There are some studies that have shown that NSTEMI patients have done worse when administered opioids. Most studies were not well controled and the exact mechanism was not clear. This study adds a biological mechanism to these fidnings.
Hobl et al. showed clopidogre concentrations delayt peak yhours, have overall decrease AUC and actually decrease active metabolites when morphine is administered IV. Morphine may not be the right choice in any ACS that receives clopidogrel.
A Lancet Commission on Global Surgery has just published a 56 page article about the need to improve access to surgery and anesthesia care. Its five key messages are:
The need for high quality acute care, both for urgencies and emergencies, is clearly an important component of providing “universal access to safe, affordable surgical and anaesthesia care”- the vision of the Commission.
SIRS and Severe Sepsis Screening
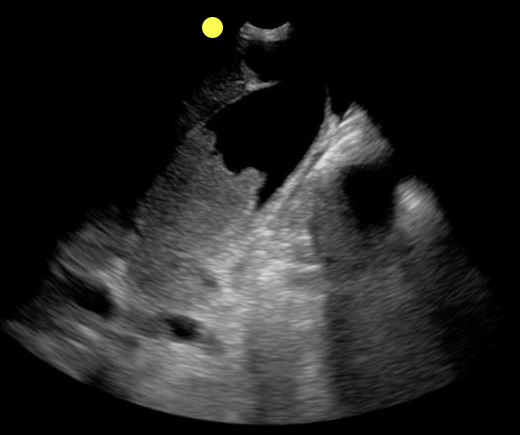
70 year-old female presents from a nursing home with fever and abdominal pain. A right upper quadrant ultrasound is shown, what's the diagnosis?
In cases of suspected spinal infection, the sensitivity of an elevated WBC count (35-61%), ESR (76-95%) and CRP (82-98%) may help guide further evaluation or consideration of other entities.
Incorporation of ESR/CRP into an ED decision guideline may help differentiate those patients in whom MRI may be performed on a nonemergent basis.
An elevated ESR (>20 mm/hour) also has a role in the diagnostic evaluation of occult malignancy (sensitivity 78%, specificity 67%).
Some medical issues arise in patients with brain tumors:
// Steroids are used to decrease vasogenic edema, especially preop or during radiation therapy. Patients are ideally gradually weaned off steroids. Dexamethasone is most commonly used. 1-2% of patients are at risk for adrenal suppression.
// Infections: Post-op wound infections can be delayed up to months, especially in patients on steroids.
// Antiepileptics: Although technically not recommended in patients with brain tumors who have not had seizures (American Academy of Neurology 2010), many surgeons continue to prescribe antiepileptics preoperatively and then discontinue them by 1 month postop if the patients remain seizure-free. Levetiracetam is emerging as the drug of choice due to favorable side effect profile.
// Thromboembolism: Brain tumors are considered very high risk for venous thromboembolism. Low-molecular-weight heparin is the treatment of choice, with warfarin being an acceptable substitute.
// Arterial thrombosis and ischemic stroke: Risk is increased with certain medications, and thrombolysis is contraindicated.
Updates in the Management of Large Hemispheric Infarction
Large hemispheric infarctions (LHI) are estimated to occur in 2-8% of all hospitalized ischemic strokes and 10 15% of all MCA territory infarcts. LHI carry high rates of morbidity and mortality, in fact, if left untreated associated cerebral edema can rapidly progress to transtentorial herniation and death in 40 80% of patients.
Recognized risk factors for progressive cerebral edema include:
Evidence based medical strategies for LHI include:
Prophylactic hemicraniectomy
Bottom Line: Early recognition of large hemispheric stroke is critical as it is associated with a high rate of morbidity and mortality. Aggressive medical management and early neurosurgical involvement may improve outcomes.
References
Follow me on Twitter @JohnGreenwoodMD
You see the following on a parasternal long-axis view; what's the diagnosis and what coronary distribution is involved?
Cardiac Sarcoidosis
- Cardiac Sarcoidosis (CS) is reported to involve ~2-5% of patients with systemic sarcoidosis. An increasing proportion of patients are presenting with isolated CS.
- Isolated CS is associated with a higher female predominance; severe LV involvement, heart failure, and poor prognosis.
- Manifestations range from symptomatic conduction disturbances, dysrhythmias, progressive heart failure, and silent myocardial granulomas - leading to sudden cardiac death.
- CS is a serious condition with a quoted 5-year survival ~60-75%.
- Corticosteroid therapy is considered cornerstone in management, but evidence is largely observational and no randomized trials have been performed to date.
Is acetaminophen good for pain control in patients with Osteoarthritic of the Knee or Hip or Low Back Pain? Most of my patients request narcotics, but conventional teaching is that we should try to start with Acetaminophen or NSAIDs.
This recent study, http://www.bmj.com/content/350/bmj.h1225, published in the BMJ analyzed 13 studies looking at over 5400 patients. In the end, they found that acetaminophen did not appear to improve pain, disability or the patient’s quality of life in patients with back pain. Also, there was a small improvement in pain and disability in those with hip and knee pain, but it was not deemed clinically significant.
Even worse, patients taking acetaminophen had a 4x greater chance of having abnormal liver function tests.
This meta-analysis really questions whether Acetaminophen should be first line therapy in patients with osteoarthritis of the knees or hips, or in those with low back pain. For now I will stick with a course of a NSAID. Especially with the risk of unintentional overdose if they are taking other over the counter medicaitons that might also contain acetaminophen.
Approximately ¼ of lumbar punctures (LP) are traumatic or unsuccessful in infants. What is the implication of this?
A retrospective cross sectional study over a 10 year period at Boston Children’s Hospital looked at infants aged 28 to 60 days who had blood cultures sent from the Emergency Department and who had LPs performed. The ED clinicians at this facility routinely follow the “Boston Criteria” to identify infants at low risk for spontaneous bacterial infection (SBI). Traumatic LPs were defined as CSF red cell count greater than or equal to 10x10^9 cells/L while an unsuccessful LP was defined as one where no CSF was available for cell counts. A small portion of the unsuccessful LPs did not have CSF cultures sent.
173 infants had traumatic or unsuccessful LPs. The SBI rate did not differ between the normal LP and the traumatic and unsuccessful LP infants. Median hospital charges were higher in the traumatic or unsuccessful LPs compared to the normal LP group ($ 5117 US dollars versus $ 2083 US dollars).
Bottom Line: Traumatic or unsuccessful LPs lead to higher hospital charges.
In 2011, approximately 630,00 children under 15 died from unintentional injuries. Injuries are the leading cause of childhood deaths in children over 9 years old. Ninety-five percent of these childhood injuries occur in lower- and middle-income countries.
The 2008 World Report on Child Injury Prevention listed the following as the top five causes of pediatric injury deaths globally:
1) Road Crashes- approximately 260,000/year
2) Drowning- approximately 175,0000/year
3) Burns- approximately 96,000/year
4) Falls- approximately 47,000/year
5) Poisoning (unintentional)- approximately 45,000/year
Many of these deaths occur around the home and could be prevented through proven prevention measures, which include:
· Child appropriate seatbelts and helmets
· Separate children from vehicular traffic
· Limit hot tap water temperature
· Placing medications and potentially harmful household products in child proof containers
· Draining unnecessary water from baths and buckets
· Redesigning nursery furniture, toys and playground equipment
· Strengthening emergency medical services
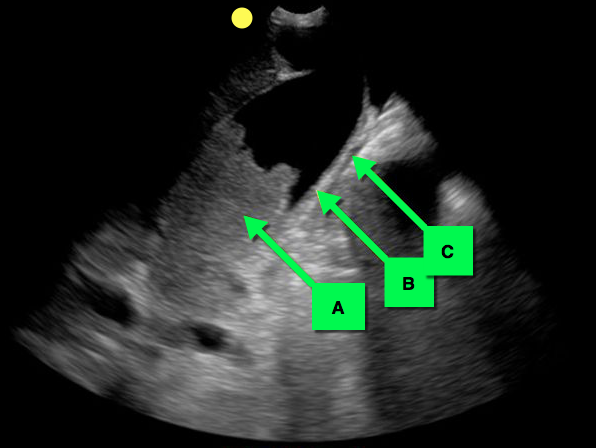
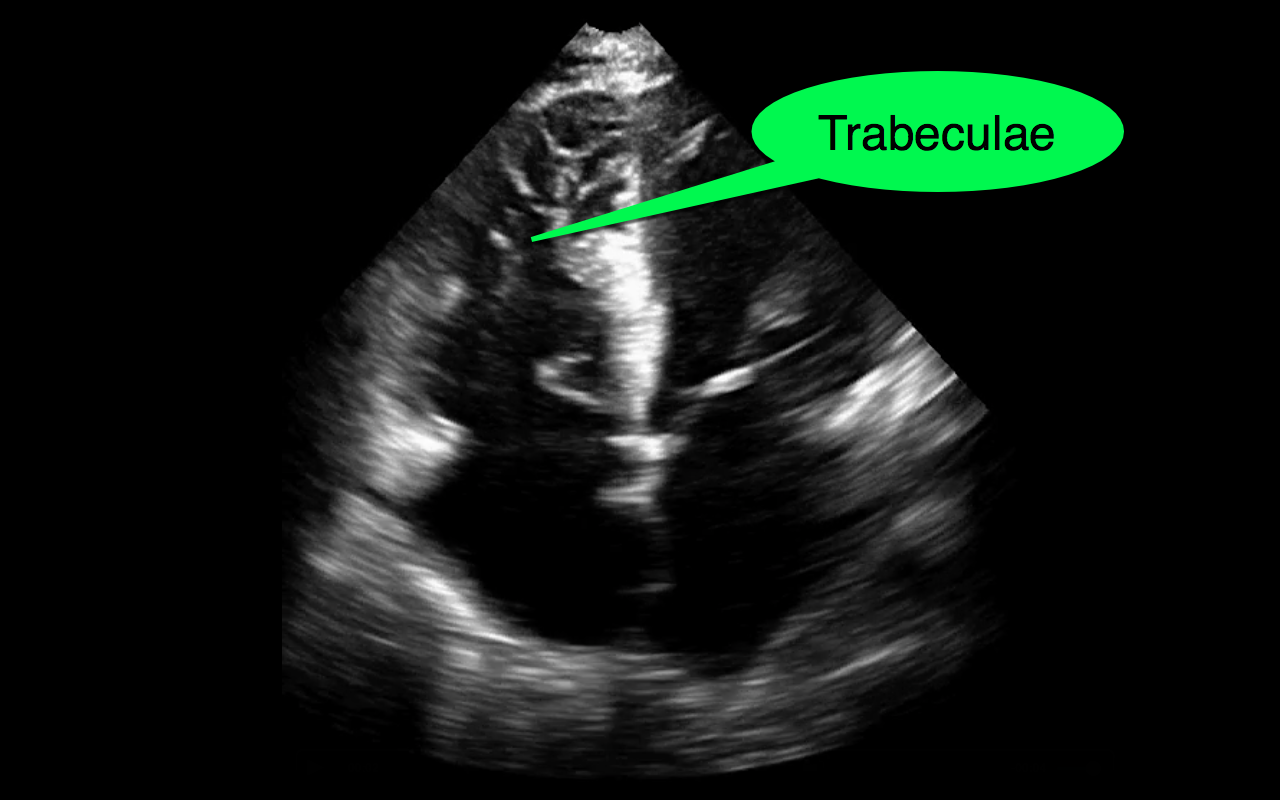
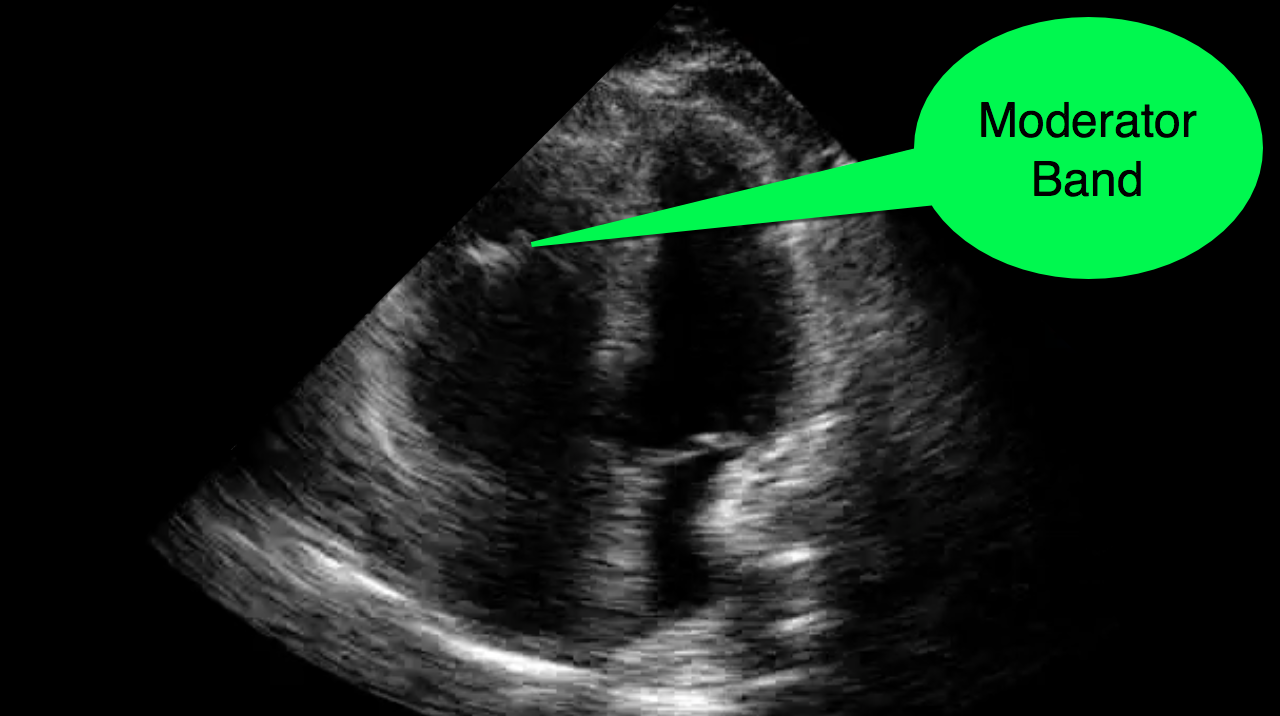
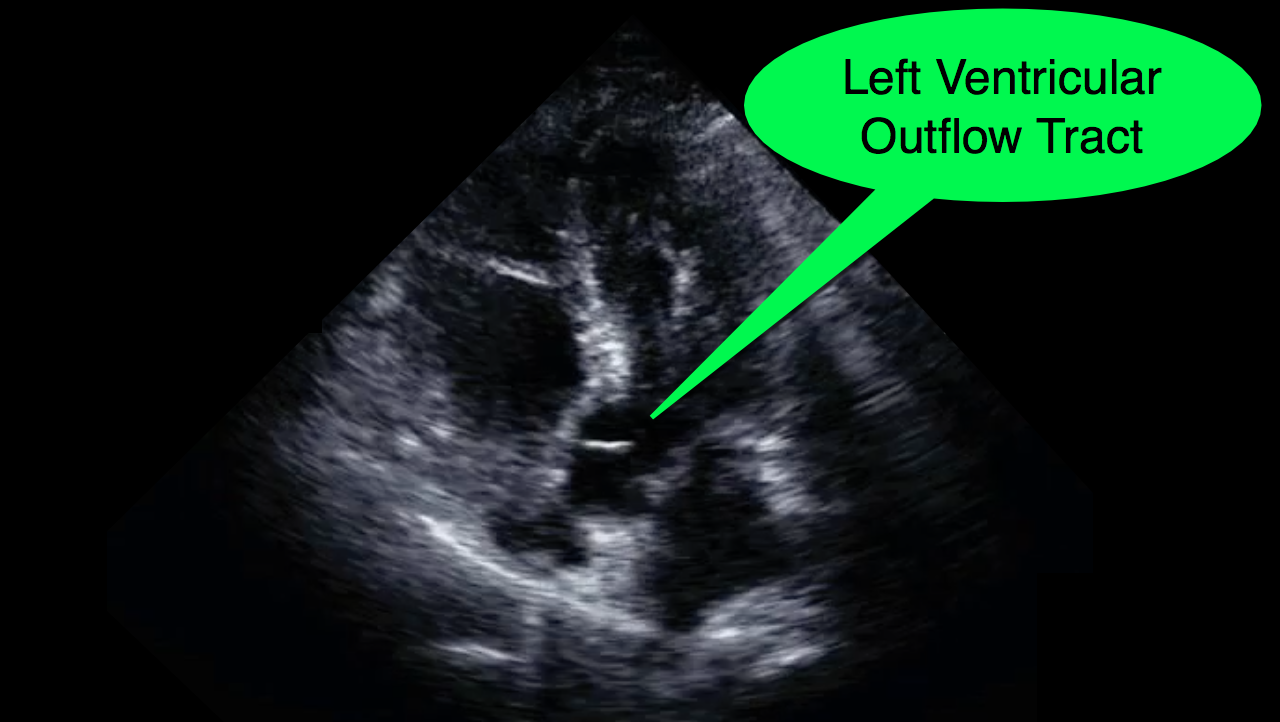
You decide to do a R.U.S.H. exam on your hypotensive patient and perform an apical four-chamber view.You see one of the two clips below; are there any tricks to figure out which is the left ventricle and which is the right ventricle?

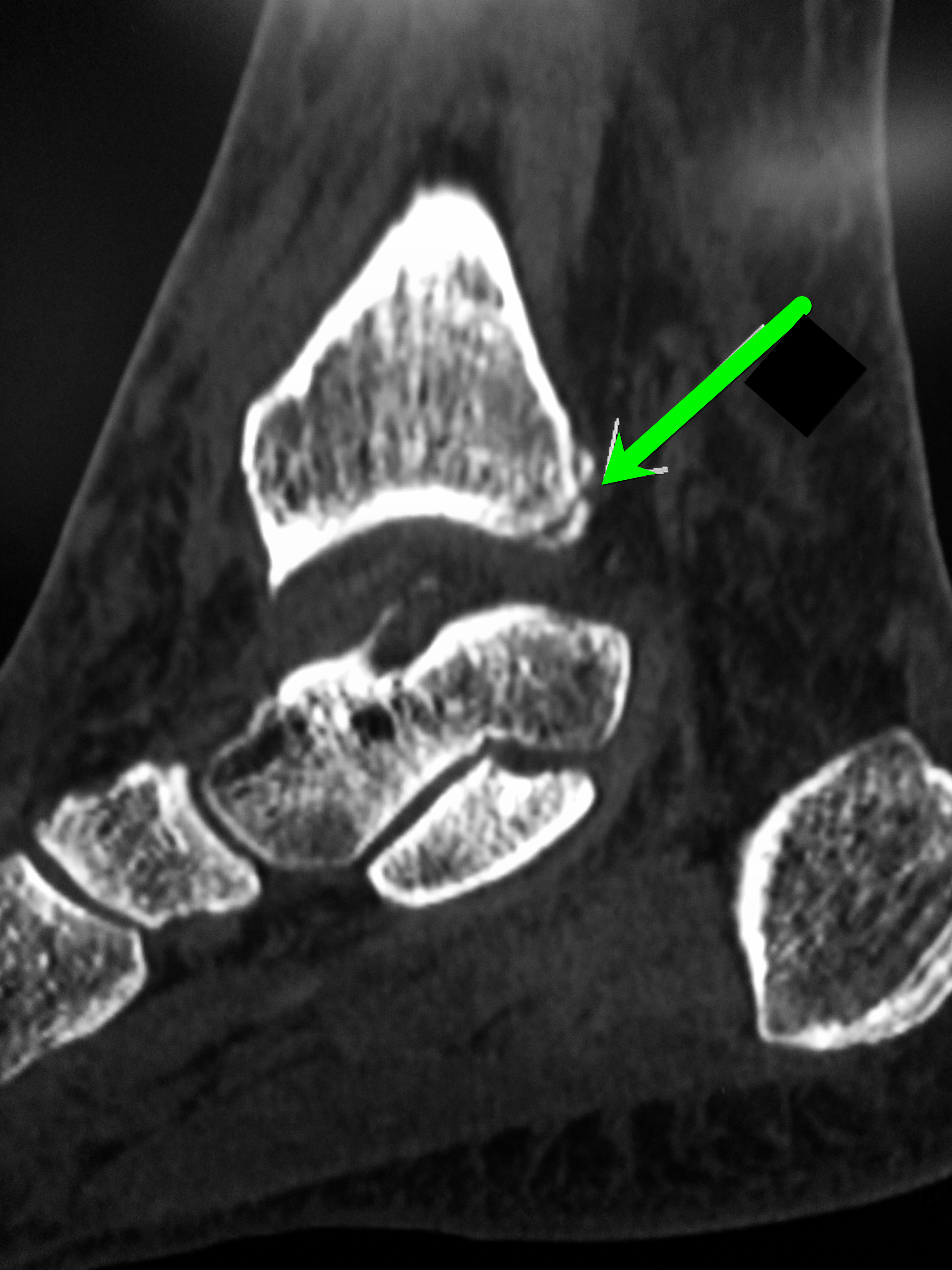
Patient presents with leg and ankle pain after a fall 3 weeks earlier. Initial ankle Xrays were negative. Patient presents today with persistent leg and ankle pain. What's the diagnosis and what other imaging would you perform and why?

A new study from South Korea identified 3 potential clinical predictors of developing delirium tremens in patients presenting to the ED with alcohol withdrawal seizures.
If one or more is present, these findings may help assess alcohol withdrawal patients for the risk of developing DTs.
Application to Clinical Practice
Prognostication in intracerebral hemorrhage - A self-fulfilling prophecy?
The ICH Score is a validated outcome prediction model for intracerebral hemorrhage (ICH) developed from clinical and neuroimaging characteristics on presentation.
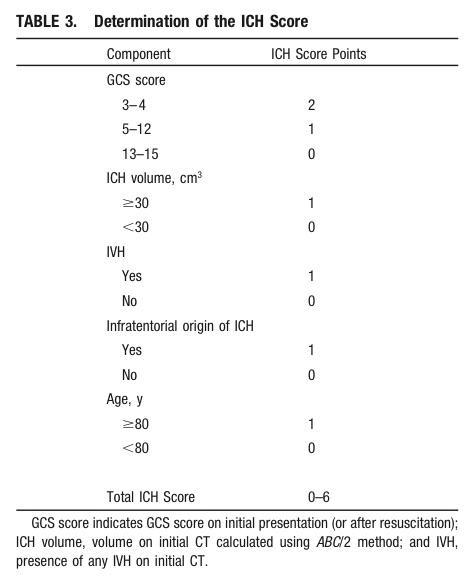
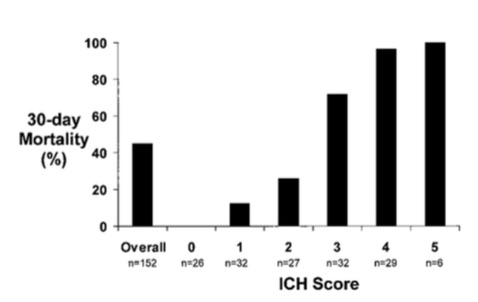
While predictive models are often used in clinical care for prognostication, is it a self-fulfilling prophecy to make early decisions to limit medical treatments based on these models?
Morgenstern et al. conducted an observational study across 5 hospitals looking at 30-day mortality of patients with ICH with initial GCS <12 who received full medical care for at least 5-days following symptom onset.
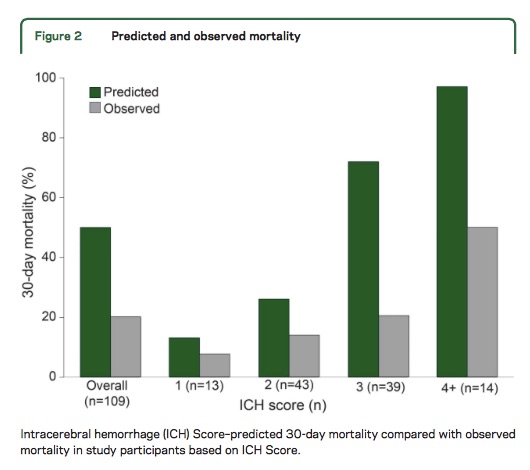
Take Home Point: The ICH Score is a useful tool for stratifying patient severity, but one should be cautious in using the model to provide specific numerical values as outcome predictions.
25 year-old male with the acute onset of right flank pain. Ultrasound of the right flank is shown. What's the diagnosis?
The Heart Is Just a Muscle
- Heart failure and peripheral myopathies share similar symptoms such as exertional fatigue, weakness, and dyspnea.
- The role of endomyocardial biopsy (EMB) to aid in the diagnosis of new-onset heart failure is controversial and major society guidelines recommend against this procedure in the routine evaluation of patients with heat failure.
- Nevertheless when symptoms of heart failure persist despite conventional imaging modalities and treatment one must consider uncommon conditions, such as mitochondrial disorders.
- Mitochondrial disorders are characterized as clinical syndromes and patients can present with any one of the following: ophthalmoplegia, proximal muscle weakness, isolated myopathy with exercise intolerance and myalgia, severe myopathy of infancy or childhood, or multisystem involvement with myopathy.
- Myocardial tissue is highly dependent on mitochondria for energy production and is therefore susceptible to defects in mitochondrial function. Cardiac manifestations of these syndromes include both arrhythmias and cardiomyopathy.
For many institutions, clindamycin is not as good as it used to be for methicillin-resistant Staph aureus (MRSA). When treating skin and soft tissue infections (SSTI), this can be challenging. Clindamycin still covers skin strep species very well, but not always the staph. On the other hand, trimethoprim-sulfamethoxazole (TMP-SMX) covers staph really well, but not so much the strep.
What They Did
A new double-blind, multicenter, randomized study in NEJM compared these two antibiotics in 524 patients with uncomplicated skin infections who had cellulitis, abscess larger than 5 cm, or both. All abscesses underwent incision and drainage. The primary outcome was clinical cure rate 7-10 days after the end of treatment.
What They Found
There was no difference in clinical cure rate between the two groups (80.3% for clindamycin, 77.7% for TMP-SMX).
Problems with the Study
Application to Clinical Practice
Unknown. This study seems to suggest TMP-SMX might be ok in uncomplicated cellulitis even though we assume strep species are the causitive organism. However, we already know cephalexin is equivalent to cephalexin + TMP-SMX from the 2013 study by Pallin et al. Why not just use cephalexin which has less adverse effects than TMP-SMX?
With such low clindamycin resistance, even to the staph species, perhaps that is why the two treatments were similar. Also, why did successfully drained abscesses need antibiotics? Finally, there were many exclusion criteria which eliminated many of the patients we see in the ED.
For a different, critical perspective of this NEJM study, Dr. Ryan Radecki gives his thoughts on his EM Lit of Note blog.