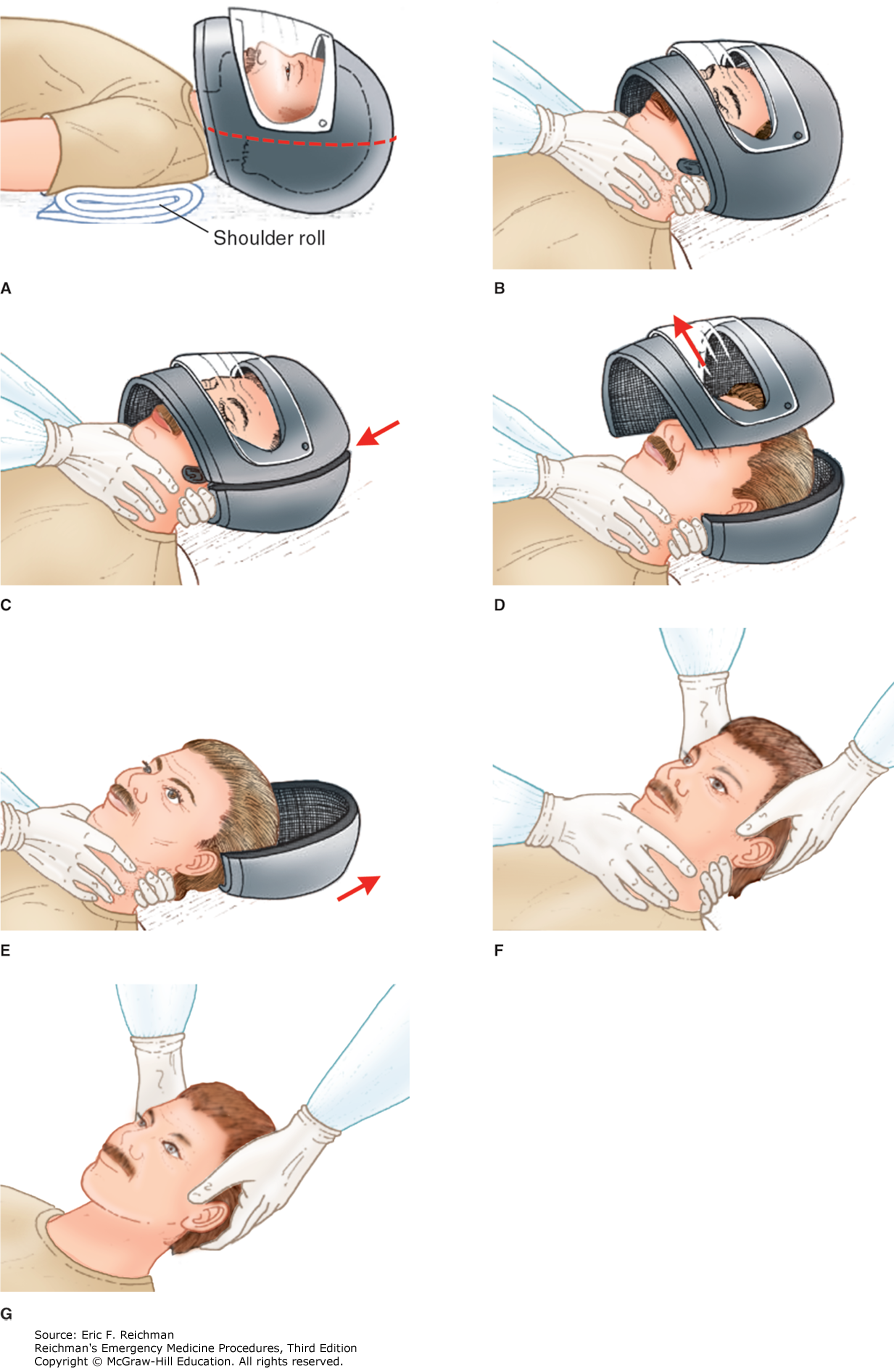
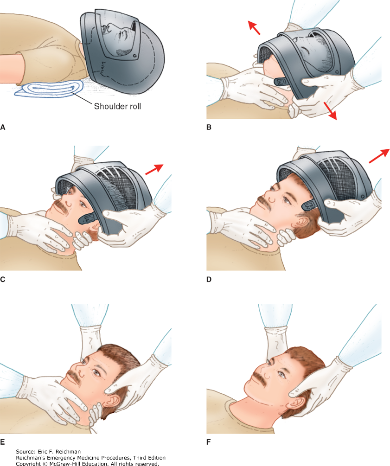
Here are two techniques to remove a helmet from an injured motorcyclist. The first uses a cast saw to bivalve the helmet. A link for a video is also provided.
US and International guidelines differ on the initial defibrillation dose in pediatric patients. International, European, Australian and New Zealand guidelines had recommend an initial dose of 4 J/kg for the initial and all subsequent doses while the American Heart Association recommends an initial dose of 2-4J/kg (with 2 J/kg in the teaching algorithms) with subsequent shocks being at least at 4J/kg and no greater than 10 J/kg. More recently, ILCOR suggested an initial dose of 2-4 J/kg.
This was a systemic review of 7 observational studies, mostly involving in hospital pediatric cardiac arrests. Outcomes of termination of VF/pVT, ROSC and survival to hospital discharged were examined in relation to the initial J/kg dose that was used compared to initial doses of 2 J/kg. Outcomes were neither better or worse with doses < 1.5 J/kg or > 2.5 J/kg. Additional research is needed as this certainty of this evidence was considered “very low.”
Access to reproductive care is being limited across the country, and the rate of undesired pregnancies is rising.
Discussing contraception preferences in the Emergency Department can support patients as well as and reduce the morbidity and mortality associated with an undesired pregnancy. Simply asking patients of childbearing age: "Are you interested in discussing pregnancy prevention?" can bridge a gap in access to reliable care. Easy and accessible tools can be used on shift to assist with appropriate initiation.
On Shift Tools:
Contraception Initiation • Clinical Resources • FemInEM
www.bedsider.org -Patient friendly comparisons of contraception options
Quick Start Contraception Care in the ED - Bridge to Treatment - ED oriented flow diagram
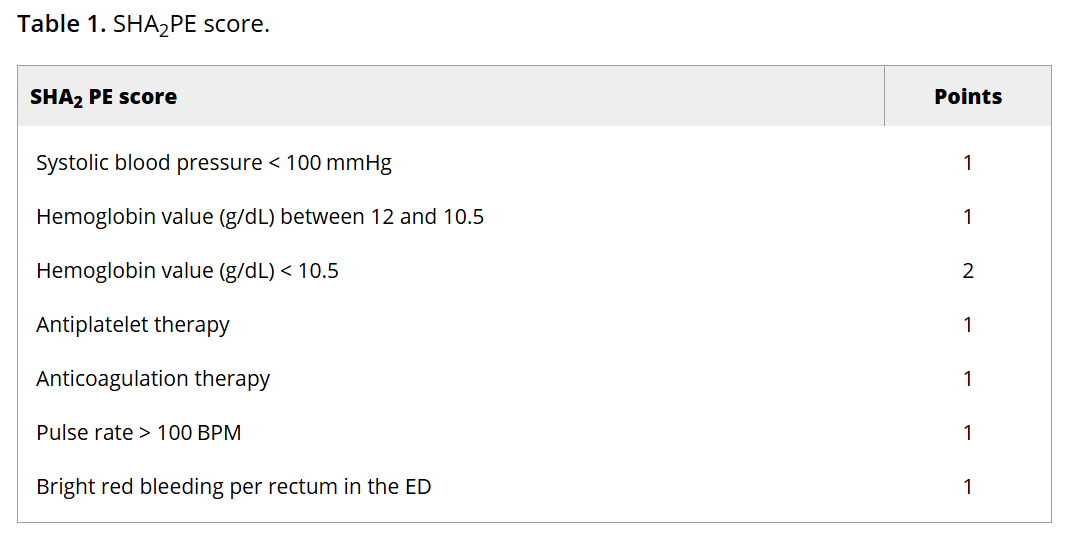
Lower GI bleed is a common reason for ED visits. This study aimed to validate a scoring system to identify low-risk LGIB pts who could be safely discharged from the ED.
The SHA2PE score incorporates characteristics and data that are commonly collected on patients with this complaint; readers can click through to see the scoring system. A score of less than or equal to 1 helps identify patients suitable for outpatient management, with a NPV of 98.3% (95% CI [97.2-99.1]) for predicting the need for hospitalization and acute intervention. However, the findings should be interpreted with caution given the relatively low prevalence of interventions within the study population.
Should we give a dose of antibiotics after intubating to reduce risk of VAP down the line? A multicenter RCT conducted in 2024 - the PROPHY-VAP Trial - found that a single dose of 2g ceftriaxone administered within 12 hours of intubation reduced VAP within the first week of hospitalization for patients intubated for airway protection due to TBI, stroke or SAH, with a VAP rate of 14% in the CTX group vs 32% in the VAP group (HR 0.60; 95% CI 0.38-0.95).
Click the link below for details and additional discussion
In 290 trauma patients diagnosed with dementia prior to injury, when compared to 3000 patients over age 65 without dementia and similar injury severity score, the dementia patients had a much higher rate of discharge to an institution instead of back to home living. This was particularly true of older women.
How much do you trust your plain film in the evaluation of elderly patients with traumatic hip pain?
BOTTOM LINE: It is critical to recognize and treat symptomatic hypocalcemia in pediatric patients.
Pediatric hypocalcemia has a variety of causes that should be considered. In the neonate congenital causes should be on the differential.
Parathyroid hormone levels should be checked on all patients along with magnesium levels and ionized calcium.
An ECG should also be obtained for prolonged QTc.
Management is guided by acute symptoms (tetany, seizures, cramping, etc.) or other signs of critical illness (sepsis, trauma, etc.) in conjunction with low ionized calcium levels.
For symptomatic patients give 20 mg/kg of elemental calcium IV over a 10–20 min period
For asymptomatic patient oral calcium supplements are typically given.
Failure to recognize concomitant hypomagnesemia may result in hypocalcemia that is resistant to treatment.
Disposition: Those children receiving IV calcium should be admitted with every 4-to-6-hour calcium levels and typically require ICU level admission. Children being monitored with oral supplementation can often be observed on a pediatric floor presuming there are no ECG abnormalities.
This article describes a paramedic run community health initiative to assist people with dementia transition to home after an ED visit. They describe:
“Persons living with dementia (PLWD) frequently use the emergency department (ED) for unscheduled care and experience significant challenges during the ED-to-home transition.
The Community Paramedic-led Transitions Intervention (CPTI) is a structured, coaching-based program delivered by community paramedics that includes a home visit and follow-up calls to support PLWD and care partners during the 30?days after ED discharge.”
Could your ED use a program like this to prevent readmissions?
Bottom Line: Multiple modalities of intervention may be needed to combat various aspects of salicylate toxicity. These include gastric decontamination, fluid hydration, dextrose admiinistration, aggressive serum alkalinization, establishment of normokalemia and hemodialysis. Intubation and chemical restraint should be avoided if possible.
A retrospective study looking at use of transdermal Buprenorphine in older trauma patients with rib fractures found a good safety profile (less naloxone use) and less overall opioid use however no change in overall length of stay or mortality. Adding this to your multimodal pain strategy in older patients with rib fractures seems like a reasonable plan.
A narrative review of literature involving older patients and constipation found:
“Major contributing factors include physical inactivity, sarcopenia, dehydration, inappropriate defecation posture, and polypharmacy, particularly opioids and anticholinergic agents. Importantly, these factors interact through the brain–gut–microbiota axis, contributing not only to gastrointestinal dysfunction but also to systemic outcomes such as frailty, cognitive decline, and increased healthcare burden, thereby supporting a multidimensional disease framework.”
It isn’t as simple as adding a laxative.
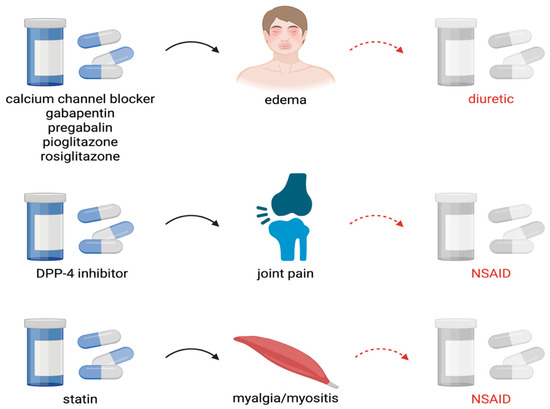
The article outlines how instead of looking at medications as the cause of symptoms, we often add more medications to treat the medication induced symptoms. Here is an example of how we get to polypharmacy in older patients
Body armor/ bullet resistant vests used by law enforcement are designed to stop penetration by handgun rounds. These rounds have less velocity than rifle rounds. When caring for someone who has been shot while wearing body armor, verify no penetration has occurred and then look for blunt injuries such as rib fractures, liver injuries, pneumothorax, cardiac contusion, vertebral injury, etc. Behind Armor Blunt Trauma (BABT) is the technical term for injuries caused by the transfer of kinetic energy that occurs when these vests are struck.
This narrative review of the trauma literature looking at chronic pain after trauma found:
Ambient Artificial Intelligence based scribes that create visit notes based on the conversation in the room during patient evaluation may save documentation time and reduce total time in the health record but may not perform as well as human scribes in some circumstances, at least for pediatric patient charts.
PaO2 to FiO2 (P:F) ratios, are often considered the gold standard in critical care for assessing the degree of oxygen-refractory hypoxia in various pathologies, particularly ARDS. P:F does have some limitations, including not accounting for the PEEP, but probably the most limiting is that it requires collecting an ABG, which is invasive and not always feasible or a top priority when resuscitating a critically ill hypoxic patient. On the other hand, SpO2 (pulse ox saturation) is routinely available, and of course the FiO2 should be known, so many have suggested perhaps using an SpO2 to FiO2 (S:F) ratio instead. But how S:F maps to P:F and how well they correlate is not fully known. Chaudhuri et al recently conducted a meta-analysis, published in Critical Care Medicine this month, which reviewed the literature on this.
Bottom Line: Yes, S:F ratios correlate well with P:F ratios, especially when the SpO2 is less than 97%, but you can't just substitute the S:F for P:F, you have to use one of the accepted formulas. See additional info on the website for the actual formula to apply and how a given S:F translates to P:F.
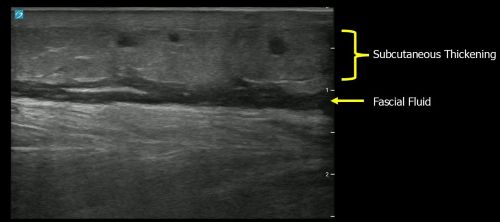
Sonographic findings suggestive of necrotizing fasciitis include:
Remember the mnemonic: STAFF (subcutaneous thickening, air, and fascial fluid)
Bottom line: Routine screening for atrial fibrillation (AF) is not recommended in the emergency department (ED). However, AF is often detected incidentally on continuous ECG monitoring. When identified, clinicians should inform the patient and consider anticoagulation if indicated.
This German retrospective review of 1500 level one trauma center patients (ICU level or ISS over 9) found obesity was an independent predictor of ARDS, multisystem organ failure, and sepsis but not pneumonia or mortality.