Treating ischemic strokes with interventional therapies (e.g., clot retrievers, stents, intra-arterial tPA, etc.) is nothing new, but there has never been a randomized control trial demonstrating benefit until recently.
The prospective MR CLEAN trial evaluated whether interventional therapies (i.e., either mechanical intervention or intra-arterial tPA) would confer benefit; patients were included if there was an acute occlusion within the proximal intracranial portion of the anterior cerebral circulation.
90% of patients received alteplase prior to randomization; there were 233 patients in the intervention group (alteplase + intraarterial intervention) and 267 patients in the usual care care arm (alteplase only); all patients were treated within 6 hours of symptoms onset
The primary outcome was functional independence at 90 days; an absolute difference of 13.5 percentage points favoring the intervention group was found. There were no significant differences in mortality or symptomatic intracerebral hemorrhage.
Despite these exciting results, we must pause and ask why this was this the first randomized trial demonstrating benefit when previous trials could not? Here are three blogs posts that deep dive this question and raise even more questions:
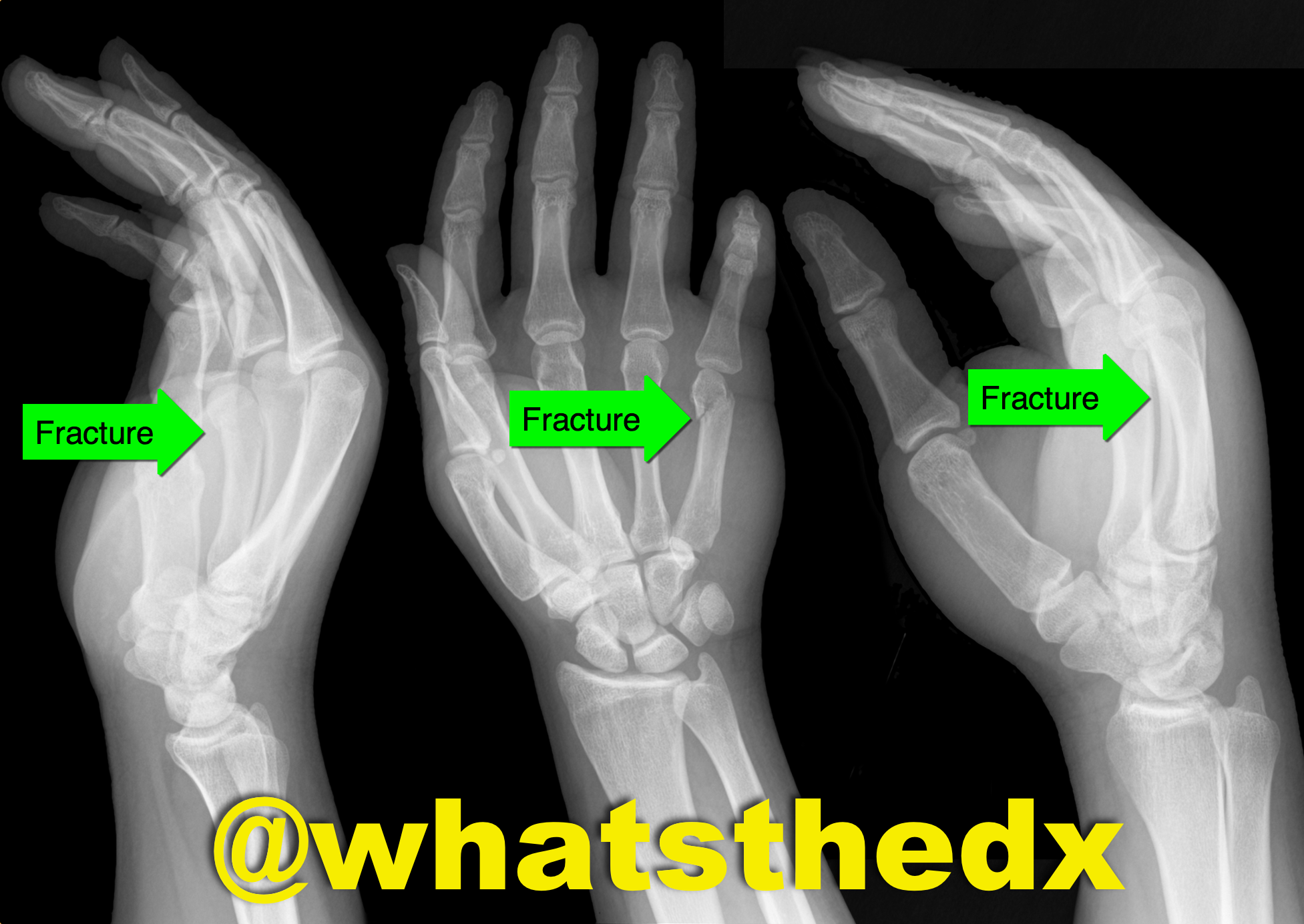
Hand pain following fist versus face. What's the diagnosis and what nerve block would you use?

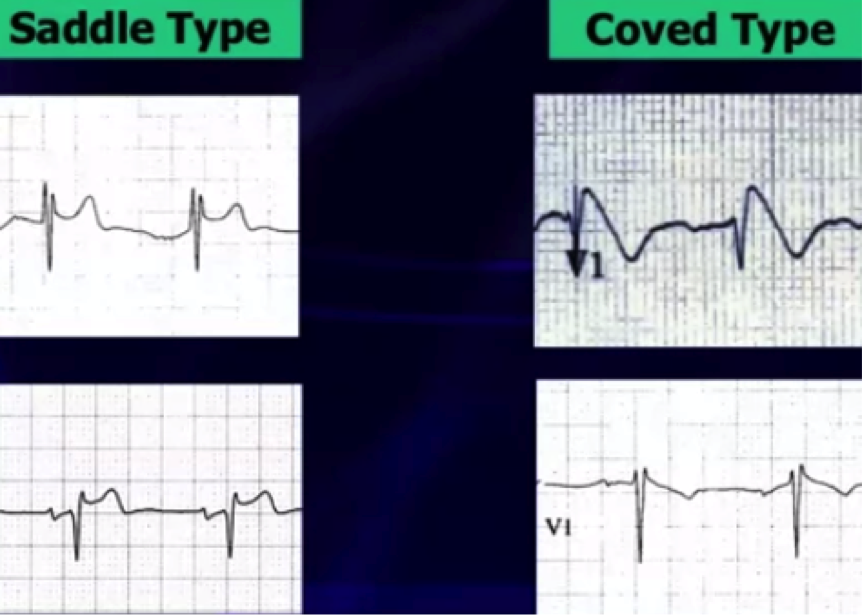
Brugada Syndrome
Brugada syndrome is an inherited arrhythmogenic channelopathy described by ST-segment elevation in the right precordial leads and an increased risk of sudden cardiac death.
There are 3 electrocardiographic patterns:
Type 1 – Coved morphology w/ST-elevation >2 mm, followed by a negative T wave in at least 1 right precordial lead
Type 2 - Saddleback morphology w/ST-elevation >2mm, with a positive or biphasic T wave
Type 3 - Either coved, or saddleback morphology with <2mm ST-elevation
Type 1 pattern is often underestimated because of its sporadic/fluctuating appearance on ECG, which can be either spontaneously occurring or drug-induced (drug-induced variant has a more favorable prognosis).
Fever has been a well-documented culprit in unmasking Brugada pattern by increasing the sodium channel dysfunction & accelerating the late sodium current inactivation.
A recent study in a large population of patients with type 1 Brugada attempted to identify other patterns unmasking Brugada using 24-hour holter monitoring. * There is now evidence that there is a higher prevalence of type 1 Brugada pattern from 12pm-6pm & unmasking by fast and a large meal, showing influence by glucose intake and insulin levels.
Now that respiratory season is upon us, we are faced with an increasing number of bronchiolitis children. The updated clinical practice guidelines for managing these kids were recently published and emphasize supportive care only.
Some of the key points:
-When clinicians diagnose bronchiolitis on the basis of history and physical examination, radiographic or laboratory studies should not be obtained routinely.
-Medications such as albuterol, nebulized epinephrine or steroids should not be administered routinely in children with a diagnosis of bronchiolitis.
-Nebulized hypertonic saline should not be administered to infants with a diagnosis of bronchiolitis in the emergency department
-Clinicians may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90% in infants and children with a diagnosis of bronchiolitis
-Clinicians may choose not to use continuous pulse oximetry for infants and children with a diagnosis of bronchiolitis.
Check out the full guidelines for the quality of evidence and rational behind these recommendations.
The bottom line is that not much really works, and we just need to support their respiratory effort and ensure hydration.
It is believed that administration of beta-blocker administration in patients with cocaine chest pain will produced increased vasoconstriction due to “unopposed alpha effect.”
Several retrospective studies on the use of beta-blocker in patients with cocaine-induced chest pain concluded the use of beta-blocker to be safe.
So is the unopposed alpha effect just a theory?
Lange RA et al. 1990 Ann Internal Med
Design: randomized, double-blind, placebo controlled trial.
30 (38- 68 years old) patients undergoing cardiac catherization for chest pain evaluation were studied.
Cocaine (intranasal administration) resulted in:
Administration of propranolol (intracoronary infusion) resulted in additional:
Complete coronary occlusion observed in 1 patient with ST elevation
Epicardial coronary arterial segment constriction >10% in 5 patients.
Bottom Line: Lange RA et al. 1990 demonstrates that the “unopposed alpha effect” does occur in coronary artery when beta-blocker is administered in a setting of acute cocaine exposure. Overall, the use of beta-blocker in the ED management of cocaine-induce acute chest pain is not a prudent option. It is unknown if the cocaine dose, last use of cocaine (days), or CAD history influence the “safety” of beta-blocker initiation/use during inpatient hospitalization.
Background: As discussed previously, influenza (flu) is a common respiratory disease that causes significant morbidity and mortality worldwide (see pearl from October 1. 2014). We are now in the midst of the current flu season.
Current Update: This year’s vaccine was only a partial match (<50%) for the current influenza A (H3N2) circulating virus, so there is a significant potential for a “bad” flu season with widespread disease and severe illness. Currently, influenza is now widespread throughout the US, with some states reporting more activity than others. The CDC has a weekly surveillance map that highlights current disease spread.
Bottom Line:
How does it present?
Who cares…I got my vaccine! Does the vaccine work this year?
Can I test for this?
The CDC is recommending treatment...wait I thought we were done with Tamiflu?
Who is at risk/who deserves consideration for treatment?
Pearls of treatment
What are the side effects of anti-viral agents?
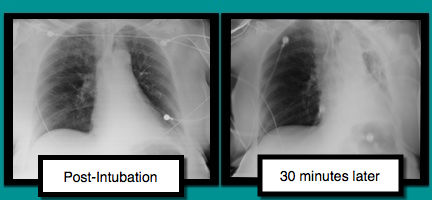
A patient is intubated for respiratory failure and the post-intubation CXR is shown on the left. 30 minutes later the patient desaturates and another CXR is obtained (the one on the right). What’s the diagnosis and what should you do?
Not So Benign: Benign early repolarization (BER) effects in STEMI
- Benign early repolarization (BER) has been associated with increased risk of sudden cardiac death and ventricular fibrillation (VF) in patients with and without structural heart disease.
- Acute STEMI is associated with high incidence of ventricular arrhythmias and the most frequent cause of sudden cardiac death in the adult population.
- BER has been associated with arrhythmogenicity, however the prognostic importance of this ECG finding in patients with STEMI has not been well elucidated.
- In a recent prospective study of STEMI patients, BER was associated with higher rates of in-hospital ventricular arrhythmias and mortality; It is an independent predictor of long-term mortality beyond well-known other parameters.
Should beta blockers be withheld in cocaine-chest pain patients?
A new study retrospectively compared patients who received beta blockers as an inpatient to those who did not. Even though the beta blocker group had higher risk clinical characteristics, there was no difference in the composite primary end point of myocardial infarction, stroke, ventricular arrhythmia, or all-cause mortality within 24 hours of beta blocker use.
Important Limitations
The potentially dangerous interaction between beta blockers and cocaine is likely a much larger issue in patients with very recent cocaine use in the setting of a catecholamine surge. A retrospective analysis likely doesn't include those patients.
Application to Clinical Practice
While this study doesn't answer the question about beta blocker use in acute cocaine toxicity, it does provide some reassurance about the safety of beta blockers given for cocaine-related chest pain.
Does clinical decision support help reduce head CT utilization in mild traumatic brain injury related ED visits?
Are we utilizing clinical decision rules adequately to help us appropriately select patients for CT imaging?
Can clinical decision support (CDS) help us reduce head CT utilization in mTBI related ED visits?
Take Home Point:
Clinical decision support may be a useful tool to help reduce CT utilization in mild TBI related ED visits.
The Critically Ill Patient with Ebola Virus Disease
Patient was found in a house fire and was given a certain medication in the Emergency Room. The patient’s urine turned this color (red), what’s the diagnosis?

Predictors of Cardiac Rupture After AMI
- In the era of revascularization and aggressive cardiac care there has been a continual decline in acute myocardial infarction (AMI) mortality rates; however one of the most deadly complications, cardiac rupture (left ventricular free wall, ventricular septum, or papillary muscle rupture), still remains relatively stable.
- Cardiac rupture is an increasingly more frequent cause of death during AMI, thus a recent study retrospectively assessed the clinical and morphologic variables in those with and without cardiac rupture that were hospitalized for AMI.
- Cardiac rupture overwhelmingly complicates a first AMI.
- Cardiac rupture occurs most often in patients with an immense quantity of cardiac adipose tissue, the size of the left ventricular cavity is typically normal, and the area of the infarct is small.
- Heart failure patients with prior AMI have healed scar tissue and are at nominal risk of complications such as rupture if a subsequent AMI occurs.
Many of the oral antibiotics prescribed in the ED have good bioavailability. So, a one-time IV dose before discharge generally won't provide much benefit.
In fact, a new prospective study found that a one-time IV antibiotic dose before ED discharge was associated with higher rates of antibiotic-associated diarrhea and Clostridium difficile infection. [1] One-time doses of vancomycin for SSTI before ED discharge are also not recommended (see Academic Life in EM post).
Bottom Line
Though there are a few exceptions, if a patient has a working gut, an IV dose of antibiotics before ED discharge is generally not recommended and may cause increased adverse effects. An oral dose is just fine.
Sympathomimetic toxicity is a known toxidrome that is complicated by the development of rhabdomyolysis. There are multiple stimulant agents that induce sympathomimetic toxicity including, synthetic cathinones, cocaine, amphetamines, and methamphetamines.
A recent retrospective, single-center, chart review in the age range of 14-65 years sought to determine the prevalence of rhabdomyolysis in patients with sympathomimetic toxicity and compare rates among patients using specific agents. Rhabdomyolysis and severe rhabdomyolysis were defined as CK>1000 and 10,000 IU/L, respectively.
Rhabdomyolysis occurred in 42% of study subjects (43/102)
Prevalence in 89 subjects due to a single-stimulant exposure:
Rhabdomyolysis
1) Synthetic cathinone (MDPV, alpha-PVP) 63% (12/19)
2) Methamphetamine 40% (22/55)
3) Cocaine 33% (3/9)
4) Other single agents (methylphenidate, pseudoephedrine, phentermine) 0% (0/6)
Severe Rhabdomyolysis
1) Synthetic cathinone 26% (5/19)
2) Methamphetamine 3.6% (2/55)
3) Cocaine 11% (1/9)
4) Other single agents (methylphenidate, pseudoephedrine, phentermine) 0% (0/6)
In this study, patients exposed to synthetic cathinones were more likely to develop rhabdomyolysis and severe rhabdomyolysis compared to the non-cathinone-exposed group.
Bottom Line:
Be aware of this increased risk from synthetic cathinones along with other stimulants. Treat aggressively with IV fluids, rapid correction of hyperthermia, benzodiazepines to control manifestations of sympathomimetic toxicity to reduce muscle activity and metabolic demand.
In December 2013, Academic Emergency Medicine published the results of the 2013 consensus conference that focused on advancing global health and emergency care research.
As noted in the issue’s executive summary, “Emergency physicians are uniquely poised to address challenges in health services, health care systems development and management, and emerging global disease burdens (both communicable and noncommunicable). “
The consensus conference covered developing research in eight focus areas, including understanding of cardiac and injury resuscitation, ethics of research, health systems development, and the education of future global health leaders.
For anyone interested in global health and emergency care, this issue of Academic Emergency Medicine is an outstanding resource and roadmap to developing research. It can be found at: http://onlinelibrary.wiley.com/doi/10.1111/acem.2013.20.issue-12/issuetoc
Dynamic Measures of Intravascular Volume Assessment
The resuscitation of a patient in shock often requires the administration of intravenous fluid. Excessive fluid resuscitation can lead to worsening pulmonary edema, systemic edema, acid-base disturbances, as well as many other complications. There are a myriad of techniques to try and figure out if the patient needs more intravascular volume, but each has it’s pitfalls.
Recently, experts have recommend that we move away from using static measures of preload assessment such as central venous pressure (CVP) and instead focus on using dynamic measures for volume responsiveness.
Volume Responsiveness Defined: An increase of stroke volume of 10-15% after a 500 mL IV crystalloid bolus over 10-15 minutes.
Below is a chart describing key values, requirements, and contraindications for each of these dynamic measures of non-invasive intravascular volume assessment.
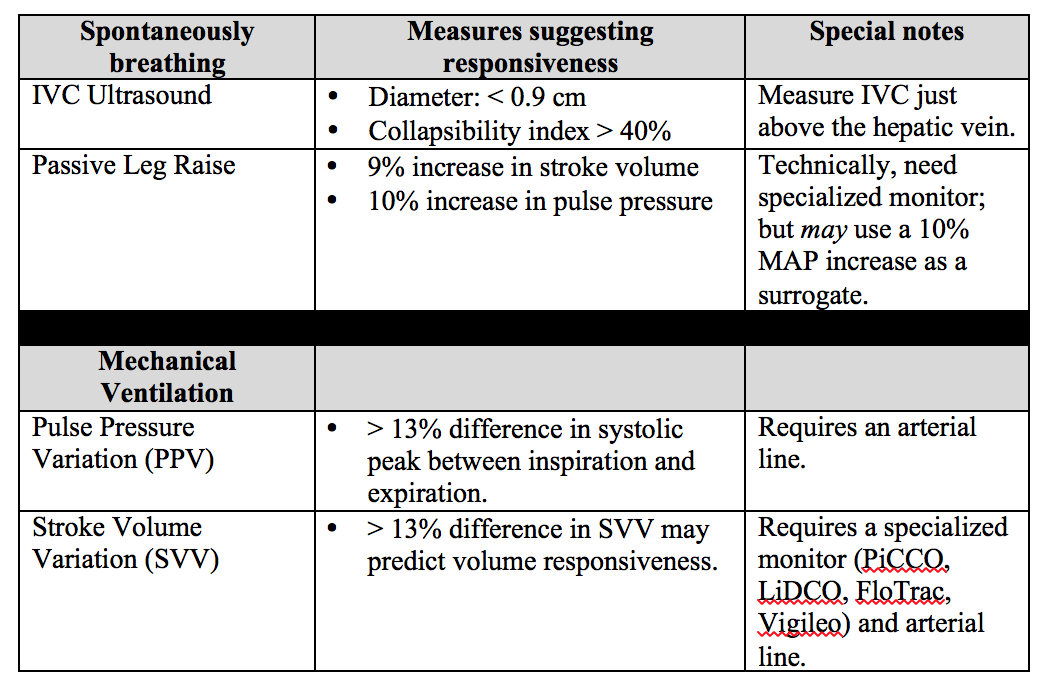
Important notes: PPV and SVV require the patient to be intubated with controlled tidal volumes. Arrhythmias and right heart failure make many of these measures invalid (except for PLR). Other methods of assessment not discussed include systolic pressure variation, left ventricular outflow track velocity time integral (LVOT VTI), and end-expiratory occlusion pressure (EEO).
Bottom Line: None of these measures are perfect and shouldn't be used in isolation to determine if the patient’s “tank is full”. Combine clinical judgment with these measures to get a best estimate of whether or not to give that next fluid bolus.
Reference
1. Enomoto TM, Harder L. Dynamic indices of preload. Crit Care Clin. 2010;26(2):307-21,
Follow Me on Twitter @JohnGreenwoodMD
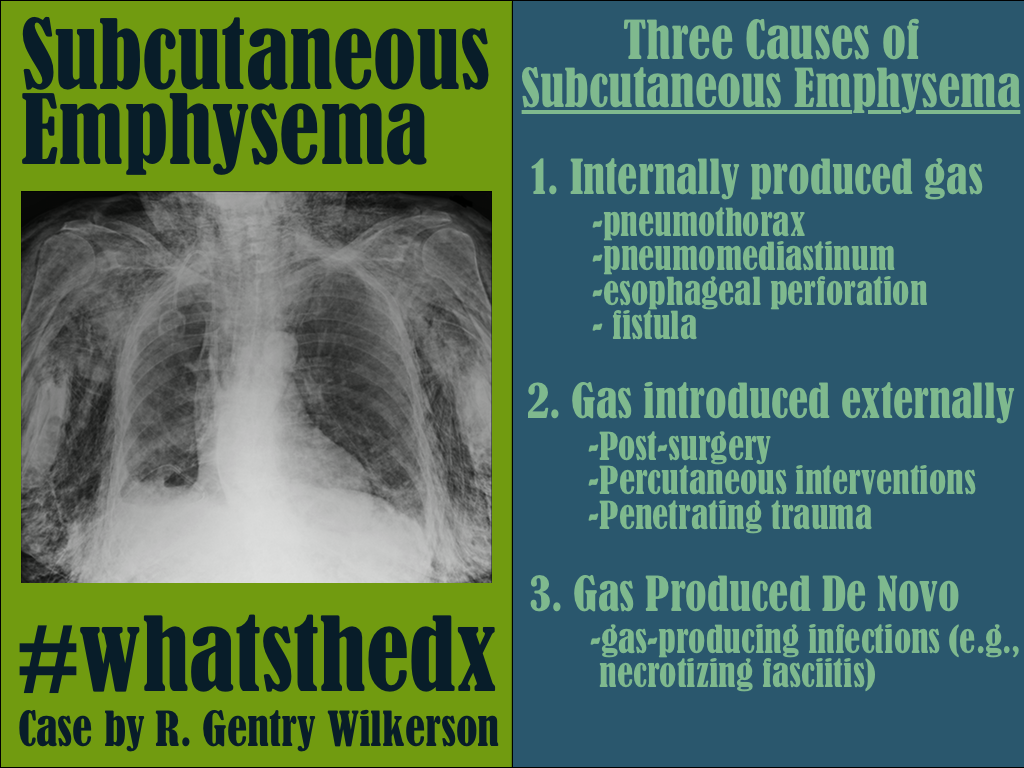
Patient presents with dyspnea. What's the diagnosis and name three potential causes (can be specific to the case or in general)?