https://images.radiopaedia.org/images/3173801/1ee24da1a6fe907a27d2bf20481174.jpg
Young toddler presents with left lower leg pain. What is the diagnosis??
Patient found pulseless after submersion in water for 20 minutes. After ROSC, patient’s GCS was 3 and pupils are dilated and nonreactive.

It's Election Day in the US, so here are some interesting facts about Presidential causes of death:
George Washington likely died from epiglottitis on 12/14/1799
CLICK BELOW FOR MORE INTERESTING FACTS!
8 year-old female with no PMH who presents with concerns for "purple patches" popping up on her arm for 2-3 days. Stated that one appeared and then, the other one appeared 12 hours later. She denied any trauma whatsoever, history of easy bleeding/bruising and did feel safe at home. The rest of the review of systems was negative.
Patient said there was mild pain when the area was touched. The rest of the physical examination was normal.
What's the diagnosis? (Image below)

Do you have a patient with renal insufficiency who is in need of an anticoagulation bridge to warfarin? Subcutaneous unfractionated heparin (UFH) as an initial dose of 333 Units/kg subcutaneously followed by a fixed dose of 250 Units/kg (actual body weight) every 12 hours may be an alternative to admission for heparin infusion with monitoring.
As noted in a previous post, the FASH exam is the Focused Assessment with Sonography for HIV/TB. Below are typical ultrasound images of a positive FASH exam.
Peri-aortic lymph nodes- Multiple enlarged nodes, 97.1% specific for TB
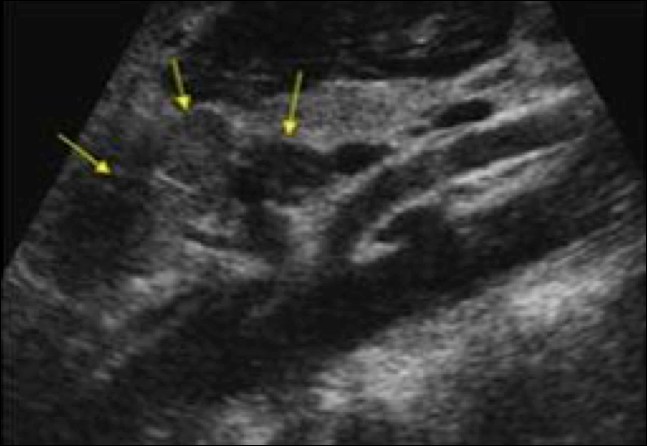
Splenic lesions – multiple ‘punched out’ lesions

The effusions often have fibrous stranding
Submitted by Dr. Laura Diegelmann
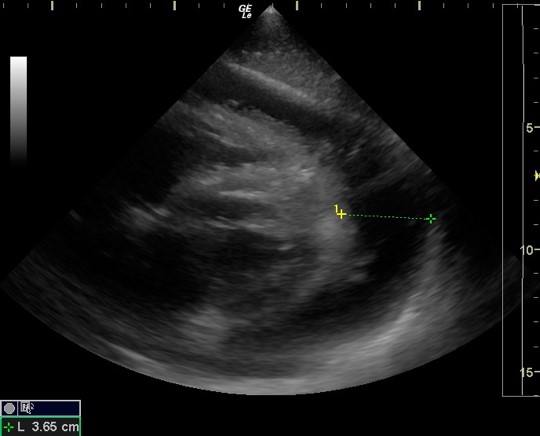
Dynamic LVOT Obstruction
30 year old female presents with a painful finger for 1 week. Finger exam showed the following. What is the diagnosis ?

Typically, empiric treatment for lobar community acquire pneumonia (CAP) in immunized < 5 year olds (preschool) is amoxicillin (45mg/kg BID or 30 mg/kg TID for resistant S. pneumoniae) for outpatient and ampicillin or ceftriaxone for inpatient. Additional coverage with azithromycin is typically recommended for school age and adolescent patients (>= 5 years), but not necessarily for younger children unless there is a particular clinical suspicion for atypical pneumonia with history, xray findings, or sick contacts.
However, in sickle cell patient with suspicion for acute chest syndrome, azithromycin is recommended for all ages groups, as atypical bacteria such as Mycoplasma are a common cause of acute chest syndrome in patients of all ages with sickle cell disease even young children. In a prospective series of 598 children with acute chest syndrome, 12% of the 112 cases in children less than 5 had positive serologic testing of M. pneumoniae (9% of all cases had M. pneumoniae) (Neumayr et al, 2003).
Recently, a retrospective study of unintentional buprenorphine/naloxone exposure among pediatric population was published. All patients were evaluated by toxicologists at the time of initial hospital presentation (or transfer) at the study center.
Bottom line
Magnetic resonance imaging (MRI) is the method of choice for imaging the spine for the suspicion of non-traumatic disorder, such as multiple sclerosis (MS), transverse myelitis, epidural abscess, spinal cord infarcts, and spondylotic myelopathy (changes in the spinal cord due to disk herniation or osteophytes in degenerative joint disease).
If the differential diagnosis includes infection, neoplasm, demyelination or inflammation, then IV contrast should be administered.
Recently Emergency Physicians have become far more aware of the importance of right ventricular (RV) function in our critically ill patient population. One of the methods that has been proposed to assess RV systolic function with bedside ultrasound (US) is the tricuspid annular plane systolic excursion (TAPSE). This simple bedside measurement utilizes M-mode to quantify the movement of the tricuspid annulus in systole. And while it has demonstrated reasonable accuracy at predicting RV dysfunction, adequate visualization of the lateral tricuspid annulus is not always obtainable in our critically ill patient population (1,2). In these circumstances an alternative measurement obtained in the subcostal window may be a viable option.
Similar to TAPSE, subcostal echocardiographic assessment of tricuspid annular kick (SEATAK) utilizes M-mode to assess the apical movement of the tricuspid annulus during systole. In a recent prospective observational study, Díaz-Gómez et al examined 45 ICU patients, 20 with known RV dysfunction and 25 with normal function. They compared the measurements obtained from TAPSE and SEATAK and found a strong correlation between the two measurement (Spearman’s ρ coefficient of .86, P=.03).
The small sample size and limited evaluation of RV function is far from ideal and more robust data sets are required before we cite SEATAK’s diagnostic accuracy with any confidence, but in the subset of patients where a TAPSE is unobtainable this may serve as an adequate surrogate until a more thorough echographic assessment can be obtained. 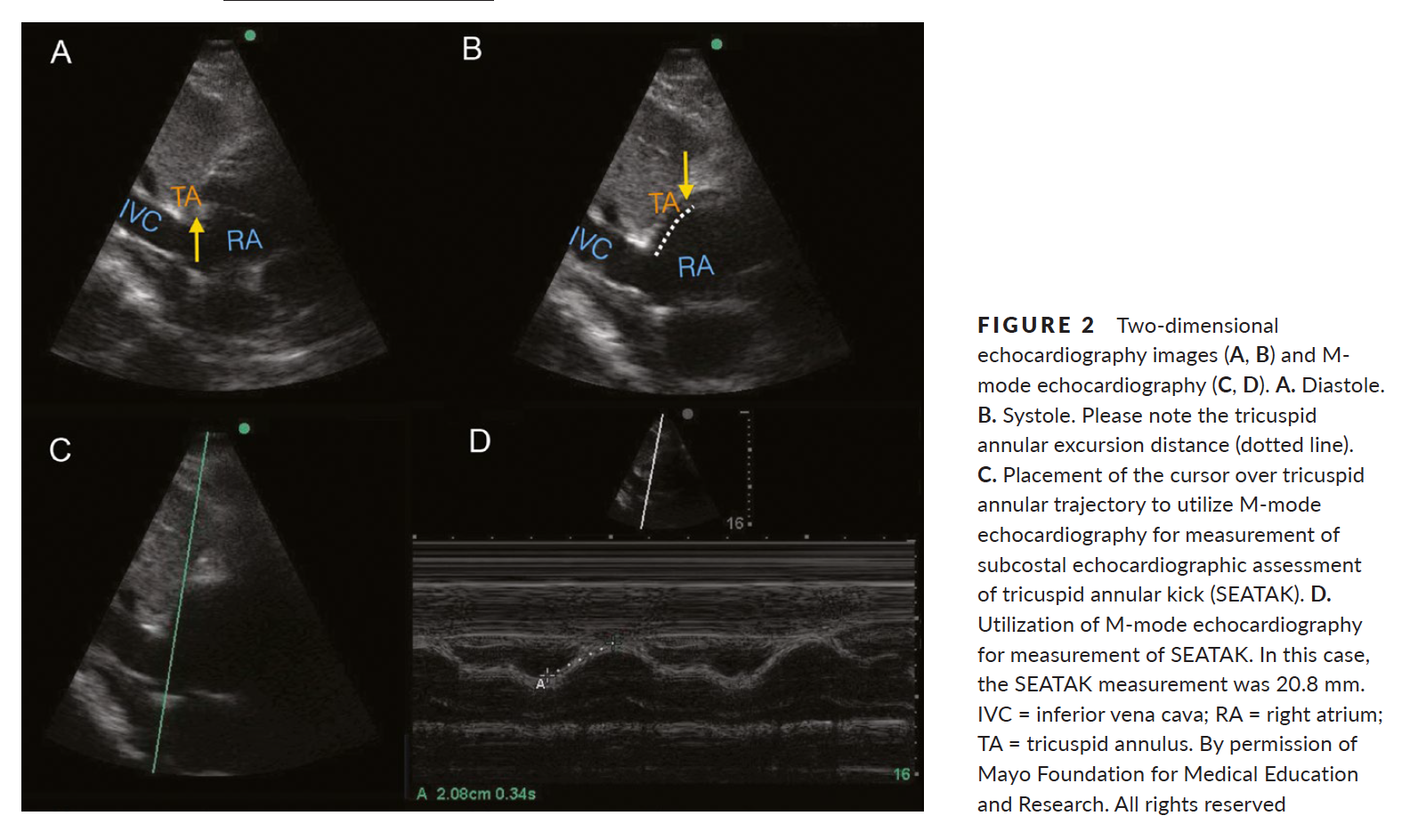
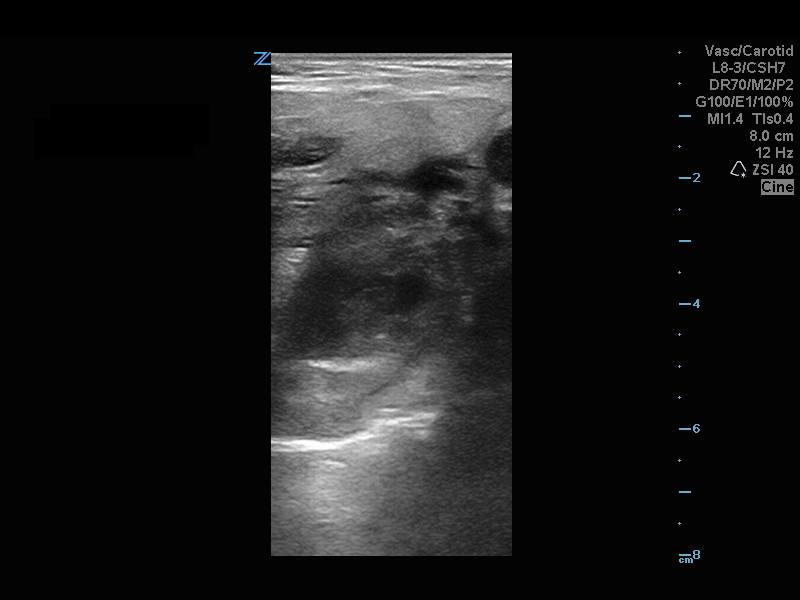
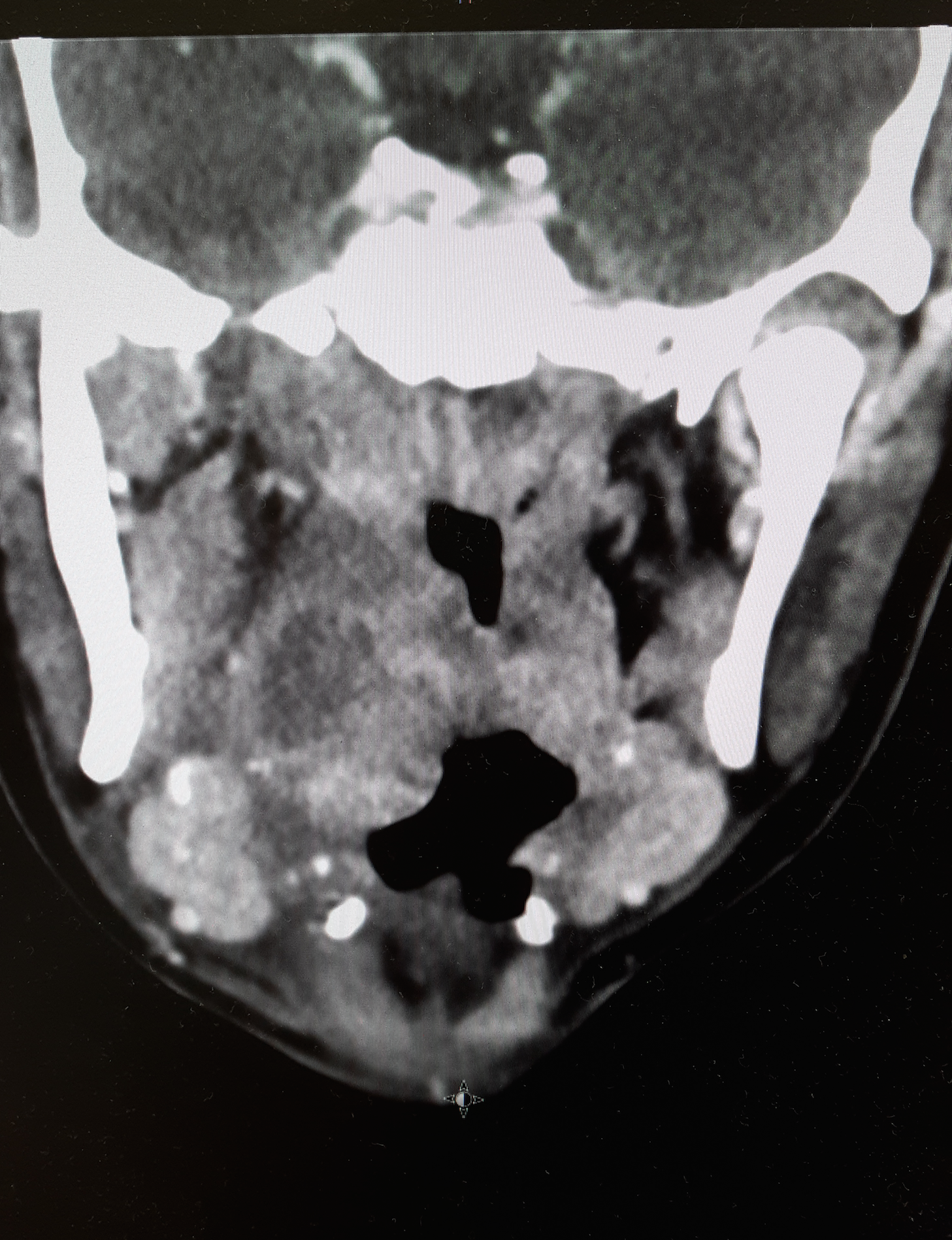
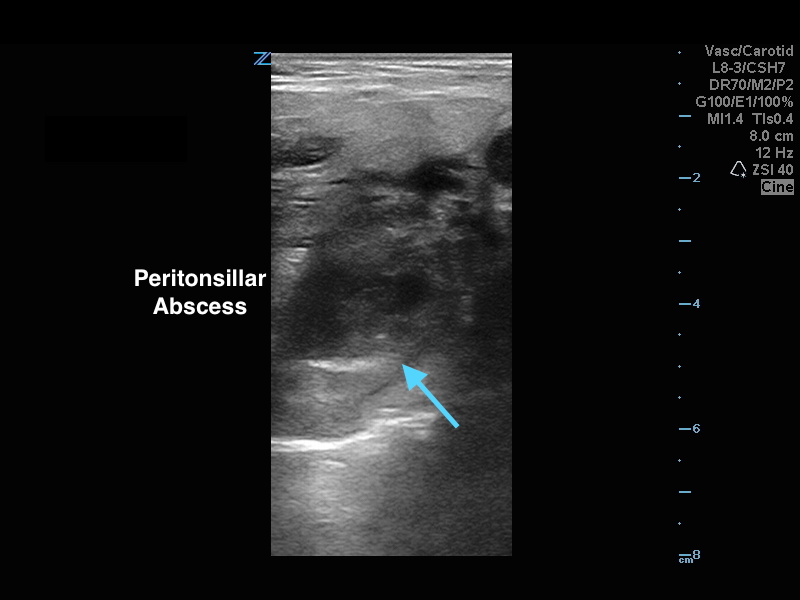
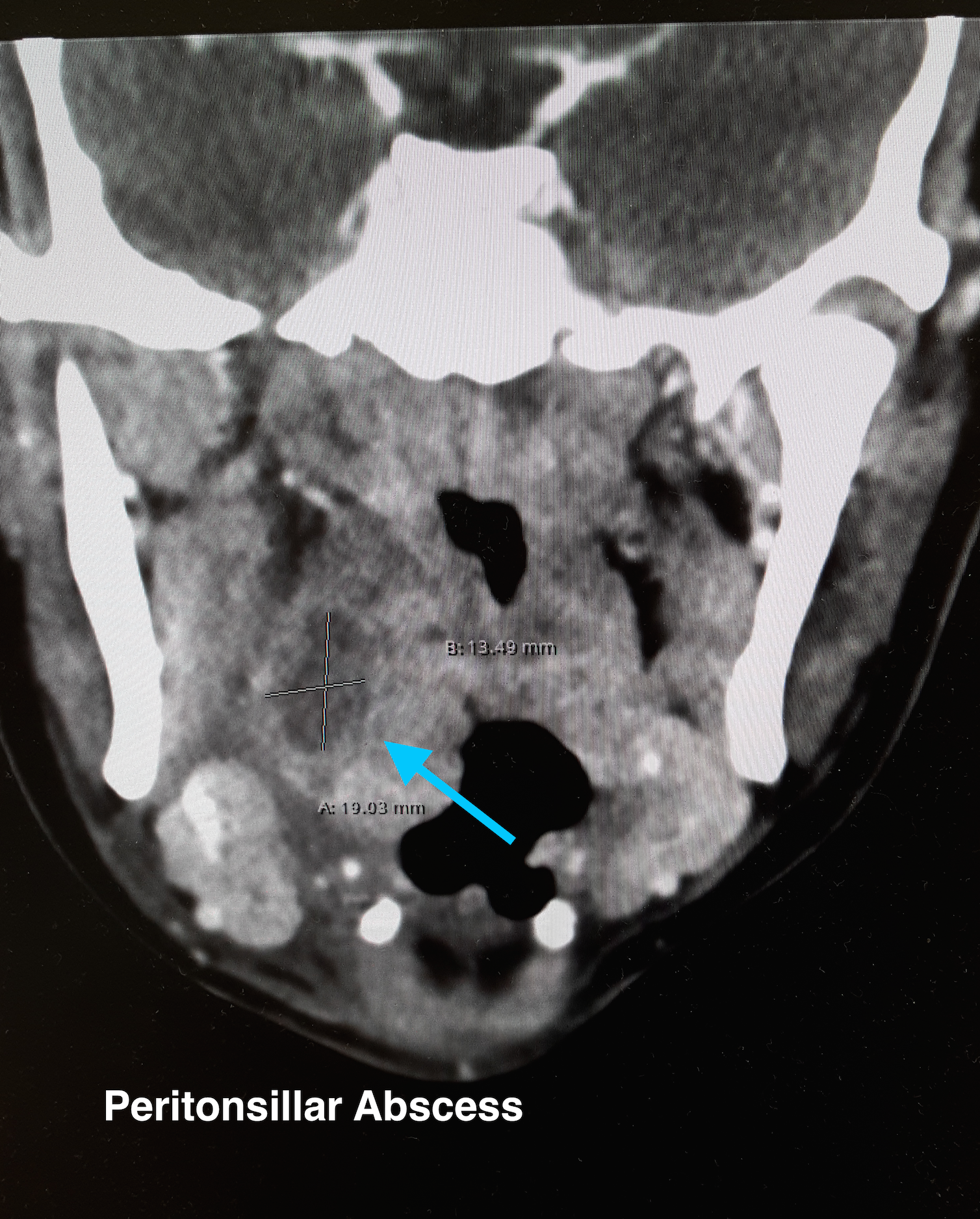
20 year-old female presents with sore throat, right throat fullness, difficulty speaking for 2-3 days. A bedside ultrasound and subsequent CT was obtained as seen below. What's the diagnosis?
Many of us use exercise as a coping strategy when emotionally stressed or to blow off steam when angry. This may place your heart at risk.
A recent observational study in Circulation surveyed 12,000 first MI patients about potential triggers. The associations didn't depend on age, smoking status, hypertension, or baseline physical activity.
Anger or emotional upset in the hour before onset elevated odds of MI 2.44 fold
A similar 2.31 fold elevation was observed form heavy exertion
However, the combination of the two raised the odds to 3.05 fold (P<0.001 for interaction)
Plasma-Lyte A outperformed 0.9% NaCl for rehydration in children with acute gastroenteritis showing a more rapid improvement in serum bicarbonate levels and dehydration scores.
--Massive PE is defined as PE with obstructive shock (hypotension [SBP <90] or end-organ malperfusion)
--Consider venoarterial (VA) ECMO in massive PE for hemodynamic support, particularly prior to intubation
--VA ECMO may prevent intubation/mechanical ventilation, surgical intervention, systemic and local thrombolysis
Davos Shoulder Reduction Technique
Take Home Points
Interested, well find out more by watching this video by Larry Mellick https://www.youtube.com/watch?v=u2MsnjVNoPM or clicking the link below.
US, Canadian and European critical care and toxicology societies recently published a consensus recommendation is the management of CCB poisoning.
Bottom line:
1. First line therapy remains unchanged: IV calcium, atropin, high-dose insulin (HIE) therapy, vasopressor support (norepinephrine and/or epinephrine).
2. Refractory to first line therapy: increase HIE, lipid-emulsion, transvenous pacemaker
3. Refractory shock, periarrest or cardiac arrest: Above (#1 & #2) plus ECMO if available.
Updated Guidelines for Traumatic Brain Injury
The Brain Trauma Foundation (BTF) Guidelines for the Management of Severe Traumatic Brian Injury (TBI) was recently updated and published in September 2016.
Updated recommendations include:
For the executive summary and complete guidelines, go to https://braintrauma.org/guidelines/guidelines-for-the-management-of-severe-tbi-4th-ed#/
Oxygen-ICU Trial
{kind=link}
{kind=link}