A 12 year old with arm pain after doing push ups during gym class. What is the diagnosis?
The current opioid epidemic is considered the worst drug crisis in American history responsible for 50,000 deaths per year in the US from overdose of heroin and opioid prescription drugs. A 200% increase in the rate of overdose deaths involving opioids occurred between 2000 and 2014. The continued rise in opioid related deaths calls for an urgent need for treatment. Three types of medication-assisted therapies (MATs) are available for treating patients with opioid addiction:methadone, buprenorphine, and naltrexone. Suboxone a combination of buprenorphine and naloxone, is emerging as one of the best choices for the following reasons:
Congenital infection with the Zika virus is associated with 5 types of birth defects
· These are rarely or never seen with other infections during pregnancy
· These defects are:
1. Severe microcephaly (small head size) resulting in a partially collapsed skull
2. Decreased brain tissue with brain damage
3. Damage to the back of the eye with a specific pattern of scarring and increased pigment
4. Limited range of joint motion, such as clubfoot
5. Too much muscle tone restricting body movement soon after birth
Sepsis Mimics
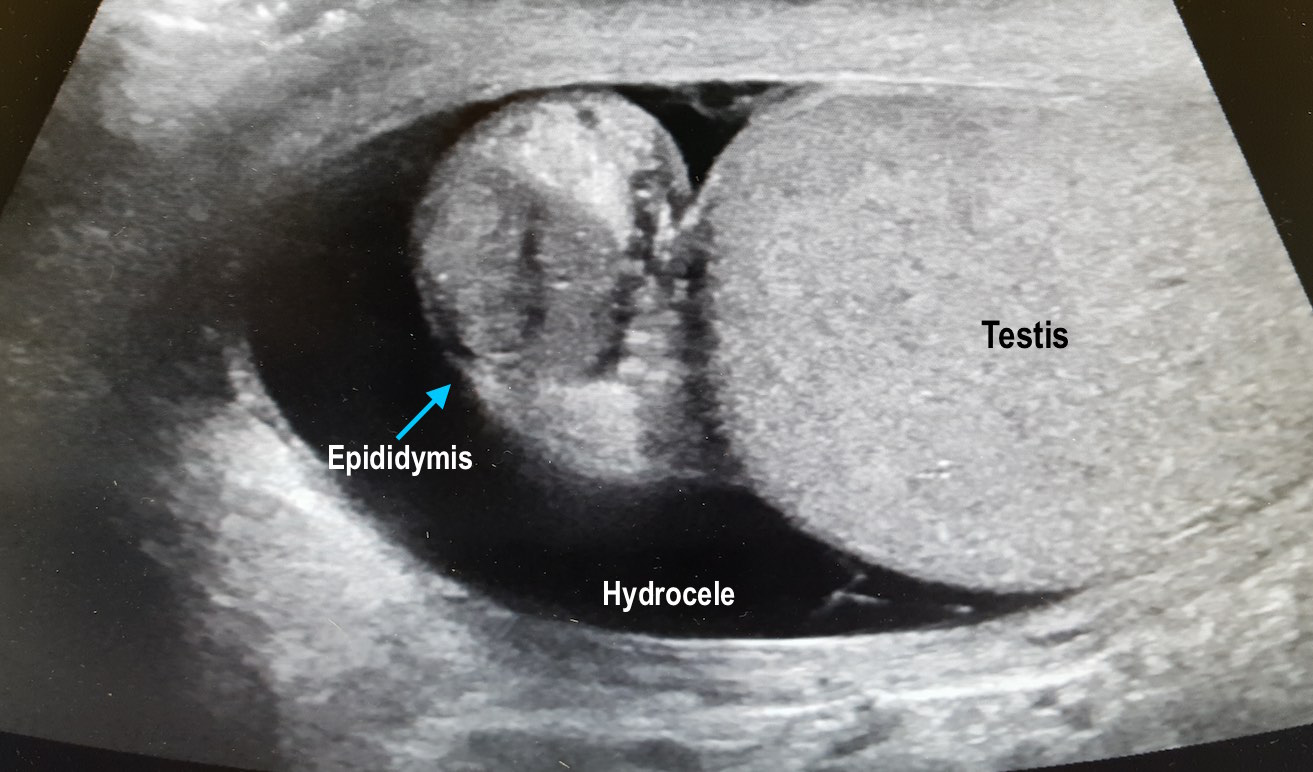
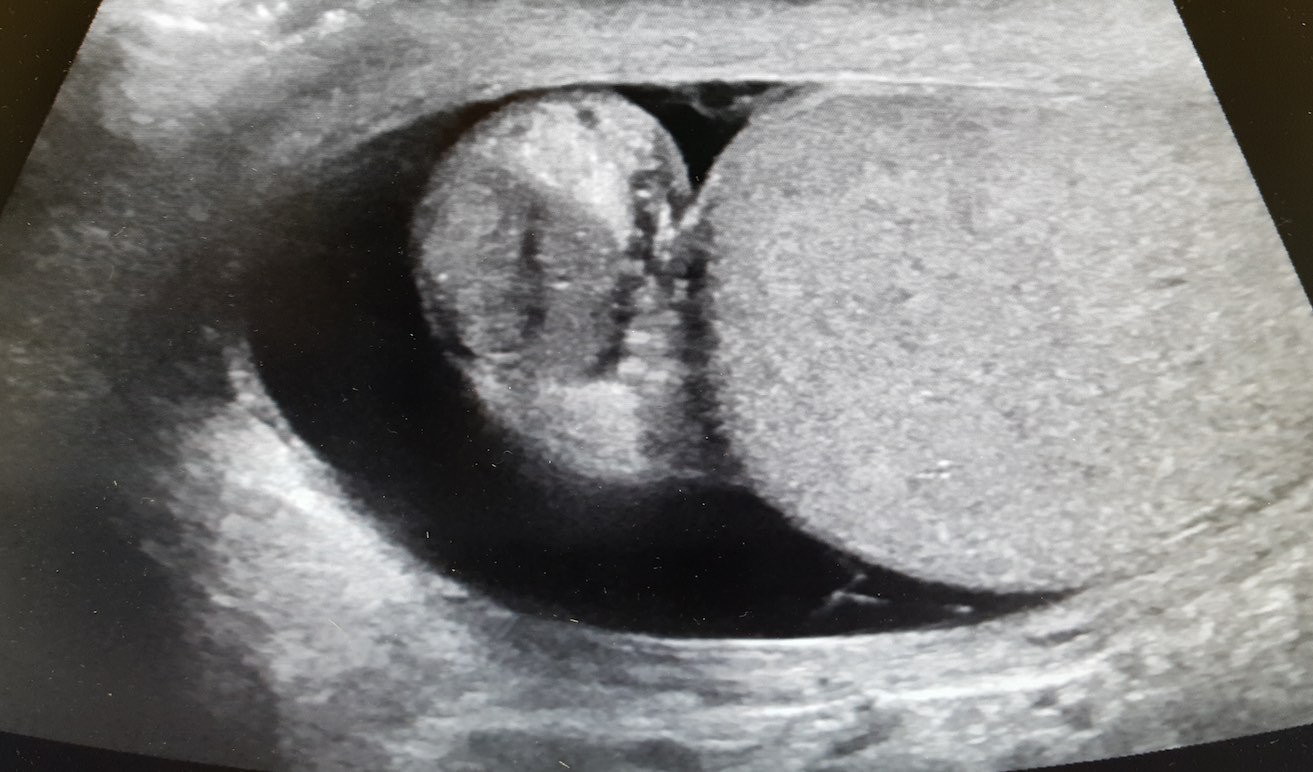
56 year-old male with history of hypertension presents with complaints of right scrotal swelling and pain. Denies any urinary symptoms, abdominal pain, nausea/vomiting or change in bowel habits or prior episodes. Temp was 99.0.
A scrotal ultrasound was done and an image of the right testis was seen (below). What's the diagnosis?
Is that a fracture or a growth plate?
Pediatric elbow x-rays are complicated to interpret due to the large number of ossification centers.
Elbow trauma is common in pediatrics.
Ossification centers of the elbow appear in a reliable chronologic pattern which aids in distinguising fractures from growth plates.
Note the age ranges are an estimate with great variability. For example, girls can develop these up to 2 years earlier than boys.
The numbers 1/3/5/7/9/11 correspond to the average age of development of each ossification center
Years of fusion shown below in ()
Capitellum (12-14yo)
Radial head (14-16yo)
Medial epicondyle (16-18yo)
Trochlea (12-14yo)
Olecranon (15-17yo)
Lateral epicondyle (12-14yo)
Pneumonic: "Can't Resist My Team Of Lawyers"
Consider ordering films of both elbows to compare if in doubt.
How is this useful? If the trochlear center is present, but there is no medial epicondyle then you are most likely looking at a fx where the ossification center has been avulsed and displaced.
Identifying patients at risk of hypotension during intubation is not always straight forward. The prevalence of peri-intubation hypotension in the Emergency Department has been demonstrated to be approximately 20%.1 And while certain variables increase the likelihood of peri-intubation hypotension (ex. Shock index> 0.80), no single factor predicts it accurately enough to be used at the bedside.2 In the majority of patients undergoing intubation, clinicians should be prepared for peri-intubation hypotension with either vasopressor infusions or push dose pressors.
24-year-old male with a history of Wagner's Granulomatosis, currently on Cellcept (Mycophenolate Mofetil) and high dose prednisolone, presented with two days of sore throat, malaise and the lesions shown in the picture. What is the diagnosis?


Below is a list of pharmacy-related pearls from the 2016 Surviving Sepsis Guidelines:
At the Society of Critical Care Meeting (SCCM) this month, updates to the Surviving Sepsis Guidelines were released. Recommendations include:
--Initial 30mL/kg crystalloid resuscitation with frequent reassessment of fluid responsiveness using dynamic (not static) measures [goodbye CVP/ScvO2!]
--Initiation of broad-spectrum antibiotics within ONE hour of sepsis recognition [two agents from different classes]
--Further hemodynamic assessement (e.g. echo for cardiac function) if clinical assessment does not reveal the type of shock [get out the ultrasound!]
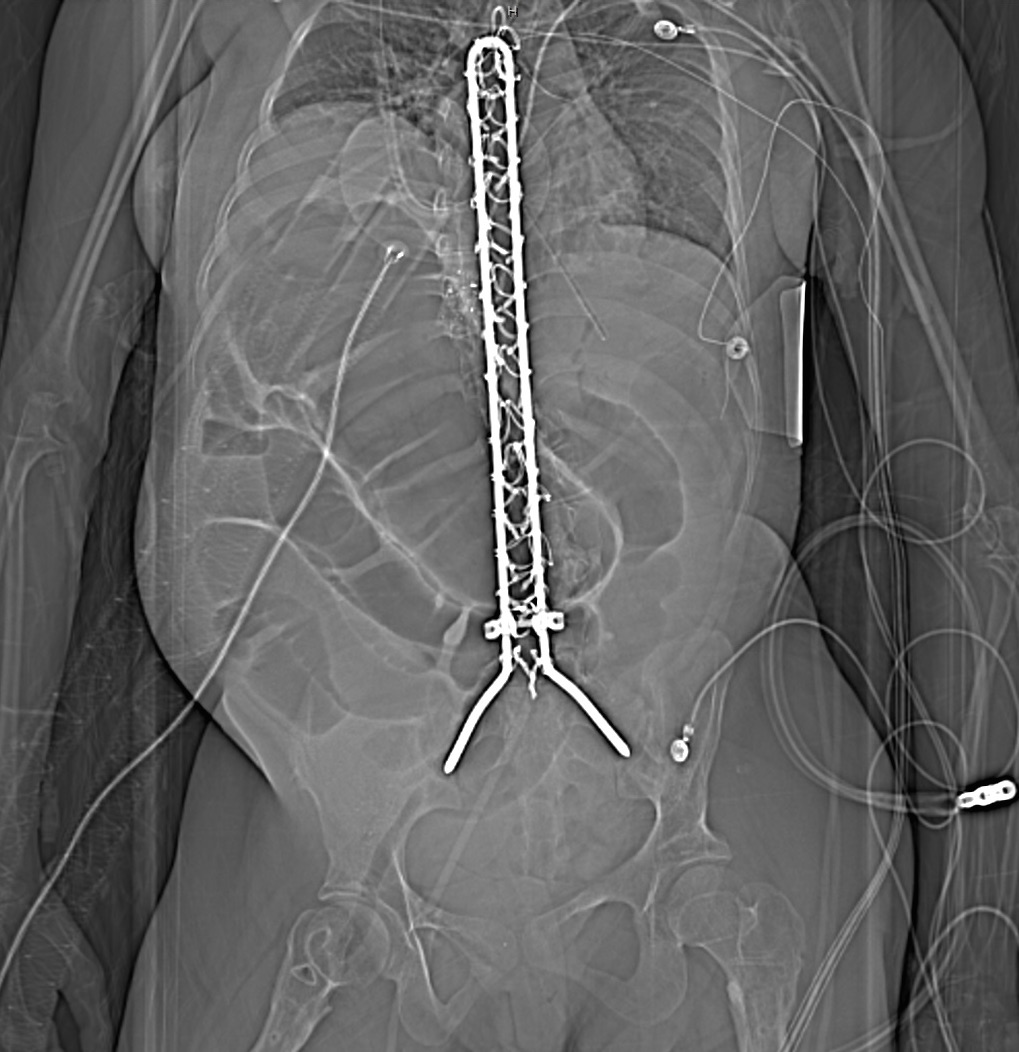
25 year-old female with hx of cerebral palsy with significant developmental delay, s/p G-tube who presented with acute hypoxic respiratory failure, hypotension and a distended, tense abdomen. A CT was done with the scout film below. What's the diagnosis?
During a busy ED shift, your 40yo charge nurse asked you to look at his hand. He is known avid mountain biker. He has pain in his right 4th and 5th digits. . He feels a lack of coordination and a feeling of “clumsiness” of the hand. Where is his possible nerve compression and what do you expect to find on exam?
Ulnar nerve entrapment is sometimes called “handlebar palsy.”
Compression location is Guyon’s canal.
The ulnar nerve supplies the intrinsic muscles of the hand AND the extrinsic muscles for flexion of the 4th and 5th digits. This is what aids in a “power grip” and why he may have diminished grip strength on exam.
Also innervates the ADDuctor pollicis and 1st dorsal interosseous muscles (pinch)
Note the ulnar nerve also passes through the radial tunnel at the elbow. Entrapment here is called Radial tunnel syndrome or Cubital tunnel syndrome and causes forearm pain and paresthesias in the 4th and 5th digits with grossly normal motor and sensory function.
As a follow up to Dr. Winter’s Pearl on Anaphylaxis on 1/24/2017, here’s a handy pearl for pediatric anaphylaxis (part 1).
Anaphylaxis: rapid and potentially life-threatening involvement of at least 2 systems following exposure to an antigen.
Medications (max: adult doses)
Get it?!?! Easy right? Instead of fumbling through an app or reference card during your next case of pediatric anaphylaxis, be a rock star "EM DR" by remembering the “Rule of 2’s”.
(Can't help it...ya'll know I love my mnemonics!!)
Methadone overdose produces classic signs and symptoms of opioid intoxication - CNS and respiratory depression with pinpoint pupils. However, methadone overdose has also been associated with hypoglycemia – a relatively uncommon adverse effect.
Bottom line:
Patients may present to the ED with new onset weakness due to myasthenia gravis (MG). A group that is frequently missed is late-onset MG, which occurs after the age of 50. It is frequently misdiagnosed as a stroke or transient ischemic attach (TIA).
Two cardinal features:
Bonus pearl: Ocular symptoms are present in up to 85% of patients with MG, with unilateral ptosis or asymmetric bilateral ptosis being the most common presentations.
Epinephrine in Anaphylaxis
More studies are needed, but the existing data shows that medical adhesives may be quicker without impacting cosmetic and functional outcome.
Urine drug screens are most commonly performed by immunoassay technology utilizing monoclonal antibodies that recognizes a structural feature of a drug or its metabolites. They are simple to perform. provide rapid screening, and qualitative results on up to 10 distinct drug classes with good sensitivity but imperfect specificity. This can lead to false positive results and the need for confirmatory testing. UDS does not detect synthetic opiates or cannabinoids, bath salts (synthetic cathinones), and gamma-hydroybutyrate. Most common drug classes detected are the following: