Haloperidol has a higher D2 receptor antagonist effect than standard antiemetic treatment agents such as metoclopramide. In addition, newer antipsychotic agents such as Olanzapine have a high affinity at multiple antiemetic sites such as the dopamine and serotinergic receptors.
While formal RCT's are still in the works, multiple sources including palliative care, emergency medicine, and pain journals support their use in refractory emesis.
Consider Haloperidol 3-5 mg IV.
Check an EKG for long QTc prior to use. Consider dose reduction of haloperidol in those with hepatic impairment. Also consider dose reduction in patients taking carbamazepine, phenytoin, phenobarbital, rifampicin, or quinidine due to that pesky CYP3A4 inhibition.
Consider Olanzapine 2-5 mg IV.
Several case reports have shown a higher rate of success with olanzapine for refractory emesis. Olanzapine has similar precautions as those to haloperidol (EKG, hepatic impairment), although it's CYP drug interactions are less common. Additionally, use olanzapine cautiously in hyperglycemic patients as there are several case reports of olanzapine prompting episodes of DKA. Consider frequent blood sugar checks or small doses of insulin in hyperglycemic patients.
Take Home Points:
Consider the antipsychotic agents Haloperidol or Olanzapine for patients with refractory emesis, they may be more effective than traditional antiemetics.
Get an EKG prior to administration to check for QTc prolongation. As the classical and atypical antipsychotic agents are sedating, use caution in conjunction with other sedating medications (such as benzodiazepines).
Ventilator Settings for the Post-Arrest Patient
Septic Arthritis in Children
Classic presentation: Pain, fever (may not always be present)
Limited range of motion of joint or refusal to bear weight,
Joint swelling (difficult to visualize in hip or shoulder),
Limb held in position that allows greatest capsular volume (elbow held in 30° flexion for example)
Diagnostic testing may include diagnostic markers (ESR, CRP) or imaging (US/MRI)
Most common organisms: Staph and Strep, Neisseria (adolescents), HACEK organisms, consider gram negatives in immunocompromised children
DDX: Transient synovitis, osteonercrosis or osteomyelitis, Psoas abscess, acute leukemia, Lyme disease
A common ED presentation is the child with the painful limp
35% of all cases of septic arthritis
>50% of cases occur in children younger than 2yo
Hip held in flexion, Abduction, external rotation
Fever and inflammatory markers are more sensitive than WBC count and refusal to bear weight
Kocher criteria:
1) Refusal to weight bear on affected side
2) Sed rate greater than 40mm/hr
3) Fever (>38.5°C
4) WBC count of >12,000 mm3
IF
- 4/4 criteria are met, there is a 99.6% chance of septic arthritis;
- when 3/4 criteria are met, there is a 93% chance of septic arthritis;
- when 2/4 criteria are met, there is a 40% chance of septic arthritis;
- when 1/4 criteria are met, there is a 3% chance of septic arthritis;
CRP can also be incorporated into a diagnostic algorithm
CRP>2.0 (mg/dl) in a child who refuses to bear weight yields a 74% probability of septic arthritis
Predictive factors of asthma development in patients diagnosed with bronchiolitis include:
- Male sex (OR 1.3)
- Family history of asthma (OR 1.6)
- Age greater than 5 months at the time of bronchiolitis diagnosis (OR 1.4)
- More than 2 episodes of bronchiolitis (OR 2.4)
- Allergies (OR 1.6)
Lactic acids are often elevated in critical care patients (e.g. septic shock). It can be also elevated in setting of drug overdose or less frequently in therapeutic use due to interference of oxidative phosphorylation. Some of the agents include:
Bottom line:
The Centers for Disease Control and Prevention (CDC) just released an official health advisory through the Health Alert Network entitled: “CDC Recommendations for Diagnosing and Managing Shigella Strains with Possible Reduced Susceptibility to Ciprofloxacin”
Concerning treatment, one key point is:
Do not routinely prescribe antibiotic therapy for Shigella infection. Instead, reserve antibiotic therapy for patients for whom it is clinically indicated or when public health officials advise treatment in an outbreak setting.
o Shigellosis is generally a self-limited infection lasting 5-7 days.
o Unnecessary treatment with antibiotics promotes resistance.
o Treatment can shorten the duration of some illnesses, though typically only by 1-2 days
Save time by using bedside ultrasound to confirm above-the-diaphragm central venous catheter (CVC) placement rather than waiting for chest x-ray confirmation:
1. Perform rapid push of saline (it doesn’t have to be agitated) through CVC while cardiac probe is placed with right atrium in view. Immediate visualization of bubbles (or “atrial swirl”) essentially confirms correct placement.
2. Perform the usual search for ipsilateral lung-sliding and the waves-on-the-beach to rule out procedural pneumothorax.
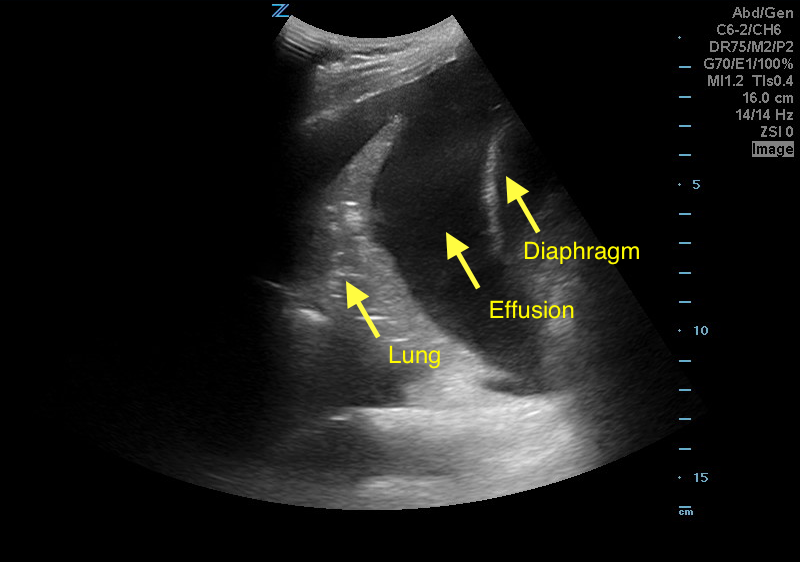
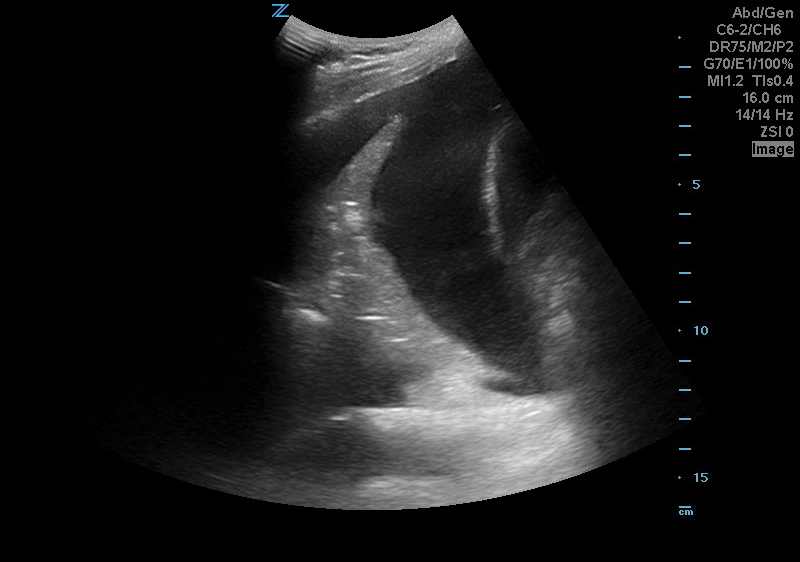
A 50 years old male with a history of CHF, presenting to the ED with progressively worsening shortness of breath. POCUS was performed. The picture shows the left lower part of the chest. What is the diagnosis?
We all wish there was a great treatment regimen for our patients with back pain. However, most studies have shown that it really does not matter what you do, as most patients will get better in 6 weeks.
A recent study published in JAMA looked at the role of spinal manipulation to improve pain and function in adults with low back pain. They looked at 26 randomized controlled trails and found that there was modest benefit for spinal manipulation and it was similar to using NSAIDs.
So spinal manipulation may or may not work for some patients. Something to consider along with physical therapy if patients are not getting relief with home remedies.
A recent study suggests that using a lower cut off value of white blood cells in dilute urine, may have a higher likelihood of detecting a urinary tract infection in children.
In dilute urine (specific gravity < 1.015), the optimal white blood cell cut off point was 3 WBC/hpf (Positive LR 9.9). With higher specific gravities, the optimal cut off was 6 WBC/hpf (Positive LR 10). Positive leukocyte esterase has a high likelihood ratio regardless of the urine concentration.
Bottom Line: The motor GCS and Simplified Motor Scale (SMS) have similar discrimination when compared with the total GCS, and may be easier to use.
The deleterious effects of hyperoxia are becoming more and more apparent. But obtaining a blood gas to ensure normoxia in a busy Emergency Department can be burdensome. And while the utilization of a non-invasive pulse oximeter seems ideal, the threshold that best limits the rate of hyperoxia is unclear.
Durlinger et al in a prospective observational study demonstrated that an oxygen saturation 95% or less effectively limited the number of patients with hyperoxia (PaO2 of greater than 100 mm Hg). Conversely when an SpO2 of 100% was maintained, 84% of the patients demonstrated a PaO2 of greater than 100 mm Hg.
Most of our knowledge of the athlete’s EKG is based on white athletes.
African/Afro-Caribbean athletes are more likely to have an abnormal EKG than white athletes in multiple studies.
Different selective criteria have been developed to minimize classification of benign normal patterns as abnormal.
The 2010 ESC criteria classified 40.4% of black athletes as abnormal versus the Refined criteria which resulted in 11.5% of EKGs classified as abnormal.
This reduction was aided by the recognition that isolated anterior TWI in asymptomatic black athletes is considered a benign finding.
Note this does NOT apply if the TWI extend to the lateral leads
For example, T-wave inversion (TWI) was present in 23% of African/Afro-Caribbean athletes vs. 3.7% of white athletes (usually in contiguous anterior leads).
Other changes included a higher prevalence of early repolarization, RV hypertrophy, and LA/RA enlargement.
FDA announced a shortage of sodium bicarbonate on 3/01/17. Sodium bicarbonate is frequently used in acid-base disorder as well as in poisoning (cardiac toxicity from Na-channel blockade, e.g. TCA & bupropion, and salicylate poisoning).
Acetate is a conjugate base of acetic acid where acetate anion forms acetyl CoA and enters Kreb cycle after IV administration. Final metabolic products of acetate are CO2 and H2O, which are in equilibrium with bicarbonate via carbonic anhydrase activity.
Administration of sodium acetate increases the strong ion difference by net increase in cations, as acetate is metabolize, and leads to alkalemia.
Adverse events from sodium acetate infusion have been associated with its use as dialysate buffer: myocardial depression, hypotension, hypopnea leading to hypoxemia and hyperpyrexia. However, such adverse events have not been reported in toxicologic application.
Bottom line:
Sodium acetate can be administered safely in place of sodium bicarbonate if sodium bicarbonate is not available due to shortage.
Sodium acetate dose:
· In the elderly, falling is the most common mechanism of injury
· Unavoidable Risk factors: age 85 or older, male, Caucasian, history of falls
· Other factors: alcohol consumption, polypharmacy
· Mechanisms of fall: slipping, tripping, stumbling
· Physical exam to include: gait, balance, proprioception, vision, strength and cognitive function testing
· Must consider neglect/abuse, affects 10% of seniors per year
· Evaluate for anticoagulant use due to increased risk of intracranial injury
· Use advanced imaging to identify occult hip fractures when clinically suspected and plain radiographs are negative
Linezolid is a weak, nonselective monoamine oxidase inhibitor (MAOI). A recent FDA Drug Safety Communication released in March 2016 noted reports of serotonin syndrome associated with certain opioids, particularly fentanyl and methadone. Development of serotonin syndrome after concomitant administration of linezolid with other serotonergic agents has been reported. Due to a potential risk of serotonin syndrome, a patient on chronic methadone should not be started on concomitant linezolid unless they will be monitored.
Sepsis remains the most common cause of death in infants and children worldwide, with pneumonia being the most common cause of pediatric sepsis overall.
Strikingly, however, the mortality rate in pediatric sepsis is significant lower in children (10-20%) as compared to adults (35-50%).
The management of pediatric sepsis has been largely influenced by and extrapolated from studies performed in adults, in part due to difficulties performing clinical trial data in children with critical illness, including sepsis.
A major difference in management of children vs. adults with refractory septic shock with or without refractory hypoxemia from severe respiratory infection is the dramatic survival advantage of children when ECMO rescue therapy is used as compared to adults.
Bottom line: Consider ECMO for refractory pediatric septic shock with respiratory failure – in kids, survival is improved dramatically – consider it early!
Children less than 5 years of age account for the majority of poisoning exposures in the United States. As expected, accessible household items are the most frequently reported exposures and include cosmetics and personal care products, household cleaning substances, medications, and foreign bodies. Opioids are responsible for the highest incidence of hospitalizations followed by benzodiazepines, sulfonylureas, and cardiovascular drugs (beta & calcium channel blockers, and centrally acting antiadrenergic agents). Rise in buprenorphine use has led to significant increases in pediatric exposures. The most common sources of prescription medications were pills found on the ground, in a purse or bag, night stand, or pillbox. The 2015 American Association of Poison Centers Annual report lists 28 fatalities in children less than 5 year of age. Fatalities occurred from exposures to the following: narcotics (9), disc and button batteries (5), carbon monoxide (4), and other substances (10).
Highlighted AAPC cases include:
Poison prevention education of patients prescribed opioids or other highly toxic "one pill killers" who have young children in their household is recommended and could be potentially life saving.