictor variable, death is the outcome variable, and going to the hospital is a confounder. Of course, this assumes the death was not iatrogenic; then the hospital would be in the causal chain.
Patients may be selected for interventions based on severity of disease, functional status, education level, and other factors, and these may be confounders.
Confounding can be addressed at the design stage, by:
It can be addressed in the analysis stage by:
Euglycemic DKA (eDKA) is a medical emergency requiring prompt attention. It is caused by an imbalance of insulin and glucagon leading to ketone accumulation (1-3). In addition to typical risk factors for DKA, those for eDKA include SGLT-2 inhibitor use and pregnancy, with 30% of DKA cases in pregnancy presenting euglycemic (4, 5).
eDKA presents with an anion gap metabolic acidosis, ketosis/ketonuria, & blood glucose less than 250 mg/dL.
Diagnosis requires ruling out other causes of anion gap metabolic acidosis, including toxic ingestions.
The cornerstone of eDKA management is ensuring enough dextrose to allow needed insulin administration to reverse ketone accumulation.
To obtain a posterior shoulder view: Have the patient sit up with the back of the bed down. Position the curvilinear probe in the posterior aspect of the shoulder with the probe parallel to the patient bed, at the level just below the scapular spine and the marker towards the patient's left. You can have the patient rotate their arm to help you visualize the movement of the humeral head.
In the normal anatomy, the humeral head should be at the level of the glenoid (this is a patient's left shoulder):
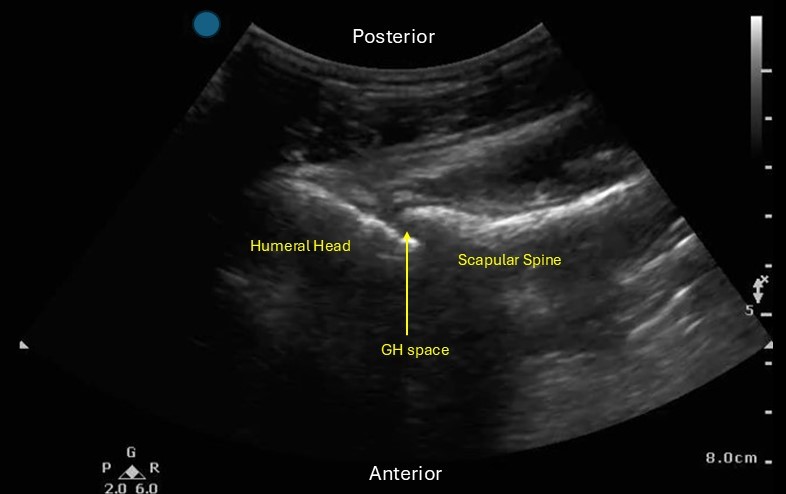
Locate the glenohumeral joint space. You can evaluate the GH joint for effusion, perform joint arthrocentesis/injection and look for signs of shoulder dislocation.
If you are evaluating for signs of a dislocation:
Posterior dislocation: the humeral head will be more SUPERFICIAL in the image than the scapular spine
Anterior dislocation: the humeral head will be DEEPER in the image than the scapular spine.
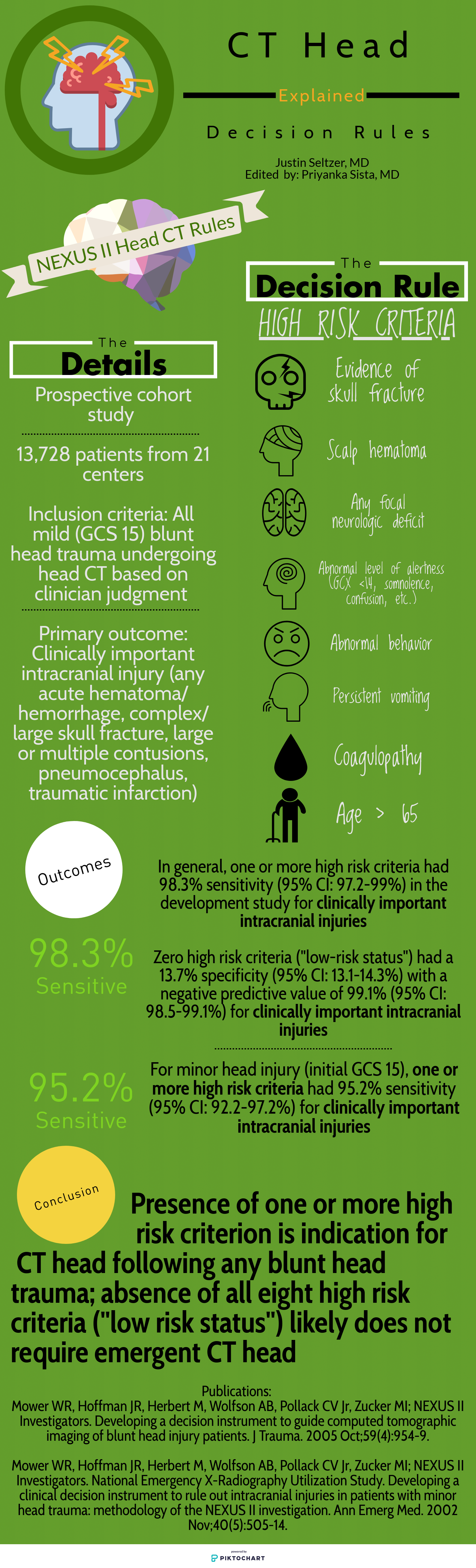
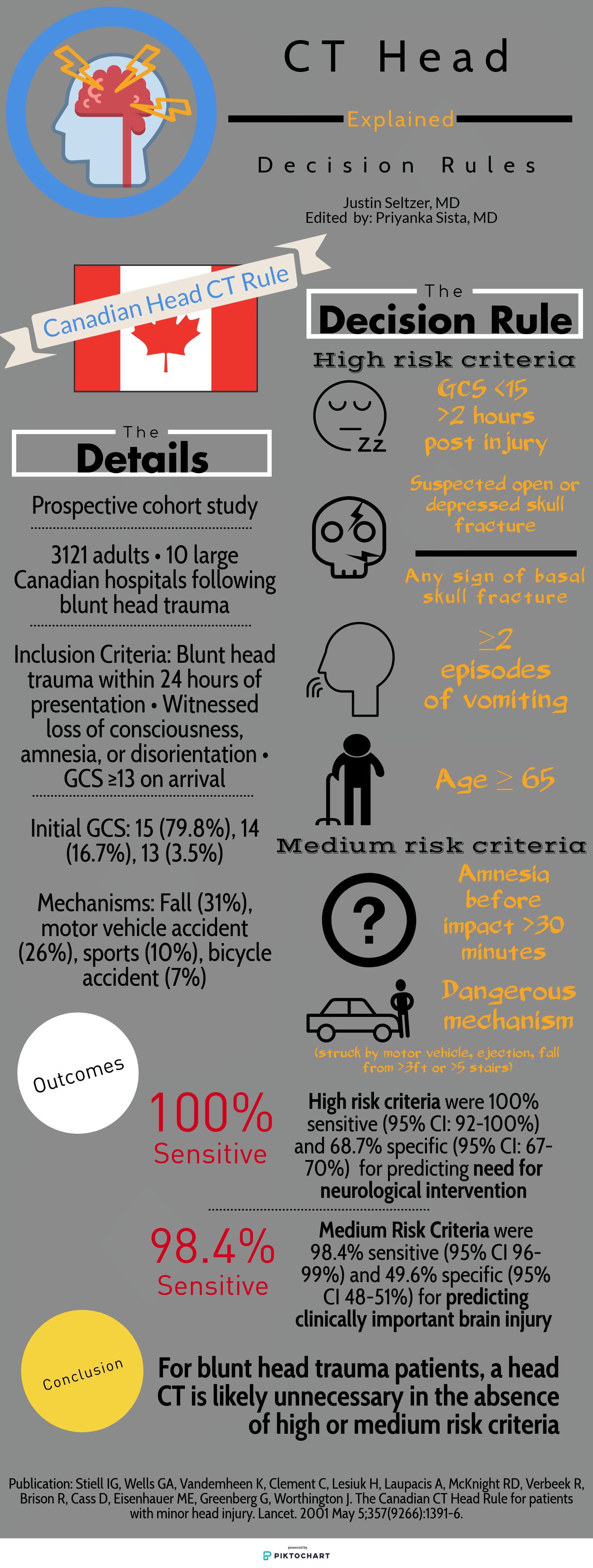
Deciding who needs exposure to radiation after blunt head injury has been looked at by both the Canadian Head Injury Guidelines as well as NEXUS. This website has excellent graphics outlining the rules. Note age over 65 alone is predictive of significant intracranial injury. All recent studies indicate age over 65 even with a low suspicion mechanism such as fall from standing is still a significant risk for intracranial pathology.
This retrospective study found that while overall rates of antibiotic prescriptions for viral URIs were low (that's good!), patients identified as non Hispanic white were prescribed antibiotics, despite guidelines advising against them, at a higher rate than non white patients (that's bad). It also found that in areas of socioeconomic deprivation, the prescribing rates were lower across all races than in more affluent areas (that's good and bad!)
This was an observational study where ultrasound was used to evaluate if the diaphragm came into view at the 5th intercoastal space (ICS) at the midaxillary line in pediatric patients during maximal respiration. A convenience sample of pediatric patients who presented to the an academic pediatric emergency department was used.
In 10.3% of patients, the diaphragm crossed the 5th ICS during normal respirations and 27.2% crossed during maximal respirations. This was a more common occurrence on the right compared to the left. An increase in body mass index was also associated with an increased risk of the diaphragm crossing the during both tidal respiration and maximal respirations.
Bottom line: Using a blind insertion of a chest tube at the 5th ICS, midaxillary line in the pediatric patient poses a not insignificant risk of piercing the diaphragm. this study recommends using ultrasound prior to chest tube placement.
A study looking at patients over age 65 with head injuries from falls assessed the association of alcohol use with severity of injury. The alcohol use was self-reported which does limit the findings. The study found “Of 3128 study participants, 18.2% (n = 567) reported alcohol use: 10.3% with occasional use, 1.9% with weekly use, and 6.0% with daily use.” Those daily drinkers had a higher incidence of intercranial injuries.
The authors concluded: “Alcohol use in older adult emergency department patients with head trauma is relatively common. Self-reported alcohol use appears to be associated with a higher risk of ICH in a dose-dependent fashion. Fall prevention strategies may need to consider alcohol mitigation as a modifiable risk factor.”
This study, done out of Australia, examined the association between abdominal pain and severity of liver injury in patients presenting after acute acetaminophen overdose.
539 cases were identified where N-acetylcysteine was administered to patients with acetaminophen overdose. The investigators explored parameters including presence of abdominal pain, time post-ingestion, and peak ALT.
Patients less than 8 hours post overdose WITH abdominal pain were as likely to develop hepatotoxicity as those presenting WITHOUT abdominal pain. (OR=1.18 [0.07 to 19.4])
Patients presenting 8 or more hours post overdose WITH abdominal pain were as likely to develop hepatotoxicity as those WITHOUT abdominal pain (OR=1.28 [0.39 to 4.21])
Don't let lack of pain fool you! Just as we all learned in medical school - let your history be your guide!
Diabetic ketoacidosis (DKA) is a serious condition that carries the risk of significant morbidity and mortality if not managed appropriately. Typically managed with an infusion of regular insulin, IV fluids, and electrolytes, there is evidence to support treatment of mild to moderate DKA with a subcutaneous (SQ) regimen using a combo of fast-acting and long-acting insulin instead, decreasing the need for ICU admission without increasing adverse events [1].
What patients?
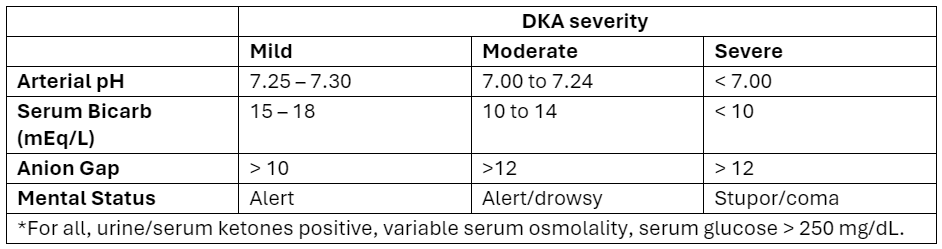
Adapted from Abbas et al.
How to manage?
Initial dose
Subsequent dosing:
If serum glucose is > 250 mg/dL
If serum glucose is < 250 mg/dL
Bottom Line
DKA management with a SQ insulin protocol is a reasonable approach for patients with mild to moderate DKA, is supported by the American Diabetes Association [5], and can be particularly helpful in this era of ED boarding and bed shortages. Give a long-acting insulin dose every 24 hours (or restart the patient’s home long-acting regimen) and short-acting insulin every 2 to 4 hours. Aggressive IV fluid resuscitation, electrolyte repletion, and treatment of underlying precipitating cause remain additional cornerstones of DKA management.
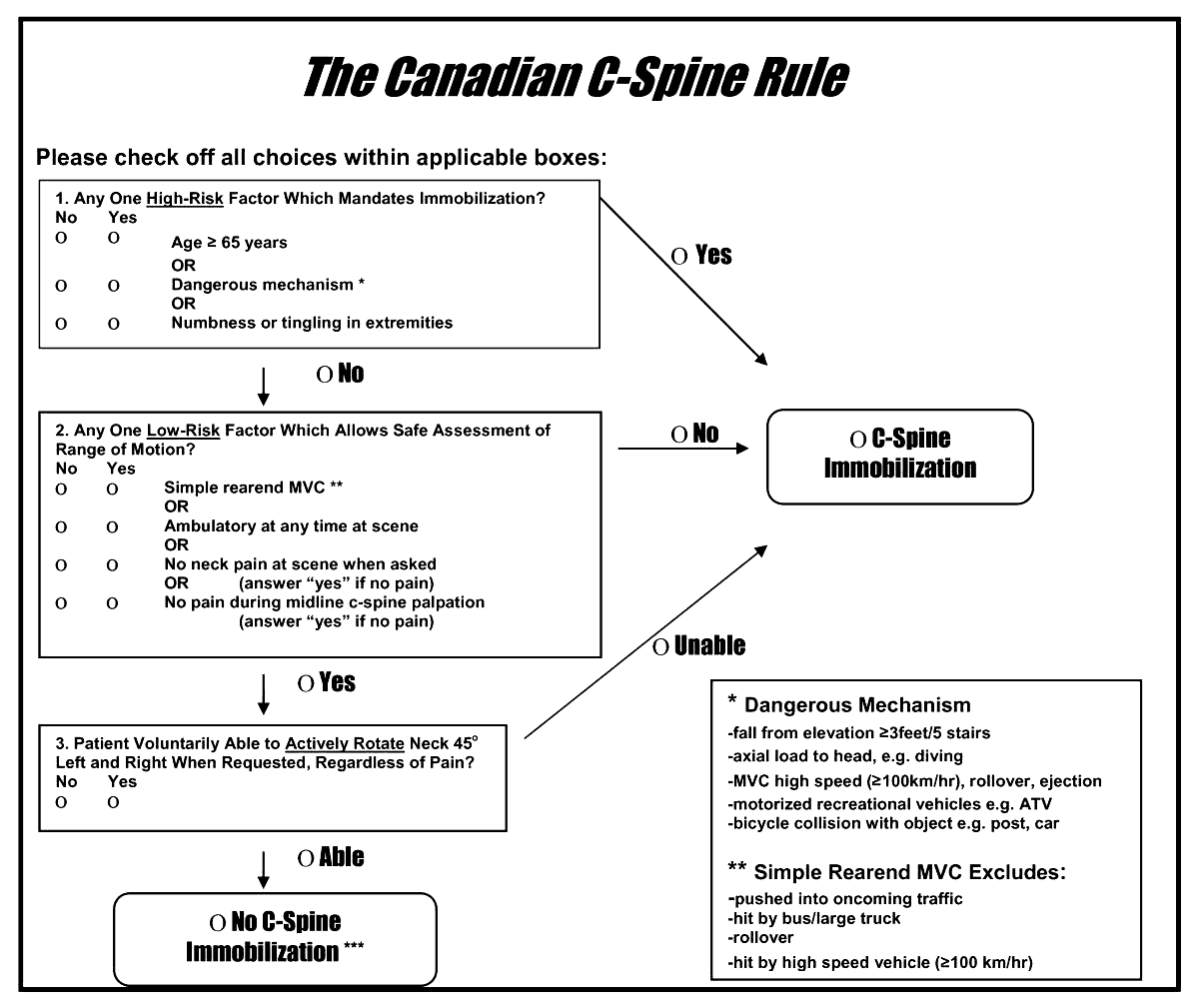
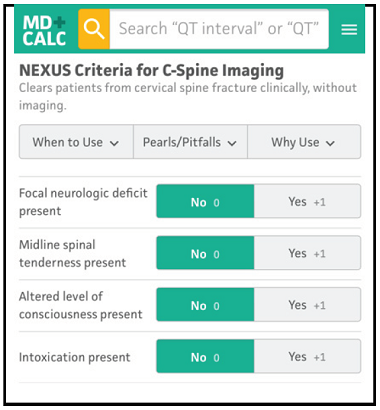
A reminder of two validated tools used to determine the need for cervical spine imaging in adult blunt trauma patients. A recent meta analysis concluded:
“Based on studies, both CCR and NEXUS were sensitive rules that have the potential to reduce unnecessary imaging in cervical spine trauma patients. However, the low specificity and false-positive results of both of these tools indicate that many people will continue to undergo unnecessary imaging after screening of cervical SCI using these tools. In this meta-analysis, CCR appeared to have better screening accuracy.”
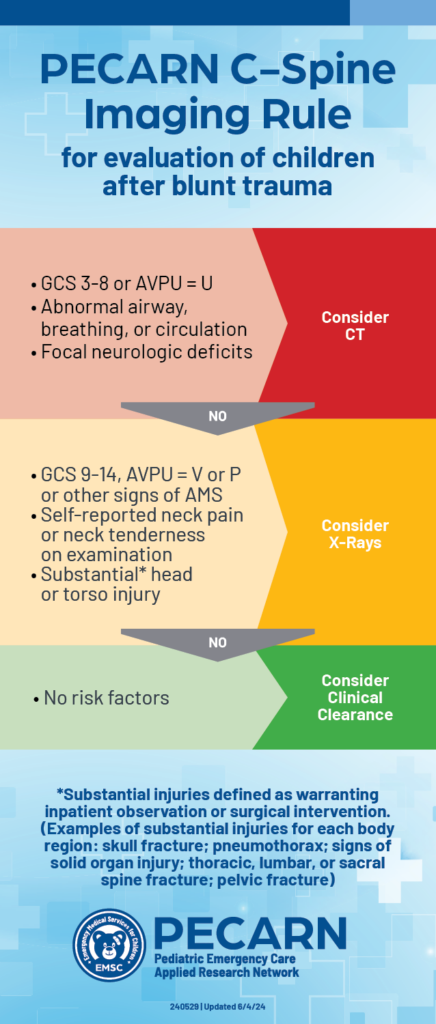
A just released study published in the Lancet gives us guidance on which pediatric blunt trauma patients need cervical spine imaging. Age range was 0-17 years.
“Out of 22,430 children included in the study, 433 (1.9%) were found to have Cervical spine injury (CSI). The study identified 4 high risk factors for CSI to be used to triage children to CT (12% risk for a cervical spine injury):
In children without high-risk findings, 5 additional findings identified children with intermediate, non-negligible risk of CSI (3.6% risk of a cervical spine injury):
The Lever test can be used to examine for a torn ACL
May be helpful when examining larger patients
Place patient supine with both knees extended. Examiner places fist below the proximal third of patient’s calf.
With the other hand, the examiner presses down on the distal third of the patient’s quadriceps.
Positive test: A torn ACL disrupts the lever arm of the lower leg. The heel will not rise.
Negative test: An intact ACL allows the lever arm of the lower leg to lift the heel. The heel will rise.
More study is needed but reported sensitivities are similar to classic tests such as the anterior drawer or Lachman.
Breastfeeding provides a great nutrition source for infants, but early cessation is common for a wide variety of reasons. Notably, being asked to withhold breastmilk (“pump and dump”) due to safety concerns or illness increases rates of termination.
A recent paper is an invaluable reference on commonly used medications in the care of emergency department women of childbearing age and the lactation risk. It breaks down medications into clinical categories and then further highlights those that are safe, likely safe, and safe-but may reduce milk supply, and those to avoid.
The majority of commonly used medications in the ED are safe to use in breastfeeding. Only 3% of the medication analyzed should be avoided (aspirin [at doses > 325mg/day], dicyclomine, prochlorperazine, and benzonatate) and in most cases a safe alternative could be used.
Using these recommendations can help prescribe safe medications, prevent the recommendations to pump and dump, and relieve stress for the patient breastfeeding.
Consider adding the LactMed(R) app to your phone as well - This is a free database through the NIH to search individual medications to assess risk in lactation.
BACKGROUND:
Cardiac arrest is time sensitive disease. Despite significant advances in resuscitation technology such as eCPR and mechanical compression devices, early basic life support interventions (specifically bystander CPR) are strongly associated with survival. EMS systems must advocate for early initiation of bystander CPR. Dispatch Assisted CPR (DA-CPR) is one of several strategies designed to improve outcomes and encourage early compressions. To optimize survival, EMS systems should achieve a comprehensive understanding about barriers to succesful initiation of DA-CPR.
METHODS AND OUTCOMES:
49,165 patients with out of hospital cardiac arrest were eligible for inclusion the study, and over 36,000 underwent successful DA-CPR. The study's primary outcome was good neurological recovery at hospital discharge. Secondary outcomes included: prehospital return of spontaneous circulation (ROSC)and survival to hospital discharge. The authors defined successful DA-CPR when bystanders initiated compressions and continued resuscitation until the arrival of EMS.
RESULTS:
Quite a few results were consistent with prior studies. Unsuccessful DA-CPR was associated with:
Successful DA-CPR was more likely associated with the presence of family members at the scene and improved neurological recovery. Witnessed arrests were also more likely to receive successful DA-CPR. Not surpringly, patients in the successful DA-CPR group also exhibited improved survival to discharge and prehospital ROSC.
BOTTOM LINE:
Though the study is retrospective and involves a host of confounding variables, EMS systems continue to identify modifiable factors linked to the delivery of DA-CPR. Improved community CPR education and dispatcher training may contribute to higher DA-CPR rates.
BALTIMORE, MD, SPECIFIC PEARL:
Baltimore metropolitan jurisdictions are collaborating with the CPR LifeLinks program to address DA-CPR. The CPR LifeLinks program a national initiative “to help communities save more lives through implementation of telecommunicator and high performance CPR programs." https://www.911.gov/projects/cpr-lifelinks/
We heard it before. Continuous administration of antibiotics might be associated with better outcomes. However, results from smaller randomized controlled trials of beta-lactam showed inconsistent conclusions. Therefore, a large RCT was conducted
Settings: 31 ICUs in Croatia, Italy, Kazakhstan, Russia between June 2018 – August 2022.
Randomized, double-blind control trial.
Participants:
Outcome measurement:
Study Results:
Discussion:
Conclusion:
In critically ill patients with sepsis, continuous administration of meropenem did not improve mortality nor reduce the emergence of pandrug resistant bacteria.
In a critically ill trauma patient, the FAST exam is used to evaluate for potential internal injuries. Specifically, the subxiphoid view of the FAST exam helps assess for signs of pericardial tamponade. However, distinguishing between a pericardial effusion and an epicardial fat pad can be challenging.
One study indicated that the sensitivity of EPs in differentiating between effusion and fat pad was 73%, with a specificity of 44% when reviewing difficult patient video clips.
Here are some tips to help you distinguish between effusion and fat pad:
Change your view: Use the parasternal long axis view, which is more sensitive for effusion. Fat pads are usually anteriorly, and effusions tend to accumulate posteriorly in a supine patient.
Screen for other signs of tamponade: Adjust your subxiphoid view to visualize the IVC entering the right atrium, allowing better visualization of the right side of the heart.
Movement: Fat tends to move synchronously with the heart, whereas hemopericardium moves independently.
Echogenicity: Fat typically appears brighter on ultrasound, while blood tends to be less echogenic.
For further learning, refer to the supplemental Material from the referenced articles.
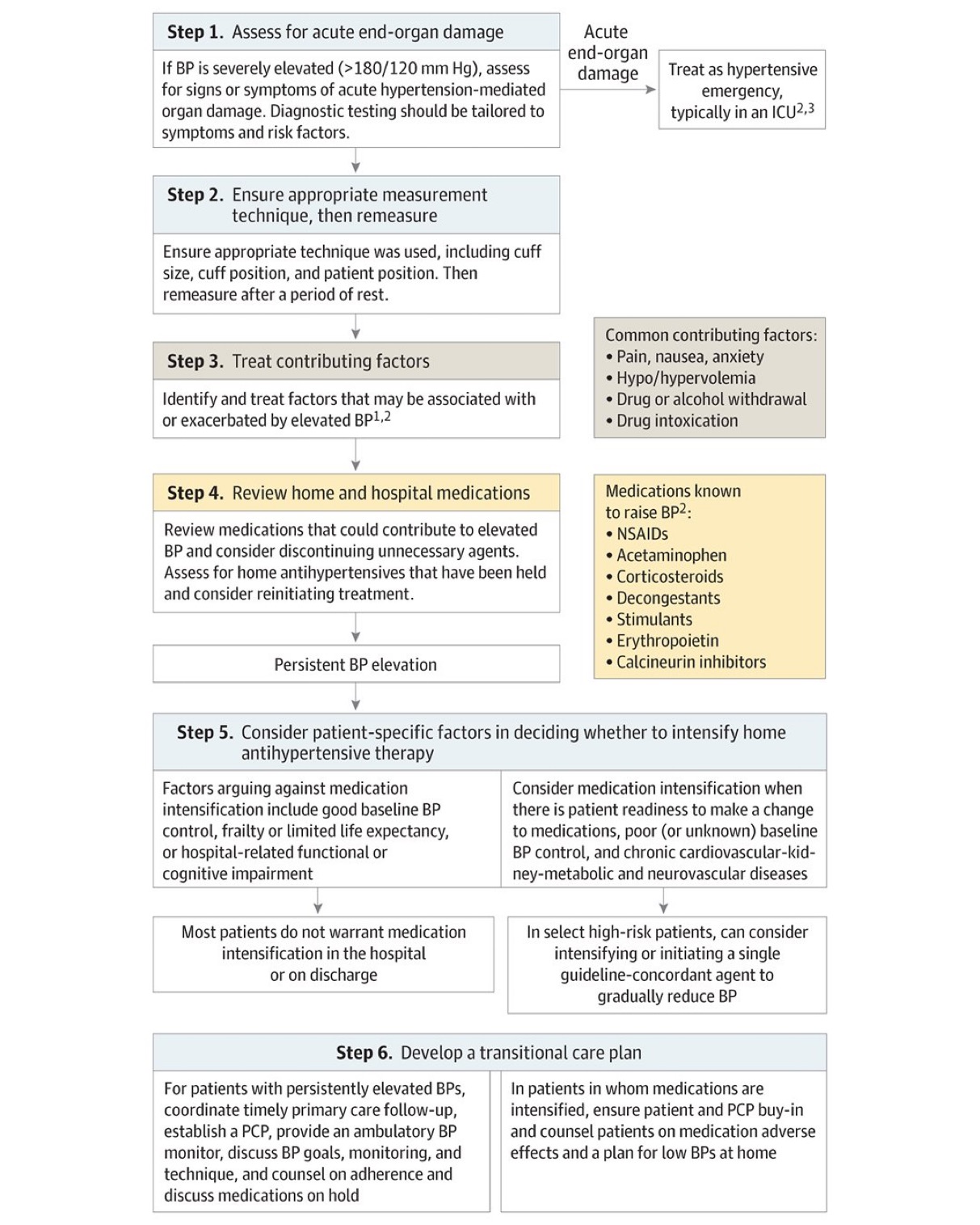
This article from JAMA is targeted at inpatient management of asymptomatic hypertension, however, it’s a great reminder that “hypertensive urgency” is not an entity. We should be treating the patient and not the numbers. Gradual, out patient lowering of asymptomatic hypertension is the safe and proper way to approach this. Spread the word to your friends in primary care, urgent care, dental, and other office based practices.
This article serves as a great reminder that our older patients are on a significant amount of medications and many of these medications effect cognition. Cognitively impaired patients are at risk of medication errors. High risk medications in older patients include anticoagulants, opioids, anticholinergics, hypoglycemic/insulin and sedating medications. The authors found:
It is important to ask how the patient takes (or doesn’t take) their medications as well as other social determinate of health such as living alone.
Hyperkalemia is less common than hypokalemia in pediatric patients, though it is not uncommon to have hemolysis in patients who receive heel stick lab work.
The age of the patient is critical to determining the cutoff for hyperkalemia:
Typically, levels up 6.0mmol/L are well tolerated in children, unless the shift is rapid. For any child meeting age related hyperkalemia or who have a known lower prior potassium level should receive an ECG.
Treatment for hyperkalemia is similar to adults
Calcium Chloride (20mmg/kg - Max 1g) or Calcium Gluconate (0.5ml/kg - Max 20ml) is given for cardiac stability.
Albuterol can be given based on weight
Insulin and dextrose can be used with extreme caution and close monitoring for hypoglycemia. (Dextrose should be given as D10% in children under 5 years of age, D25% can be used if > 5 years old)