It is a common scenario in the ICU, and occasionally in the ED, to be asked which pressor you would like to wean first, norepinephrine or vasopressin. This is mostly an “art not science” question, but is there a right answer? Does picking one vs the other to wean first lead to less hypotension?
Bottom Line: This meta-analysis doesn't suggest that either the norepi-first or vasopressin-first strategies for vasopressor wean are associated with an increased incidence of hypotension, although the literature is mixed. Whatever your current practice is, it's probably reasonable to stick with that. See the additional information for my personal approach.
Key Takeaway: Most emergency department prescription callbacks for clarification are preventable. The most frequently identified causes include unclear directions for use, incorrect medication or dose, allergy or adverse reaction concerns, and duplicate prescriptions. A quick double-check before you hit “send” can save you (and the pharmacist) a callback later.
Cerebral venous sinus thrombosis (CVST) is an emergent diagnosis frequently missed on standard brain imaging in the ED, with studies reporting miss rates up to 30–73% on noncontrast CT alone. Diagnostic delays average 4–10 days from initial presentation in confirmed cases. CTV and MRV both have very high sensitivity for detection of CVST.
When to Suspect CVST
Summary: Consider adding CTV in patients with strong thrombotic risk factors, atypical/multifocal hemorrhage patterns, or focal deficits unexplained by CT/CTA.
Bottom line: Good news! In 2022 and 2023, at ACEP, SAEM and AAEM, invited speakers were evenly split 50/50 women and men (with a small percentage nonbinary) showing no significant gender bias toward speaker invitation.
Bottom line: Socioeconomic differences in outcomes of cardiac arrest are present in the pediatric population as well and CPR education and resources should be present in ALL communities.
In a single level 1 trauma center there were 274 patients age over 55 evaluated for falls in a one year retrospective period. Their blood toxicology was reviewed for presence of alcohol, opioids, benzodiazepines and cannabinoids. The authors found:
“detection rates were 21.2% for opioids, 18.6% for ethanol, 13.9% for benzodiazepines, and 9.1% for cannabinoids. Injuries identified included 16.4% spinal fractures, 9.5% extremity fractures, 7.7% hip/thigh/pelvic fractures…In this study, nearly 20% of adults 55+ presenting for fall-related trauma recently used substances that impair psychomotor function.”
An area for injury prevention research and intervention would be to screen patients over age 55 for substance use, consider prescribing patterns in this age group (benzodiazepines) , and discuss with patients fall risk avoidance.
Bottom line: Education to the public is needed to help to improve the information relayed to telecommunicators in an emergency. Further telecommunicator education can help to overcome the barriers within their control, such as the recognition of agonal breathing.
Bottom Line: Hypertonic sodium bicarbonate (8.4%) can be used judiciously as an alternative hyperosmolar therapy in the setting of increased intracranial pressure (ICP) or cerebral edema with impending herniation, particularly in setting of concomitant metabolic acidosis. Two 50 mL ampules of hypertonic sodium bicarbonate is the equivalent of approximately 200 mL of 3% sodium chloride (hypertonic saline).
Bottom Line: Left Optic Disc Elevation was found to be an independent predictor of mortality and need for surgical intervention for patients with head trauma.
A case report on use of the abdominal aortic and junctional tourniquet in a 27 year old female with hemorrhagic shock secondary to a pelvic fracture after a 10 meter fall demonstrated improved blood pressure and stabilized vasopressor use prior to operative intervention. This device has been used in battlefield situations, however very few reports of civilian use exist. Much more data is needed, however, it is a device to be aware of for future use.
BOTTOM LINE: Modify WBC threshold for diagnosing septic arthritis is patients who received recent antibiotics (24h to 2 weeks).
BOTTOM LINE: It is generally safe and effective to discharge vomiting pediatric patients with a prescription for ondansetron, and a recent study supported this common practice.
While it has become common practice to prescribe ondansetron to children with emesis, a 2025 randomized controlled study showed that a prescription for ondansetron decreased the risk of moderate to severe gastroenteritis in the following 7 days.
This study compared children 6 months to 18 years of age who received either ondansetron or placebo. They found a rates of moderate to severe gastroenteritis to be 5.1% in the ondansetron group versus 12.5% in the placebo group.
*Note that ondansetron is NOT approved for children under 6 months of age or in those with prolonged QT.
Take Home Point: Andexxa (andexanet alfa) was voluntarily withdrawn from the US market effective December 22, 2025, due to safety concerns. 4-Factor Prothrombin Complex Concentrate (4F-PCC/Kcentra) remains the standard of care for reversing apixaban and rivaroxaban in life-threatening bleeding.
Why was it pulled? AstraZeneca, in consultation with the FDA, discontinued the manufacturing and sale of Andexxa after the ANNEXA-I post-marketing trial showed that the drug's risks outweigh its benefits. The trial compared Andexxa to usual care (primarily 4F-PCC) in intracranial hemorrhage and found a significant safety signal:
Clinical Action Items:
------------------------------------------------------------------------------------------------------------
Institutional Note: You may recall that our institution (like many others) never added Andexxa to the formulary. We cited the lack of high-quality survival data and cost-benefit concerns as our primary reasoning. Consequently, this market withdrawal requires no change to our local practice. We will continue to use 4F-PCC as our standard for Factor Xa inhibitor reversal, a practice now validated by the FDA's safety findings.
Diagnostic Errors in the Critically Ill
Well, it depends on who you ask - ACOG defines it as greater or equal to 1000ml of blood loss within that first 24 hours, but most research articles define it as greater or equal to 500ml, while they define severe postpartum hemorrhage as greater or equal to 1000ml. But what is it actually?
The World Health Organization decided to tackle this question to look at what level of blood loss is the most clinically relevant in a meta-analysis from last year. They reviewed 12 different databases and over 300000 patients to look at levels of blood loss and when that was associated with mortality/severe morbidity. They found that the standard 500ml cutoff was actually only around 75% sensitive, but when they dropped those levels to 300/400/450, they lost a lot of specificity. So, what they did is they came up with their own rules and re-evaluated them based on their data to see how sensitive and specific they were.
What they found with a sensitivity of 87% and a specificity of 66-76% was:
Consider someone as having CLINICALLY SIGNIFICANT blood loss if they had EITHER:
OR
So look at the vitals + the blood loss together, and use those to guide your clinical actions!
Popliteal artery injuries are very rare (4% of all vascular injuries).
The majority of injuries are secondary to penetrating injury (70+%)
Blunt mechanism of injury has the higher rate of amputation.
Prolonged ischemia time (from injury to repair greater than 6 hours) leads to higher rates of amputation
Hard signs of vascular injury should prompt X-ray imaging of the knee, femur, and lower extremity and transfer to an operating room for repair.
Soft signs ("a history of significant bleeding which has ceased, nonexpanding hematomas, and the presence of an Ankle-Brachial Index of less than 0.9") and shotgun injury should prompt CT angiogram to evaluate arterial injury.
In a metanalysis of studies looking at intercranial hemorrhage in fall patients older than 65 years, the following were unadjusted odds ratio risk factors for finding an ICH in this patient population:
suspected open or depressed skull fracture , signs of basal skull fracture ), reduced baseline Glasgow Coma Scale score , focal neurologic signs , seizure , vomiting , amnesia , loss of consciousness , headache ), external sign of head trauma , male sex , chronic kidney disease , preinjury single antiplatelet , and dual antiplatelet medication .
Preinjury anticoagulant was not a significant risk factor.
When looking at adjusted odds rations only focal neurologic signs , external sign of head trauma , loss of consciousness , and male sex were found to be associated with intercranial hemorrhage.
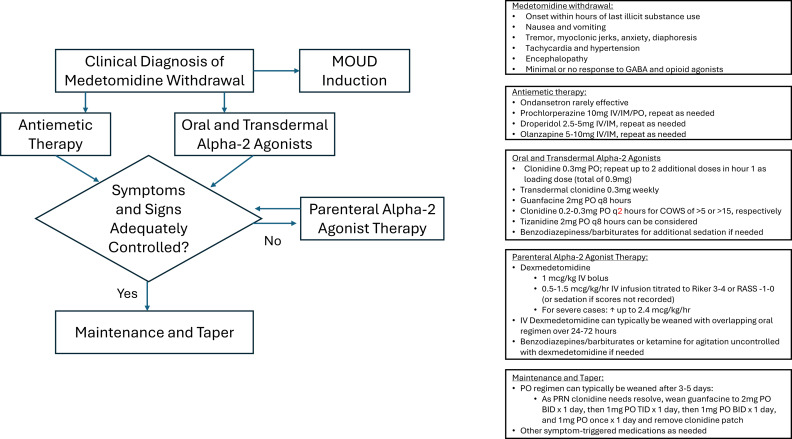
The US drug supply has been found to contain medetomidine as an adulterant to heroine/fentanyl. It is a potent tranquilizer used in animals. It is an alpha 2 blocker (similar pharmacology to clonidine and xylazine). Exposure to this drug can induce withdrawal symptoms to include anxiety, tremor, diaphoresis, nausea, vomiting, agitation, sympathetic hyperactivity, and delirium. Withdrawal can start within 4-6 hours of last use.
Treatment for withdrawal is outlined in this diagram.

Etomidate is often a go-to agent for RSI because it is considered relatively hemodynamically neutral. However, lab studies have shown an association with transient adrenal suppression, and some observational studies and meta-analyses have suggested that patients intubated with etomidate face higher risk of cardiovascular collapse and in-hospital mortality than those intubated with ketamine.
The RSI trial was a pragmatic open-label multi-center randomized control trial conducted in 6 EDs and 8 ICUs across the US and compared induction with ketamine 1-2mg/kg versus etomidate 0.2-0.3mg/kg for RSI of critically ill adults (excluding trauma patients). They found no significant difference in overall 28 day hospital mortality across the cohort. They found an increased risk of cardiovascular collapse during intubation in the ketamine group. This increased risk was more pronounced in patients with sepsis or septic shock and patients with APACHE II ?20.
Some details:
Overall - this was a well conducted randomized control trial that - at the very least - suggests that etomidate is likely as safe (if not safer) than ketamine with respect to 28d mortality and peri-intubation cardiovascular collapse, even among patients with critical illness or septic shock.
