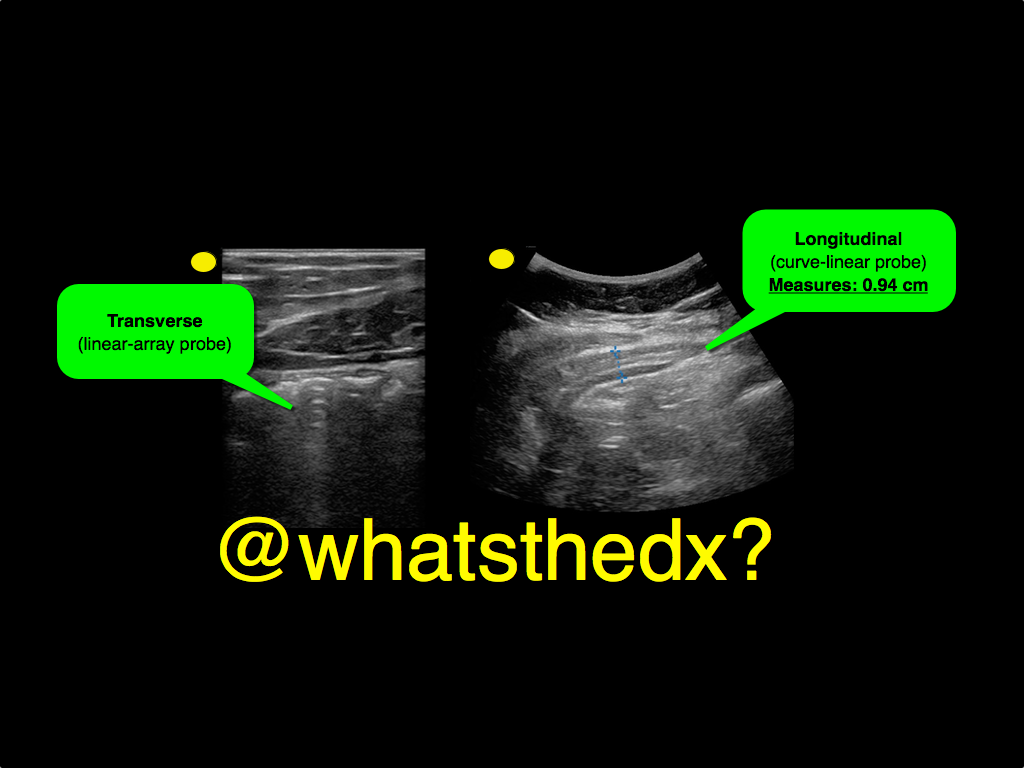
A male patient presents with right lower quadrant pain. The ultrasound is shown at the point of maximal tenderness. The diameter of the structure (image on right) is about 0.94cm. What is this structure and what's the diagnosis?
Are you comfortable with Intraosseous Catheter Placement in Children during a code? A pediatric code or child in distress is also distressing to care providers. Your staff may not feel comfortable with IO access in children. Read on to be more comfortable with your options as IO access in children can be difficult, especially the chubby toddlers. The basics for a patient in distress are "IV, O2, Monitor". Access is vital to giving resuscitation medications.
Indications for IO access: Any child in whom IV access cannot readily be obtained, but is necessary.
All IOs are 15G for infusion equal to central vascular access.
Different colors indicate different sizes:
Preferred sites:
Kids-do NOT use the sternum or distal radius
The reference from NEJM has videos to review placement and different tools (manual, EZ IO, and autoinjector).
Does IV magnesium have a role in the management of acute migraine headache in the ED? A new study says yes. [1]
Intervention
What They Found
Magnesium sulfate was more effective in decreasing pain severity at 20-min (pain scale 5.2 vs. 7.4) and 1-h (2.3 vs. 6.0) and 2-h (1.3 vs. 2.5) intervals after treatment (p < 0.0001) compared to treatment with dexamethasone/metoclopramide.
As you get ready to celebrate the coming of a new year, it is important to be safe while you are having a good time.
Injuries seen during holidays, such as new years, include:
If you are working, be ready to see increased alcohol and injury related visits.
If you are off and plan to celebrate, be sure to identify a designated driver or an alternate means of getting home.
Have a Happy and Safe 2015!
Cartoons Kill: A new high-risk patient for critical illness & death
This past month, the BMJ published an impressive retrospective review that analyzed nearly 80 years of data to find that animated characters in children’s films are in fact at a very high-risk for death when compared to characters in adult dramas.
Films ranged from 1937 (Snow White) to 2013 (Frozen) and were compared against the two highest gossing dramatic films in that same year. The authors found that nearly two thirds of the children’s animated films contained an on-screen death of an important character compared to only half in adult dramas.
Fatalities were most commonly the result of:
Other high-risk animated characters include the parents of the protagonist (17.8% mortality) and nemeses (28.9% mortality). Median survival time was approximately 90 minutes (much less than the usual ED LOS!)
Notable early on-screen deaths included Nemo’s mother being eaten by a barracuda 4 minutes into Finding Nemo, Tarzan’s parents being killed by a leopard 4 minutes into Tarzan, and Cecil Gaines’ father being shot in front of him 6 minutes into The Butler.
The author’s intention was to point out the psychological impact of death on young children, but I think the authors also highlight an important, high-risk patient population that could present to your ED.
Bottom Line: Animated characters should be aggressively resuscitated and strongly considered for admission to a higher level of care should they present to your ED, as they appear to be at high-risk for death and rapid decompensation.
May all of you have a happy and safe 2015!
Reference
1. Colman I, Kingsbury M, Weeks M, et al. CARTOONS KILL: casualties in animated recreational theater in an objective observational new study of kids' introduction to loss of life. BMJ. 2014;349:g7184.
Follow me on Twitter: @JohnGreenwoodMD
19 year-old male complaining of left arm pain one week after injecting anabolic steroids into his sholder. What's the diagnosis?
Holiday Heart
- Holiday heart commonly refers to alcohol use and rhythm disturbances, particularly supraventricular tachydysrhythmias.
- The most common rhythm disorder is atrial fibrillation (AF), which usually converts to normal sinus rhythm within 24 hours and antiarrhythmic therapy is typically not indicated.
- Analyses of ECGs in patients who have consumed a large quantity of alcohol show prolongation of the PR, QRS, and QT intervals.
- 2014 AHA/ACC/HRS updated guidelines for nonvalvular AF utilize the CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years [doubled], diabetes mellitus, prior stroke or TIA or thromboembolism [doubled], vascular disease, age 65 to 74 years, and sex category) score for assessment of stroke risk.
Knee Dislocation
Following reduction and immobilization, a thorough vascular assessment should follow. Any signs of vascular injury should prompt immediate vascular consultation (pallor, absent or diminished pulses)
1) Palpate popliteal and distal pulses
2) Measure ankle-brachial index (*ABI) (<0.9 = abnormal)
3) Duplex ultrasound (if available)
*ABI ratio of SBP in lower (DP/PT) and upper (brachial) extremities.
**Evaluation is often institutional specific. Discuss with your consultants.
A) If strong pulses normal ABI and normal u/s admit patient for observation with serial vascular examinations.
B) If the limb is still well perfused but the pulses are asymmetric or ABI is abnormal or US is abnormal then consult vascular surgery and obtain arteriogram (expanding role for CTA here).
C) If pulses are weak or absent or distal signs of ischemic limb then obtain emergent vascular consultation for surgical repair.
Cyanotic (right to left shunt) Congenital Heart Disease (CHD) lesions can be easily remembered with the 1,2,3,4,5 method.
1- Truncus Arteriosis (ONE trunk)
2- Transposition of the Great Vessels (TWO vessels flipped)
3- TRIcuspid Atresia
4-TETRAlogy of Fallot
5- Total Anomolous Pulmonary Venous Return (TAPVR=5 words/letters)
A few other important DUCTAL-DEPENDENT lesions: Coarctation of the Aorta, Hypoplastic Left Heart Syndrome, and Pulmonary Atresia.
Patients present to the emergency department within the first week of life in severe distress, including hypoxia, tachypnea, and hypotension. The above cyanotic CHD all reflect DUCTAL-DEPENDENT lesions, meaning they need a widely open PDA (which closes in the first week of life) to maintain sufficient oxygenation for viability.
These patients will not survive without timely intervention with prostaglandin (PGE1), so be sure to initiate this life-saving medication as soon as possible! Side effects include apnea…be prepared to intubate your neonate!
Delirium has long been recognized as a common disorder of the geriatric ED population (seen in up to 20% of patients above the age of 65 years), but how good are we at detecting it?
Studies show that the diagnosis of delirium is made in the ED in only 11-46% of patients, which means that more than half go undiagnosed. The problem is, the risk of death at 3 months increases by 11% for every 48 hours of delirium the patient experiences, and so does their length of stay and functional decline. It is mostly missed in patients who have a baseline cognitive dysfunction, such as dementia.
So what can we do about that?
Treat delirium as a neurolgical emergency; be vigilant about diagnosing it and treating it. There are a lot of neurocognitive tests that can be used for diagnosis (such as the mini-mental status exam), but they are usually too cumbersome to use in an ED setting. The CAM (Confusion Assessment Method) has been extensively studied and has a sensitivity and specifity of about 95% to diagnose delirium. It includes the acuity of onset, fluctuant course, inattention (the hallmark), disorganized thinking and/or altered level of consciousness.
Bottom Line? Don't forget to screen your elderly patients for delirium and treat them accordingly!
Treating ischemic strokes with interventional therapies (e.g., clot retrievers, stents, intra-arterial tPA, etc.) is nothing new, but there has never been a randomized control trial demonstrating benefit until recently.
The prospective MR CLEAN trial evaluated whether interventional therapies (i.e., either mechanical intervention or intra-arterial tPA) would confer benefit; patients were included if there was an acute occlusion within the proximal intracranial portion of the anterior cerebral circulation.
90% of patients received alteplase prior to randomization; there were 233 patients in the intervention group (alteplase + intraarterial intervention) and 267 patients in the usual care care arm (alteplase only); all patients were treated within 6 hours of symptoms onset
The primary outcome was functional independence at 90 days; an absolute difference of 13.5 percentage points favoring the intervention group was found. There were no significant differences in mortality or symptomatic intracerebral hemorrhage.
Despite these exciting results, we must pause and ask why this was this the first randomized trial demonstrating benefit when previous trials could not? Here are three blogs posts that deep dive this question and raise even more questions:
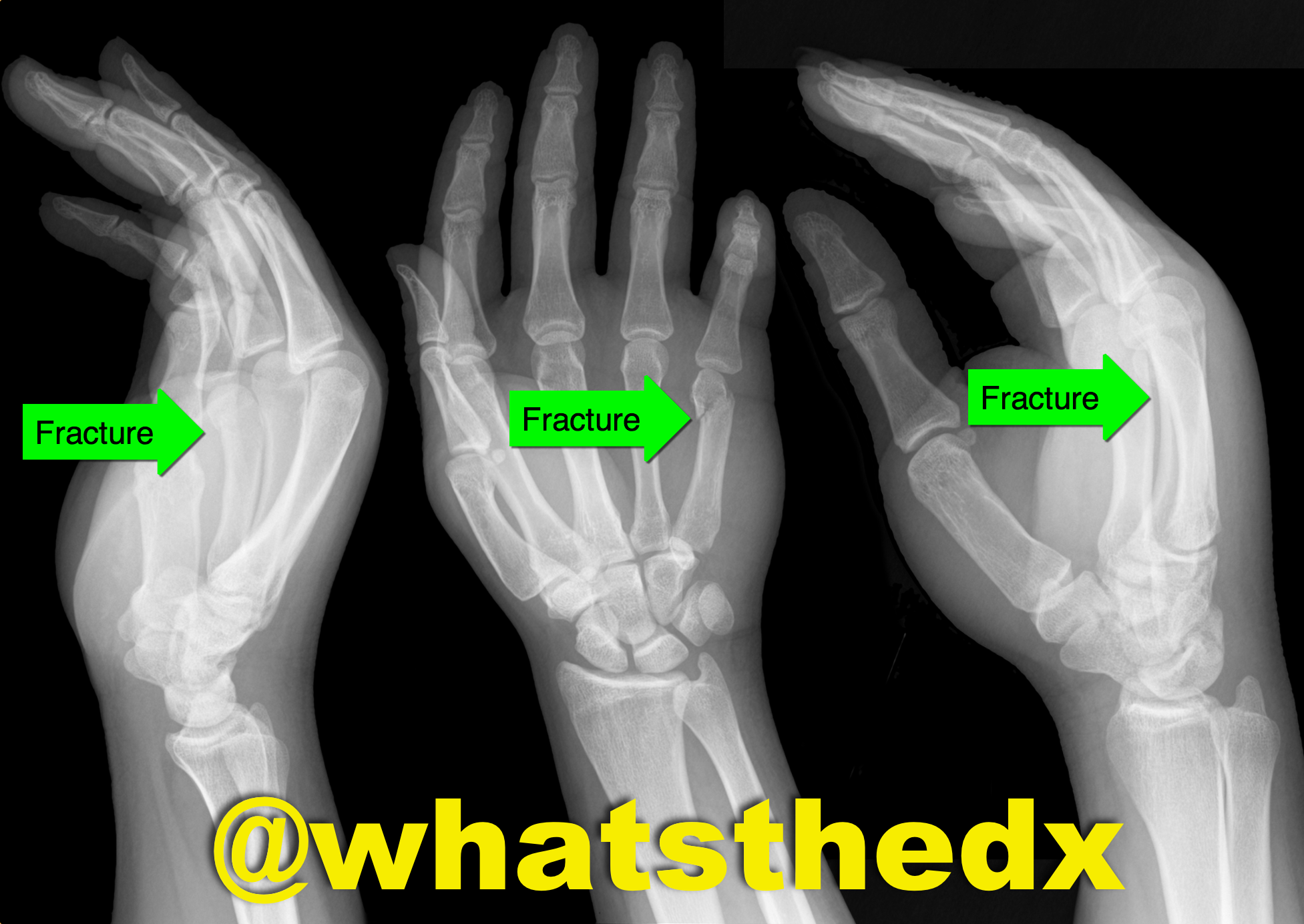
Hand pain following fist versus face. What's the diagnosis and what nerve block would you use?

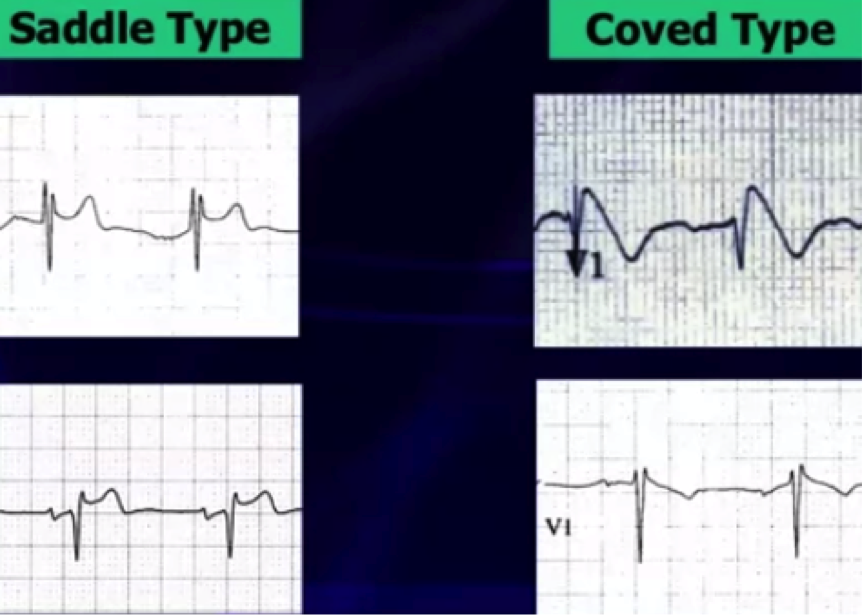
Brugada Syndrome
Brugada syndrome is an inherited arrhythmogenic channelopathy described by ST-segment elevation in the right precordial leads and an increased risk of sudden cardiac death.
There are 3 electrocardiographic patterns:
Type 1 – Coved morphology w/ST-elevation >2 mm, followed by a negative T wave in at least 1 right precordial lead
Type 2 - Saddleback morphology w/ST-elevation >2mm, with a positive or biphasic T wave
Type 3 - Either coved, or saddleback morphology with <2mm ST-elevation
Type 1 pattern is often underestimated because of its sporadic/fluctuating appearance on ECG, which can be either spontaneously occurring or drug-induced (drug-induced variant has a more favorable prognosis).
Fever has been a well-documented culprit in unmasking Brugada pattern by increasing the sodium channel dysfunction & accelerating the late sodium current inactivation.
A recent study in a large population of patients with type 1 Brugada attempted to identify other patterns unmasking Brugada using 24-hour holter monitoring. * There is now evidence that there is a higher prevalence of type 1 Brugada pattern from 12pm-6pm & unmasking by fast and a large meal, showing influence by glucose intake and insulin levels.
Now that respiratory season is upon us, we are faced with an increasing number of bronchiolitis children. The updated clinical practice guidelines for managing these kids were recently published and emphasize supportive care only.
Some of the key points:
-When clinicians diagnose bronchiolitis on the basis of history and physical examination, radiographic or laboratory studies should not be obtained routinely.
-Medications such as albuterol, nebulized epinephrine or steroids should not be administered routinely in children with a diagnosis of bronchiolitis.
-Nebulized hypertonic saline should not be administered to infants with a diagnosis of bronchiolitis in the emergency department
-Clinicians may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90% in infants and children with a diagnosis of bronchiolitis
-Clinicians may choose not to use continuous pulse oximetry for infants and children with a diagnosis of bronchiolitis.
Check out the full guidelines for the quality of evidence and rational behind these recommendations.
The bottom line is that not much really works, and we just need to support their respiratory effort and ensure hydration.
It is believed that administration of beta-blocker administration in patients with cocaine chest pain will produced increased vasoconstriction due to “unopposed alpha effect.”
Several retrospective studies on the use of beta-blocker in patients with cocaine-induced chest pain concluded the use of beta-blocker to be safe.
So is the unopposed alpha effect just a theory?
Lange RA et al. 1990 Ann Internal Med
Design: randomized, double-blind, placebo controlled trial.
30 (38- 68 years old) patients undergoing cardiac catherization for chest pain evaluation were studied.
Cocaine (intranasal administration) resulted in:
Administration of propranolol (intracoronary infusion) resulted in additional:
Complete coronary occlusion observed in 1 patient with ST elevation
Epicardial coronary arterial segment constriction >10% in 5 patients.
Bottom Line: Lange RA et al. 1990 demonstrates that the “unopposed alpha effect” does occur in coronary artery when beta-blocker is administered in a setting of acute cocaine exposure. Overall, the use of beta-blocker in the ED management of cocaine-induce acute chest pain is not a prudent option. It is unknown if the cocaine dose, last use of cocaine (days), or CAD history influence the “safety” of beta-blocker initiation/use during inpatient hospitalization.
Background: As discussed previously, influenza (flu) is a common respiratory disease that causes significant morbidity and mortality worldwide (see pearl from October 1. 2014). We are now in the midst of the current flu season.
Current Update: This year’s vaccine was only a partial match (<50%) for the current influenza A (H3N2) circulating virus, so there is a significant potential for a “bad” flu season with widespread disease and severe illness. Currently, influenza is now widespread throughout the US, with some states reporting more activity than others. The CDC has a weekly surveillance map that highlights current disease spread.
Bottom Line:
How does it present?
Who cares…I got my vaccine! Does the vaccine work this year?
Can I test for this?
The CDC is recommending treatment...wait I thought we were done with Tamiflu?
Who is at risk/who deserves consideration for treatment?
Pearls of treatment
What are the side effects of anti-viral agents?
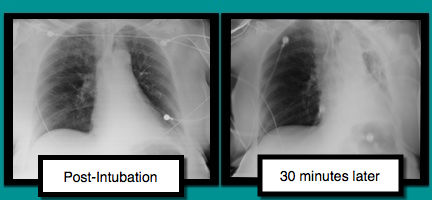
A patient is intubated for respiratory failure and the post-intubation CXR is shown on the left. 30 minutes later the patient desaturates and another CXR is obtained (the one on the right). What’s the diagnosis and what should you do?
Not So Benign: Benign early repolarization (BER) effects in STEMI
- Benign early repolarization (BER) has been associated with increased risk of sudden cardiac death and ventricular fibrillation (VF) in patients with and without structural heart disease.
- Acute STEMI is associated with high incidence of ventricular arrhythmias and the most frequent cause of sudden cardiac death in the adult population.
- BER has been associated with arrhythmogenicity, however the prognostic importance of this ECG finding in patients with STEMI has not been well elucidated.
- In a recent prospective study of STEMI patients, BER was associated with higher rates of in-hospital ventricular arrhythmias and mortality; It is an independent predictor of long-term mortality beyond well-known other parameters.