What is a massive transfusion?
When would I use this?
Indications:
-Systolic Blood pressure < 100
-Unable to obtain blood pressure
AND
-Penetrating torso trauma
-Positive FAST
-External blood loss
-Plans to go to the OR
How do I give it?
Does this apply for just traumatic bleeding?
Are there other agents I can use?
What am I trying to do with this protocol?
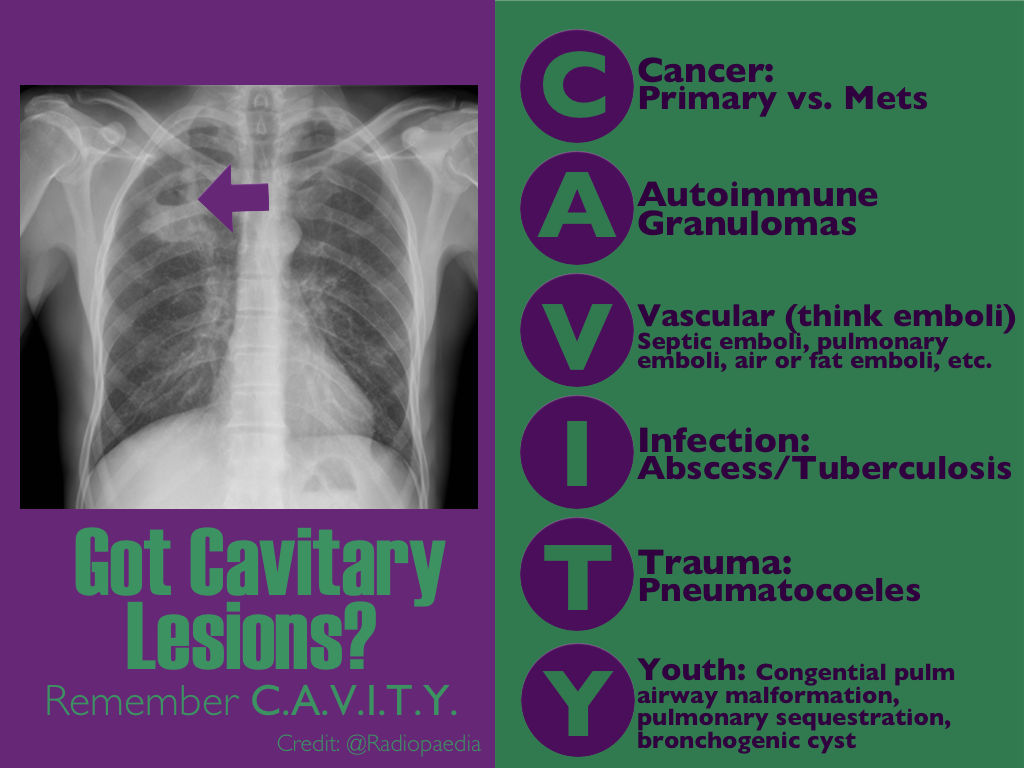
16 yo M with pleuritic right upper chest pain that started today. He is suffering from an asthma exacerbation currently in the setting of URI with cough. He is afebrile, tachycardic to 140-150s, respiratory rate 20, and sats 98% on room air. ECG was performed which incidentally diagnosed this patient WPW and he went for ablation as an outpatient. His chest x-ray showed:
Besides a bad day, what do we call this chest x-ray finding?
Tendon Lacerations:
A reasonable approach to all tendon lacerations is to loosly reapproximate the wound and splint the hand in the position of function until the patient can be seen by a hand surgeon in the next 1-3 days. These injuries do not require immediate surgical repair, and with the high rate of complications it is probably best to discuss with your hand surgeon before attempting a repair.
The NEXUS criteria is widely applied to adults who present with neck pain due to trauma. While this study did include about 2000 pediatric patients, there were not enough young children to draw definitive conclusions. For more information on the evaluation of the cervical spine, see Dr. Rice's pearl from 9/7/12. A 2003 study piloted an algorithm for cervical spine clearance in children < 8 years.
Patients were spine immobilized if: unconscious, abnormal neurological exam, history of transient neurological symptoms, significant mechanism of injury, neck pain, focal neck tenderness or inability to assess based on distracting injury (extremity or facial fractures, open wound, thoracic injuries, or abdominal injuries), physical exam findings of neck trauma, unreliable exam due to substance abuse, significant trauma to the head or face, or inconsolable children.
When the 2 pathways (see attached) were implemented, there was a decrease in time to cervical spine clearance. There were no missed injuries in the study period prior to implementation of the pathway or once it was implemented. There was no significant difference in the amount of xrays, CT scans or MRIs.
Food poisoning can occur with many different food groups/items, as well as how the food is prepared, handled or stored.
There are three specific “food poisonings” associated with fish consumption can cause serious toxicity/illness beyond GI symptoms: Ciguatera, Scrombroid, tetrodotoxin (puffer fish)
Ciguatera
Symptoms:
May progress to develop…
Treatment: supportive care and mannitol in presence of severe neurologic symptoms (limited evidence).
Scrombroid
Symptoms:
Tx: H1/H2 blockers and supportive care
Serious reactions: treat like allergic/anaphylactic reaction
Tetrodotoxin
Symptoms:
Treatment: supportive care and intubated if needed.
While sitting on an international flight, ever wonder what your risks are for a blood clot?
General Background:
It is estimated that the risk for a deep venous thrombosis (DVT) is 3-12% on a long-haul flight. However, the real incidence is difficult to evaluate, due in part to the lack of consensus about 1) diagnostic tests, and 2) the appropriate time frame to relate a venous thromboembolic event (VTE) to travel.
Risks Factors for VTEs on long-haul flights:
Bottom Line:
Infectious Risks Associated with TTM
Football player complains of sudden foot pain after begin tackled. What’s the diagnosis?

Optimal Revascularization in Complex Coronary Artery Disease
- A multicenter trial 4,566 patients with NSTEMI, unstable angina, and multi-vessel coronary artery disease were enrolled comparing outcomes of cardiac stenting versus coronary artery bypass.
- Cardiac stenting was associated with improved outcomes and lower mortality in the following subgroups: age >65 years, women, unstable angina, TIMI score >4, and 2 vessel disease.
- Despite high clinical risk patients who underwent cardiac stenting compared to surgical revascularization did better in this prospective registry.
Back pain accounts for more than 2.6 million visits
30% of ED patients receive X-rays as part of their evaluation
Imaging can be avoided in a majority of these patients by focusing on high risk (red flags) findings in the history and physical exam.
Patients who can identify a an acute inciting event without direct trauma likely have a MSK source of pain.
Imaging rarely alters management
Attempt to avoid imaging in patients with nonspecific lower back pain of less than 6 weeks duration, with a normal neurologic exam and without high risk findings (fever, cancer, IVDA, bowel or bladder incontinence, age greater than 70, saddle anesthesia, etc)
Patients with radiculopathy (sciatica) and are otherwise similar to the above also do not require emergent imaging
Digoxin-specific antibody fragments (Fab) are safe and indicated in all patients with life-threatening dysrhythmias and an elevated digoxin concentration. However, full neutralizing doses of digoxin-Fab are expensive and may not be required (not to mention cumbersome to calculate).
Based on pharmacokinetic modeling and published data, a new review suggests a simpler, more stream-lined dosing scheme as follows:
In imminent cardiac arrest, it may be justified to give a full neutralizing dose of digoxin-Fab.
In acute poisoning, a bolus of 80 mg (2 vials), repeat if necessary, titrated against clinical effect, is likely to achieve equivalent benefits with much lower total doses.
With chronic poisoning, it may be simplest to give 40 mg (1 vial) at a time and repeat after 60 min if there is no response.
Why is everyone obsessed about blood pressure management in stroke?
Greater than 60% of patients with stroke have elevated blood pressure, and 15% have a systolic blood pressure (SBP) greater than184 mmHg. That is more common in hemorrhagic stroke than ischemic stroke.
Whether it's an acute hypertensive response or a premorbid uncontrolled hypertension, it is likely to negatively affect the clinical course and neurological outcome.
Below is a suumary of the current guidelines for blood pressure management of stroke subtypes; for a more detailed summary of the guidelines, refer to the original article (below)
Ischemic stroke:
Lytic patients have a target SBP of <185mmHg, whereas nonlytic patients have a higher SBP target of <220mmHg
Hemorrhagic Stroke:
Non-aneurysmal hemorrhage patients with a SBP >180mmHg have a target SBP of <160 mmHg, whereas if their SBP was 150-220 mmHg then lowering it to 140 mmHg is safe. Patients with aneurysmal hemorrhage have a target SBP of <160mmHg
Goal-Directed Resuscitation During Cardiac Arrest
Focusing on high-quality CPR is by far one of the most effective methods to ensure your arrested patient has the best chance to survive. However, emerging evidence suggests that there are additional goals that we should try and accomplish during our resuscitation.
As we continue to move toward goal-directed resuscitation strategies, optimizing coronary perfusion pressure (CPP) may be our next target in “personalizing” the care we provide to those in cardiac arrest.
A recent AHA consensus statement recommended the following physiologic goals during cardiac arrest care:
Each of these variables can give the provider valuable feedback about how their patient is responding to their resuscitation. Some argue that the DBP target should be much higher (>35 mmHg), with the caveat that pharmacologic optimization can only occur once high quality CPR is confirmed. The goal should always be to minimize the use of epinephrine whenever possible!
Bottom Line: During your next cardiac arrest resus, consider using a goal-directed strategy by monitoring the patient’s CPP, DBP, & EtCO2 to determine the effectiveness of your resuscitation.
Suggested Reading
Follow me on Twitter @JohnGreenwoodMD
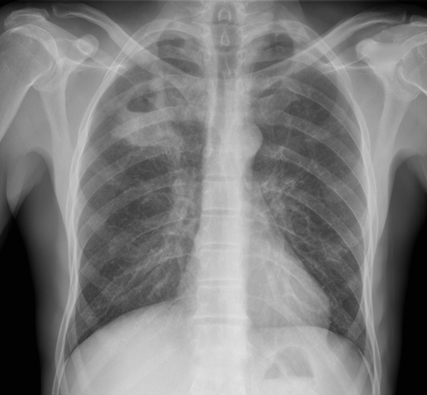
CXR shown below, what's the diagnosis? ...and name 3 differential diagnoses.
PARADIGM Shift in Heart Failure
- Angiotensin-converting enzymes inhibitors (ACE-I) are cornerstone for treatment of heart failure (HF) given the multiple trials which have shown their positive risk reduction in cardiovascular death.
- Studies looking at the effect of angiotensin-receptor blockers (ARBs) on mortality have been inconsistent; thus ARB's have been recommended as 2nd-line for those who have unacceptable side effects to ACE-I.
- A recent double-blinded RCT (PARADIGM-HF) ~8400 patients with class II-IV HF w/ ejection fraction <40% were treated with enalapril (standard therapy) versus novel therapy with neprilysin (neutral endopeptidase) inhibitor combined with an ARB.
- Primary outcomes were death from cardiovascular causes and hospitalization for HF; The RCT was ceased early (~27 months) because of an overwhelming benefit with the new agent.
- At study closure death occurred 26.5% in the standard group versus 21.8% in the novel group. The risk of HF hospitalization was decreased 21% with novel therapy.
- In early studies the use of a neprilysin inhibitor combined with an ARB has shown superior effects to current standard therapy (ACE-I), however long-term effects of this novel therapy are yet to be determined.
In May 2014, the U.S. Public Health Service released the first comprehensive clinical practice guidelines for PrEP.
Pre-Exposure Prophylaxis (PrEP) has been shown to decrease the risk of HIV infection in people who are at high risk by up to 92%, if taken consistently.
How this applies to the ED patient:
For more information, the CDC has a comprehensive website dedicated to PrEP.
Dysrhythmia-induced sudden death, termed "sudden sniffing death syndrome," is well described phenomena due to inhalant (chlorinated and aromatic hydrocarbon) abuse.
Common inhalants include:
Chlorinated hydrocarbons: Degreasers, spot removers, dry-cleaning agents
Fluorocarbons: Freon gas, deodarants
Toluene: Paint thinners, spray paint, airplane glue
Butane: Lighter fluid, fuel
Acetone: Nail polish remover
The common theory behind the syndrome is cardiac sensitization that increases susceptibility of the heart to systemic catecholamines (epinephrine, norepinephrine, etc). Usually, it occurs after an episode of exertion in that any excess catecholamine exposure causes irritability of the myocardium, resulting in dysrhythmias (V. fib, V. tach) and cardiac arrest.
If acute dysrhythmias is due to myocardial sensitization, sympathomimectis should be avoided. Beta-adrenergic antagonist can be used for the catecholamine-sensitized heart.
Hyperthermia can be defined as a core body temperature > 38.5ºC. In contrast to fever, the body’s temperature rises uncontrollably and the body is not able to dissipate the heat. There can be many causes of hyperthermia, including from environmental exposure.
There are two main environmental heat illnesses, heat exhaustion and heat stroke.
Heat exhaustion:
Heat stroke
Bottom line:
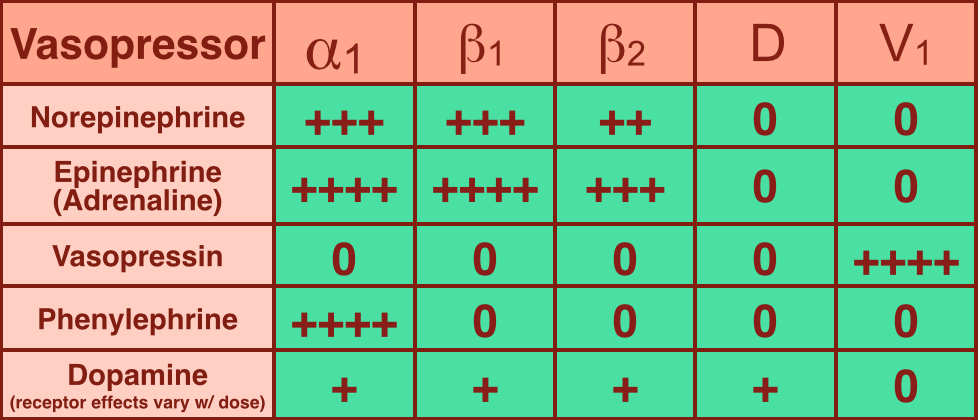
Vasopressors are used in shock-states to increase mean arterial pressure (MAP) and improve distal tissue perfusion. Additionally, some agents have effects on the heart to augment cardiac output.
Receptors that vasopressors work on include:
Norepinephrine (NE): excellent vasopressor for most types of shock and recommended as a first-line agent in the Surviving Sepsis Guidelines.
Epinephrine (a.k.a. Adrenaline): in several countries the first-line agent for shock (including sepsis).