Take home points:
Acetaminophen is one of the most common pharmaceutical ingestions in overdose and a leading cause of acute of liver failure in the U.S. Early recognition and treatment is critical for prevention of morbidity.
Impact of an ED pharmacist on time to thrombolysis in acute ischemic stroke
Mechanical Ventilation in the Obese Patient
30 Year-old female presents to the ED for a rash. The rash started suddenly, mainly in her extremities and it is painful. The patient denied having fever or chills. Her past medical history is unremarkable. She admits to using cocaine frequently. The rash is shown in the picture.

Recent study evaluated whether an acetaminophen (APAP) level obtained less than 4-hour post acute ingestion can predict which patient would not require n-acetylcysteine (NAC). APAP cutoff level of 100 ug/mL was used for analysis. This was a secondary analysis of the Canadian Acetaminophen Overdose Study database (retrospective study).
Bottom line:
The prognosis of patients who experienced OHCA, who have not achieved ROSC by the time they present to the Emergency Department, is dismal. As such, it behooves us as Emergency Physicians to identify the few patients with a potentially survivable event. Drennan et al examined the ROC data base and identified the cohort of patients who had not achieved ROSC and were transported to the hospital. The overall survival in this cohort was 2.0%. Factors that predicted survival were initial shockable rhythm and arrest witnessed by the EMS providers. Patients arriving to the ED without ROSC, that had neither of those prognostic factors had a survival rate of 0.7%.
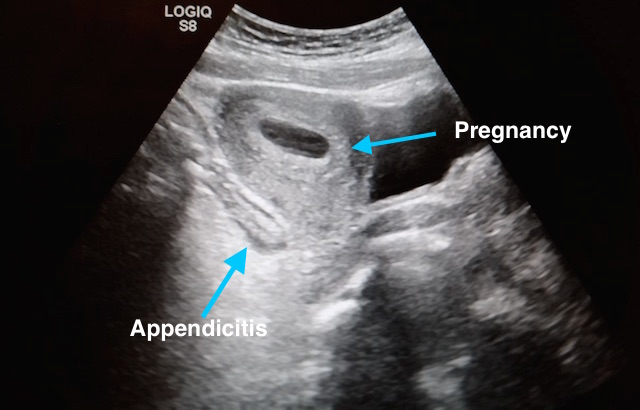
27 year-old G2P1 presents with 3 days of abdominal pain that is mostly suprapubic. Denies any urinary symptoms and vaginal bleeding. Physical examination reveals slight rebound in the right lower quadrant.
An ultrasound revealed the following. What's the diagnosis?

Consider esmolol IV 500 mcg/kg loading dose followed by a continuous infusion of 0-100 mcg/kg/min for patients in refractory ventricular fibrillation
Misclassification of adverse drug effects as allergy is commonly encountered in clinical practice and can lead to use of suboptimal alternate medications which are often less effective.
The World Health Organization announced on November 18th, 2016 that the Zika virus and associated consequences will no longer Public Health Emergency of International Concern. This changes the originally recommendation in February 2016.
However, Zika remains a “significant enduring public health challenge requiring intense action”. The consequences of the disease remains significant, especially for pregnant women and infants.
--In this study, PE was diagnosed in ~17% of patients hospitalized for syncope (though this represents only ~4%% of patients presenting to the ED with syncope).
--Patients with PE were more likely to have tachypnea, tachycardia, relative hypotension, signs of DVT, and active cancer -- take a good history and do a good physical exam!
--Consider risk stratifying (Wells/Geneva) and/or performing a D-dimer (i.e "rule out" PE) on your syncope patients, particularly when no alternative diagnosis is apparent.
Incidence and Cost of Ankle Sprains US Emergency Departments
In a sample of 225,114 ED patients with ankle sprains:
Lateral ankle sprains represent the vast majority of all ankle sprains (91%).
Lateral ankle sprains incur greater ED charges than medial sprains ($1008 vs. $914).
Lateral ankle sprains were more likely to have associated pain in the limb, sprain of the foot and abrasions of the hip/leg than medial sprains.
Medial sprains were more likely to include imaging.
Hospitalizations were more likely with high ankle sprains than lateral sprains.
There is a higher incidence of ankle sprains in younger patients (≤25 years) and in female patients (57%).
Which first-line vasoactive drug is the best choice for children with fluid-refractory septic shock? A prospective, randomized, blinded study of 120 children compared dopamine versus epinephrine in attempts to answer this debated question in the current guidelines for pediatric sepsis.
Bottom line: Dopamine was associated with an increased risk of death and healthcare–associated infection. Early administration of peripheral or intraosseous epinephrine was associated with increased survival in this population.
What Matters in Cardiac Arrest?
A 15 months old male with no past medical history, presenting with two days of decreased oral intake and decreased urine output. The exam was notable for minimal tenderness of abdomen. During an oral fluid challenge in the ED, the patient had a single episode of bilious vomiting. The ED physician ordered an ultrasound study and the results are shown below. What is the diagnosis?

Using 1.5 mg/kg or 2 mg/kg of IV ketamine led to less redosing compared to using 1 mg/kg IV.
Recently a review paper was published regarding the duration of observation in heroin overdose patients who received naloxone.
It made several conclusions regarding heroin overdose:
It should be pointed out that this is a review paper of limited number of articles with variable quality. Additionally, the clinical history of “heroin use” may be unreliable as fentanyl and novel synthetic opioids are also sold as “heroin.” Providers should exercise appropriate clinical judgement when caring for these patients.
It is well documented that when left to our own respiratory devices we will consistently over-ventilate patients presenting in cardiac arrest (1). A simple and effective method of preventing these overzealous tendencies is the utilization of a ventilator in place of a BVM. The ventilator is not typically used during cardiac arrest resuscitation because the high peak-pressures generated when chest compressions are being performed cause the ventilator to terminate the breath prior to the delivery of the intended tidal volume. This can easily be overcome by turning the peak-pressure alarm to its maximum setting. A number of studies have demonstrated the feasibility of this technique, most recently a cohort in published in Resuscitation by Chalkias et al (2). The 2010 European Resuscitation Council guidelines recommend a volume control mode targeting tidal volumes of 6-7 mL/kg and a respiratory rate of 10 breaths/minute (3).