Emergency medicine remains a relatively young and developing specialty in most parts of the world. However, it is growing in popularity, especially in the U.S. How competitive is it currently?
For the recent 2016 Match, there were 2476 applicants for 1895 categorical emergency medicine positions from 174 programs.
Bottom Line: Emergency medicine remains a highly desired and competitive specialty in the U.S.
Congratulations to all the incoming interns for the 2016-2017 year!
What is cardio-renal syndrome CRS?
There are 5 types
1. Acute CRS: abrupt worsening of heart function leading to kidney injury
2. Chronic CRS: chronic heart failure leads to progressive kidney disease
3. Acute renocardiac syndrome: abrupt kidney dysfunction leading to acute cardiac disorder
4. Chronic renocardiac syndrome: chronic kidney disease leading to decreased cardiac function
5. Systemic CRS: Systemic condition leading to both heart and kidney disease
Metacarpal Fractures
* Localize fracture to head, neck or shaft (neck most common)
5th metacarpal most commonly fractured
* Note amount of angulation, shortening and the presence of malrotation
*Treatment is based on which metacarpal is fractured and the location of the fracture
*The amount of acceptable angulation varies by the digit involved
For example for index and long finger - acceptable angulation of the shaft is 10-20 degrees and neck is 10 to 15 degrees
Whereas for the 5th digit - acceptable angulation for the shaft is 40 degrees and neck is 50 degrees
Pearls
No degree of malrotation is acceptable (document the absence of this!)
Strongly suspect fight bite injury with abrasions/lacerations overlying metacarpal heads
Highly prone to infection given the proximity to the joint capsule
Consider lacerations over metacarpal fractures as open fractures (do not close/discuss management with hand surgery re timing of washout. Many prefer delayed fixation for suspected infections )
Document integrity of the extensor tendon (can be lacerated and retracted)
Cerebral Venous Thrombosis
A meta-analysis of 74 randomized trials with a total of 58,556 patients was recently published in the Lancet that looked at the effectiveness of NSAIDs in the treatment of osteoarthritis (OA) pain.
Briefly, their conclusion was that:
You can find the article here http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2816%2930002-2/abstract
A previous pearl has looked at serum HCO3 as a predictor of DKA (see pearl from 8/21/15). The article by Gilhotra looks at using end tidal CO2 (ETCO2) to exclude DKA. 58 pediatric patients were enrolled with 15 being in DKA. No patient with ETCO2 > 30 mmHg had DKA. Six patients with ETCO2 < 30 mmHg did not have DKA. Other studies done in children have shown similar results.
An article recently published by Chebl and colleagues examined patients older than 17 years with hyperglycemia. In this study, 71 patients were included with 32 having DKA. A ETCO2 >35 excluded DKA in this group while a level <22 was 100% specific for DKA.
Bottom line: ETCO2 >35 mmHg is a quick bedside test that can aid in the evaluation of hyperglycemic patients.
Cutaneous larva migrans (CLM) is an acquired dermatosis
Clinical manifestations:
Treatment:
Bottom Line:
There are multiple vasoactive infusions available for acute hypertensive emergencies, many having serious side effect profiles or therapeutic disadvantages.
Clevidipine (Cleviprex) is rapidly-titratable, lipid-soluable dihydropyridine calcium channel blocker which has become increasingly used in the ICU in recent years [1]:
ECLIPSE trial compares clevidipine, nicardipine, nitroglycerin and nitroprusside in cardiac surgery patients. .
Clevidipine was as effective as nicardipine at maintaining a pre-specified BP range, but superior when that BP range was narrowed (also studied in ESCAPE-1 and ESCAPE2 with similar results) [2-3]
TAKE-HOME: Clevidipine is an ultra short-acting, rapidly-titratable vasoactive with favorable cost, pharmacokinetics, and side-effect profile. Consider its use in hypertensive emergencies.
Femoral neck fracture
We typically think of the presentation of the displaced fracture severe pain, writhing in the bed, unable to ambulate, limited ROM
* However, patients with nondisplaced fractures (15 20%) may walk with a limp
* Occurs primarily in the elderly & osteoporotic population after a fall directly onto the hip
* Look for a cortical step-off in the femoral neck (w/ foreshortening)
* A patient with a minimally displaced fracture may only complain of hip, knee, or groin pain and may be able to walk (albeit with a limp)
* Almost 9% of hip fractures are radiographically normal (Nondisplaced or impacted fractures)
* Fractures which were initially nondisplaced, may become displaced upon re-presentation
* Remember the limitations of plain x-ray in the evaluation of femoral neck fractures!
* Because of the significant complication of overlooking a femoral neck fracture, MRI has become the recommended imaging modality of choice for a patient with a high suspicion for a femoral neck fracture, despite normal plain radiographs of the hip
Acute cocaine toxicity can manifest with several cardiovascular issues such as tachycardia, dysrhythmia, hypertension, and coronary vasospasm. A new systematic review collated all of the available evidence for potential treatment options. Here is what the review found (there is also an 'other agents' section for medications with less published reports):
Benzodiazepines and other GABA-active agents: Benzodiazepines may not always effectively mitigate tachycardia, hypertension, and vasospasm from cocaine toxicity.
Calcium channel blockers: Calcium channel blockers may decrease hypertension and coronary vasospasm, but not necessarily tachycardia.
Nitric oxide-mediated vasodilators: Nitroglycerin may lead to severe hypotension and reflex tachycardia.
Alpha-adrenoceptor blocking drugs: Alpha-1 blockers may improve hypertension and vasospasm, but not tachycardia, although evidence is limited.
Alpha-2-adrenoceptor agonists: There were two high-quality studies and one case report detailing the successful use of dexmedetomidine.
Beta-blockers and alpha/beta-blockers: No adverse events were reported for use of combined alpha/beta-blockers such as labetalol and carvedilol, which were effective in attenuating both hypertension and tachycardia.
Antipsychotics: Antipsychotics may improve agitation and psychosis, but with inconsistent reduction in tachycardia and hypertension and risk of extrapyramidal adverse effects.
Sodium bicarbonate: Twelve case reports documented treatment of dysrhythmia with IV sodium bicarbonate, with seven reporting successful termination.
The authors note that "publication bias is a concern, and it is possible that successful treatment and/or adverse events have not been reported in some of the publications, and in general."
Sunset Eye Sign
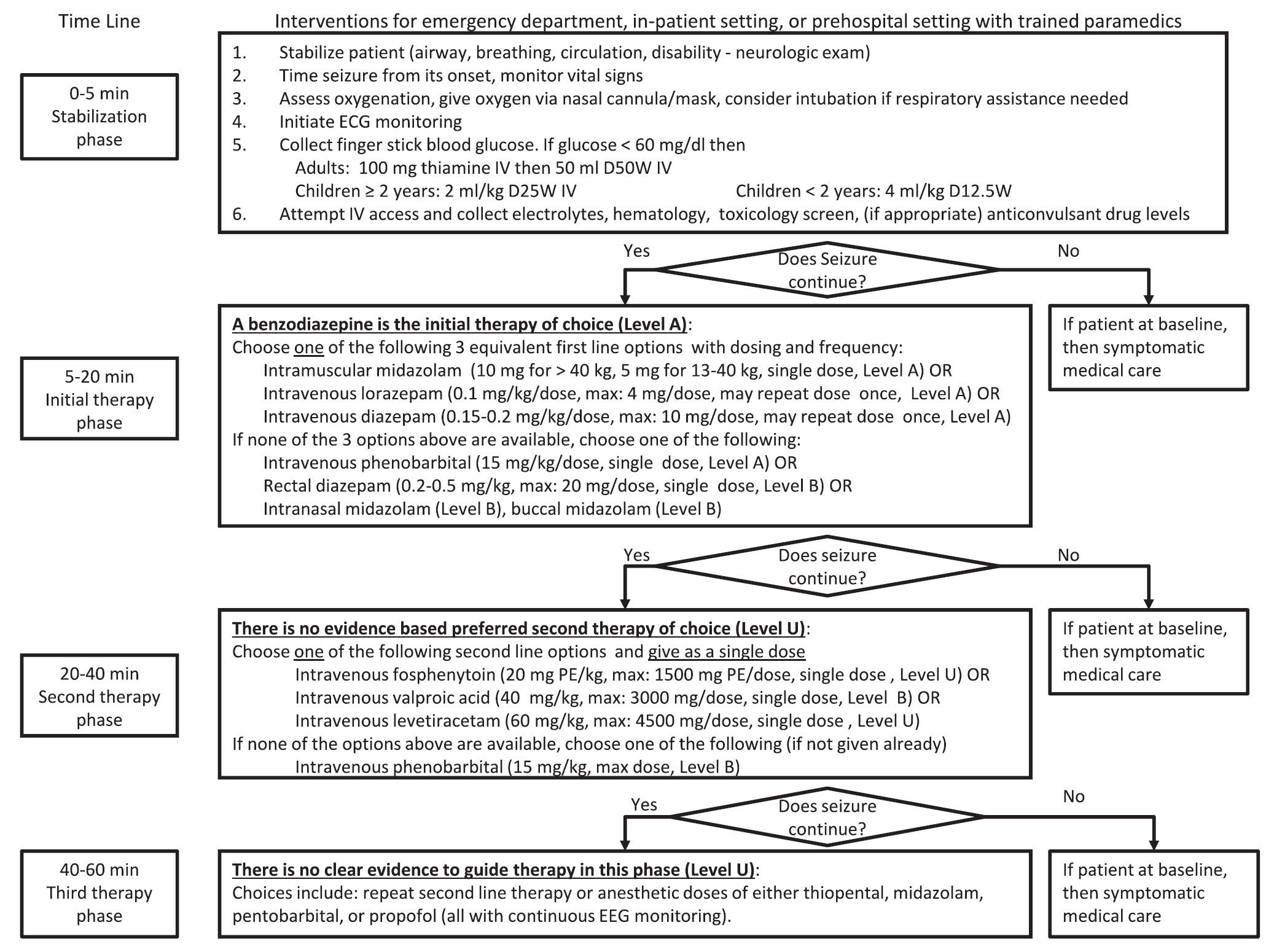
A new guideline for convulsive status epilepticus in adults AND children was recently published. [1] An insightful commentary was published alongside it (both are open access). [2] The proposed algorithm is below. Here are a few additional points to note:
Pure opioid agonists such as Morphine, Hydromorphone, and Fentanyl stimulate opioid receptors and are the most potent analgesics. Fentanyl and fentanyl analogues are up to 100 times more powerful than morphine and 30-50 times more powerful than heroin.
W-18 is a highly potent opioid agonist with a distinctive chemical structure which is not closely related to older established families of opioid drugs. While Fentanyl is approximately 100 times more powerful than Morphine, W-18 is about 100 times more powerful than Fentanyl.
While the flu season this year has been mild, it is still important to recognize which patients are at high risk for flu-related complications:
During the influenza season, when admitting a patient who 1) has respiratory symptoms and 2) is at high risk for influenza complications, consider testing them for influenza.
19 year-old male complaining of left arm pain one week after injecting anabolic steroids into his shoulder. What's the diagnosis?
Achilles tendon rupture
More common in
men, ages 30 - 40yo, s/p steroid injections, fluoroquinolone use, and episodic athletes "weekend warriors
Mechanism: usually during an athletic endeavor, sudden forced planar flexion or violent dorsiflexion of a plantar flexed foot
Location: Usually occurs 4 to 6 cm ABOVE the Achilles calcaneal insertion (hypovascular region)
Patient will report a sudden pop, gunshot like sound
History: Will report heel and calf pain and weakness/inability to walk
Physical examination: Palpable gap, weakness with plantar flexion, + Thompsons test
https://www.netterimages.com/images/vpv/000/000/007/7714-0550x0475.jpg
Consult orthopedics and splint in resting equinus
http://img.medscape.com/fullsize/migrated/408/535/mos0216.01.fig5b.jpg
Perianal Group A Strep is an infectious dermatitis seen in the perianal region that is caused by Group A beta-hemolytic Strep. Children will have a characteristic rash with a sharply-demarcated area of redness, swelling, and irritation around the perianal region. There may be associated swelling and irritation of the vulva and vagina (in girls) and penis in boys. Patients can have bleeding or itching during bowel movements.
The age range is often <10 years of age. There is often an absence of fever or other systemic symptoms.The diagnosis can be confirmed by obtaining a Rapid Strep swab from the area of interest. You can also collect a bacterial culture of the area.
Treatment requires a 14 day course of penicillin. Amoxicillin (40 mg/kg/day divided TID) and clarithromycin are alternative treatments. The additional of topical bactroban (mupirocin) can be effective, but it should not be used as monotherapy. Re-occurrence is common, so close follow-up is key.