Is there a set of criteria similar to the Ottawa Ankle or Knee Rule that can be applied to the wrist in children?
The Amsterdam Pediatric Wrist Rules are as follows:
-Swelling of distal radius
-Visible deformity
-Painful palpation of the distal radius
-Painful palpation at the anatomical snuff box
-Painful supination
A positive answer to any of these would indicate the need for an xray.
The study referenced attempted to validate these criteria. This criteria is inclusive of the distal radius in addition to the wrist. The sensitivity and specificity were 95.9% and 37.3%, respectively in children 3 years through 18 years. This model would have resulted in a 22% absolute reduction in xrays. In a validation study, 7/170 fractures (4.1%, 95% CI: 1.7- 8.3%) would have been missed using the decision model. The fractures that were missed were all in boys ages 10-15 and were all buckle fractures and one non displaced radial fracture.
Bottom line: This rule can serve as a guide for when to obtain an xray in the setting of trauma, but it is not perfect.
Monosodium glutamate
Metabisulfites (Na sulfite, Na/K bisfulfite, Na/K metabisulfite, etc.)
Tyramine reaction
Niacin
Trichloroethylene
Scrombroids
Hydroxocobalamin
Which infectious disease listed as Class A agents occur naturally, though sporadically within the U.S?
Small pox no longer occurs naturally and other viral hemorrhagic fevers occur in tropical settings.
SIMV (Synchronized intermittent mandatory ventilation)
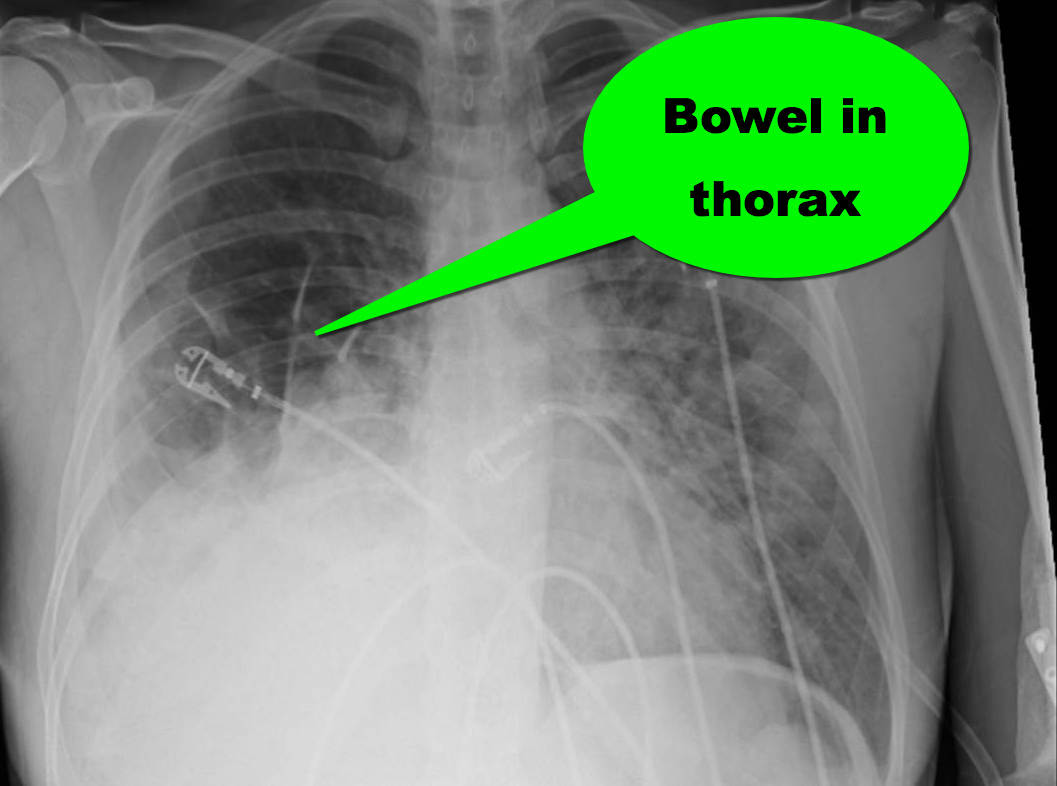
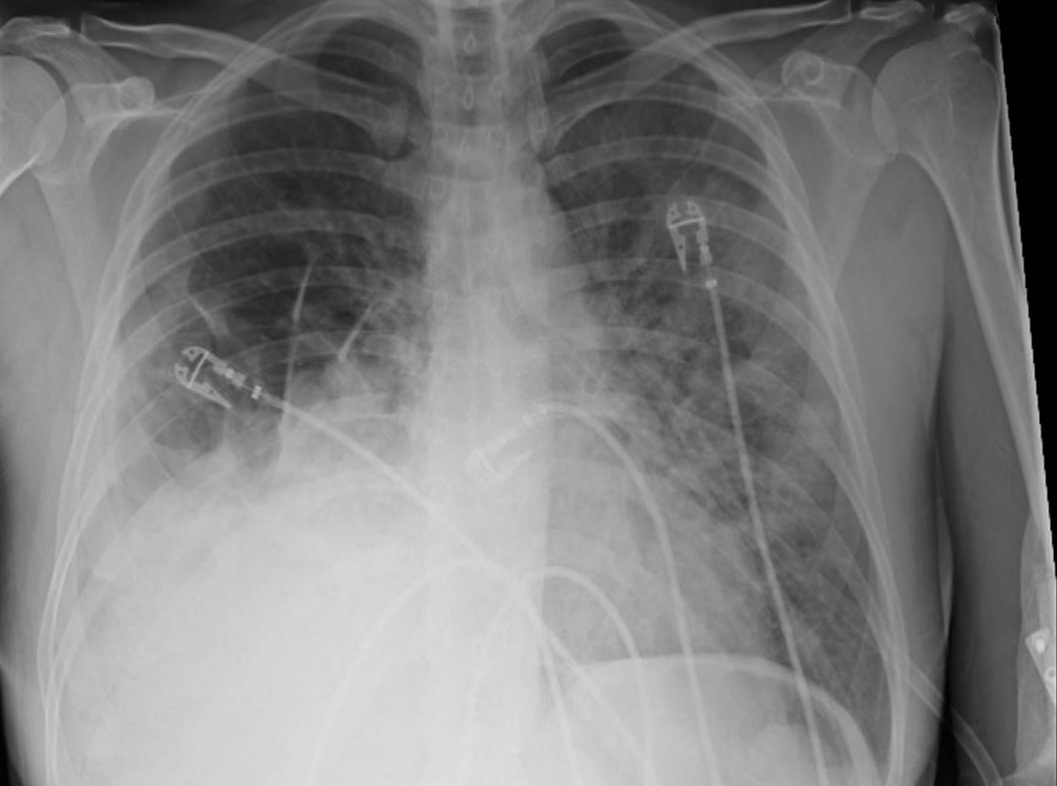
35 year-old female presents to the Emergency Room with cough and chest tightness. She was discharged from the hospital yesterday for an asthma exacerbation that was secondary to pneumonia. What's the diagnosis?
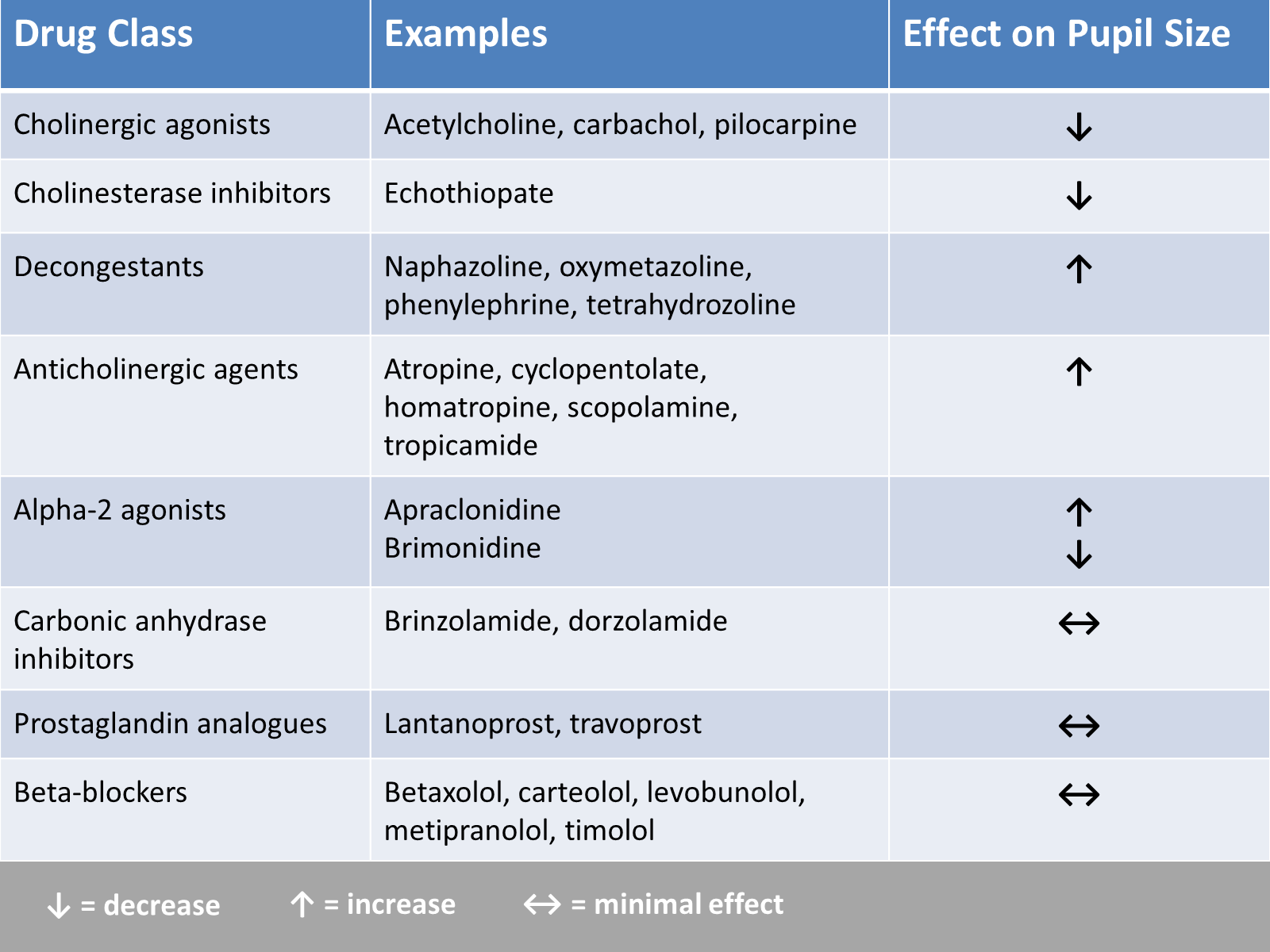
In the evaluation of ED patients, it may be important to understand the effect on pupil size from the ophthalmic medications they use. Here is a summary chart of common eye drops and their effect on pupil size.
Serotonin Syndrome - What is It?
** Stay tuned for part 2 on what causes serotonin syndrome **
Hyperoxia in the Critically Ill
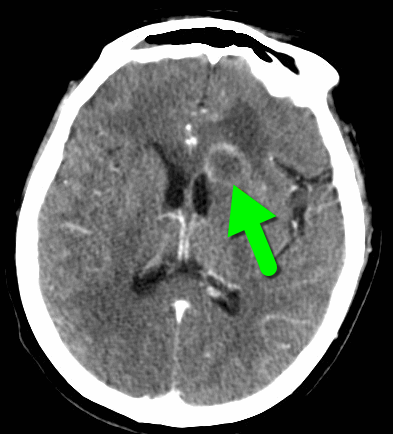
68 year-old man presents with a new-onset seizure. What's the diagnosis and what's in your differential diagnosis?
A new prospective, randomized, double-blind trial compared subdissociative ketamine to morphine for acute pain in the ED.
What they did
What they found
Injuries are a leading cause of morbidity and mortality globally
Injuries are the leading cause of preventable death in travelers
Bottom Line: Stay safe while travelling. The same safety habits used in the US, such as wearing your seatbelt or not drinking and driving, are important patterns while traveling.
Your ESLD patient is hypotensive with a tense abdomen, and he needs a paracentesis!
--ALWAYS use ultrasound to localize a fluid pocket [Fig 1]! Take the time to use color Doppler to look for underlying abdominal wall varices [Fig 2]. Cirrhotic patients frequently have abnormal abdominal wall vasculature [1-2].
--Hemorrhage from paracentesis is exceedingly rare, and reversal of mild coagulopathy probably isn't that important [3-4].
--In hypotensive patients, consider placement of a small pigtail catheter for slow, continuous drainage (e.g. 8.3F pericardiocentesis catheter) instead of large-volume paracentesis. Non-tunneled catheter infection risk goes up after 72h [5].
--Albumin replacement improves mortality and incidence of renal failure in patients with SBP or other infection [6-7].
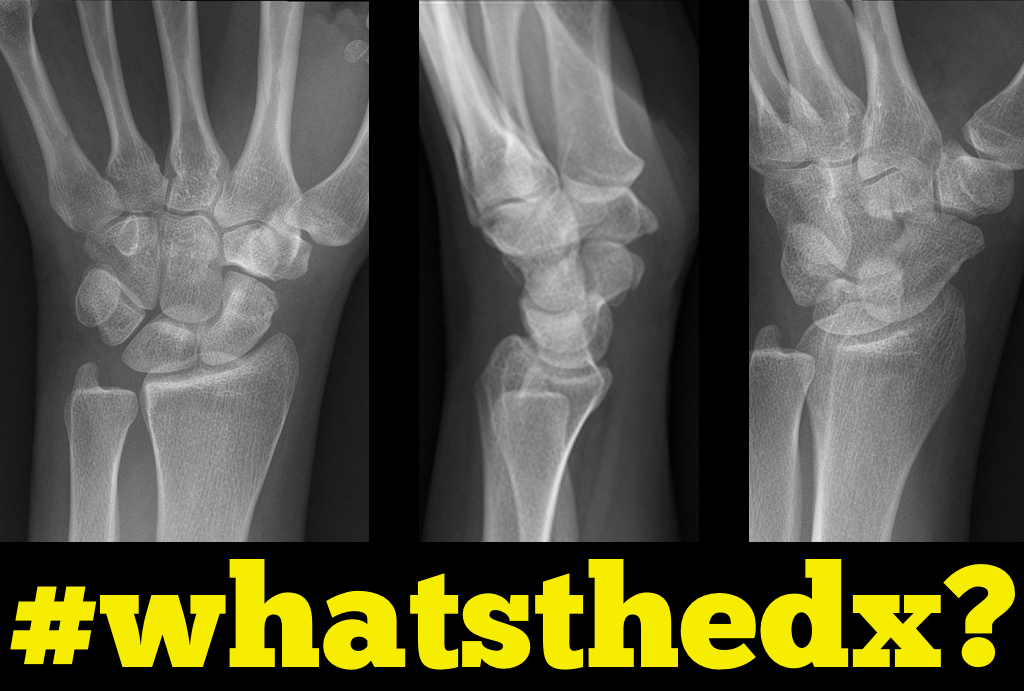
Person presents following a fall on an outstretched hand and there is snuffbox tenderness. What's the diagnosis?

Policeman's Heel:
When patient's present complaining of heel pain we often think immediately of plantar fascititis,and heel spurs. If they jumped and landed on the heel with are concerned for calcaneal fracture. However, a policeman's heel can occur from repetitive bounding of the heel or from landing on it as in a fall or jump.
Policeman's heel has been descirbed as a plantar calcaneal bursitis, inflammation of the sack of fluid (bursa) under the heel bone, or a contusion of the heel bone due to flattening and displacement of the heel fat pad, which leaves a thinner protective layer allowing the bone to get bruised.
Regardless of cause this responds well to NSAIDs, limiting weight bearing, or taping the foot. If the repetitive activity is not reduced this can easily become a chronic cause of heel pain. A short video showing how to tape the foot can be found at https://youtu.be/nQtkwfJrhXo
Making the wee patient pee – a non invasive urinary collection technique in the newborn
Obtaining a urinary sample in a neonate can be challenging and time consuming. The most commonly used non-invasive technique is urine collection using a sterile bag. This technique is limited by patient discomfort and contamination of the urinary sample. Catheterisation and needle aspiration are other options, but are more invasive.
A prospective feasibility and safety study enrolled 90 admitted infants aged under 30 days who needed a urine sample into the study [1]. They performed the following stimulation technique.
1. Feed the baby through breast-feeding or an appropriate amount of formula for their age and weight.
2. Wait twenty-five minutes. After twenty-five minutes clean the infant’s genitals thoroughly with warm water and soap. Dry with sterile gauze.
3. Have an assistant hold a sterile urine container near the infant
4. Hold the baby under their armpits with their legs dangling (if short handed, parents can do this)
5. Gently tap the suprapubic area at a frequency of 100 taps or blows per minute for 30 seconds
6. Massage the lumbar paravertebral zone lightly for 30 seconds
7. Repeat both techniques until micturition starts. Collect midstream urine in the sterile container
In the study, success was defined as obtaining a midstream urinary sample within 5 minutes after initiation of the stimulation procedure. There was a 86% success rate (n=69/80). Mean time to sample collection was 57 seconds. There were no complications, but controlled crying occurred in 100% of infants. The study was limited by the lack of a control group. Previous studies have described longer collection times with traditional non invasive techniques, up to over an hour [2].
Conclusion
Consider the above mentioned stimulation technique to obtain a urinary sample in the neonate.
Status migrainosus is a migraine that lasts more than 72 hours, and can be rather challenging to control. A few tips to tackle this are:
1. Adequately hydrate all patients (IV fluids are usually required, especially with severe nausea/vomiting)
2. Establish realistic expectations for the patient. A patient with chronic daily headaches will not be pain-free in the ED.
3. Use IV nonopioid medications for pain control
1st Line:
- Dopamine Antagonists: in increasing efficacy
- Metoclopramide
- Phenothiazines: prochlorperazine, promethazine and chlorpromazine
- Butyrophenones: droperidol and haloperidol
- NSAIDs: such as Ketorolac IV or IM
2nd Line:
- Corticosteroids: Do not treat the migraine in the ED, but prevent headache recurrence within 72 hours.
- Magnesium Sulfate: Has shown mixed efficacy. More likely to have a sustained benefit in patient with serum magnesium level of 1.3mg/dL or less.
- Valrpoic Acid: Be careful of combining it with Topiramate.
- Vasoconstrictors: Triptans, ergotamine, dihydroergotamine. Effective, but use is limited by contraindications.
- Opioids: Last resort
The RV is a low-pressure chamber that doesn’t tolerate acute increases in pulmonary pressures (e.g., ARDS, pulmonary embolism, etc.); acute increases can lead to RV dysfunction / failure
Managing RV dysfunction requires a three-pronged approach:
You find this interesting view while scanning a patient. Which view is this and why should you care about it?
Sodium Supplementation and Exercise-Associated Hyponatremia (EAH) during Prolonged Exercise (ultramarathon running)
Weight loss of around 4% body weight (relative to pre race weight) can be anticipated to maintain euhydration in such a prolonged event
Those who become symptomatic with EAH have either gained weight or lost less that 3-4% body weight
Overhydration rather than inadequate supplemental sodium intake is a greater contributor to the development of EAH
There is a suggested link between EAH and rhabdomyolysis. The mechanism remains unknown and it is unclear which condition may augment the other. Further research is needed.
Take home: Avoid overhydration during prolonged exercise to prevent EAH.
The answer may be no, as long as you have a serum HCO3. In this retrospective study, linear regression was used to to assess serum HCO3 as a predictor of venous pH. Logistic regression was also used to evaluate serum HCO3 as a predictor of DKA. Using a HCO3 cutoff of <18 mmol/L had a sensitivity of 91.8% and specificity of 91.7% for detecting a pH <7.3. A HCO3 < 8 had a sensitivity of 95.2 % and specificity of 96.7 % for detecting a pH <7.1.