Recently, there have been several news reports regarding the emergence of synthetic opioids in the U.S. and Canada. There are multiple synthetic opioids that have been identified as potential agents of abuse including W-18, U-47700, fentanyl derivatives, AH-7921 and MT-45. These compounds share a similar story with synthetic cannabinoid where they were synthesized for research purpose or by pharmaceutical companies but were not marketed. They are often sold as “research chemicals” over the internet.
In July 2016, three case reports have been published regarding several cases of U-47700 intoxication in San Diego, CA and Dallas, TX.
It is unknown if currently available heroin is cut with above mentioned synthetic opioids. Like other opioid receptor agonists, administration of naloxone will likely reverse the opioid toxidrome. But clinical experience in reversing synthetic opioids intoxication with naloxone is limited.
Bottom line:
Irrespective of whether an ED patient is exposed to synthetic opioids or "traditional" opioids of abuse (prescription opioid pain medication or heroin), the management of opioid intoxication management remains unchanged for respiratory depression.
An Arbovirus is a virus transmitted primarily by an arthropod
There are a number of major arbovirus families:
The main viral family that causes substantial human disease is the Flaviviridae family.
Despite a lack of prospective data, end-tidal CO2 (ETCO2) is often proposed as a viable replacement for the traditional pulse check to identify return of spontaneous circulation (ROSC) in patients presenting to the Emergency Department in Cardiac Arrest. A recent study by Tat et al examined this very question. The authors prospectively enrolled 178 patients suffering out-of-hospital cardiac arrest (OHCA) and examined the accuracy of a rise in ETCO2 at predicting ROSC. The authors examined both a rise of 10 and 20 mm Hg in ETCO2. Of the 178 patients included in this cohort, 60 (34%) experienced ROSC. The sensitivity and specificity of ETCO2 to predict ROSC at a threshold of 10 mm Hg was 33% and 97% respectively. At a threshold of 20 mm Hg ETCO2 performed no better with a sensitivity and specificity of 20% and 99% respectively.
What this data suggests is while a rise of ETCO2 of greater than 10 is highly suggestive of ROSC, the contrary cannot be said. The absence of a spike in ETCO2 does not rule out ROSC, as the large majority of patients experiencing ROSC in this cohort did so without demonstrating a significant rise in ETCO2. This evidence suggests that ETCO2 is a poor surrogate for a pulse check.
The pediatric epiglottis is more "U" shaped, often overlies the glottic opening, and is "less in line with the trachea."1 Because of this, it has traditionally been taught that a Miller blade is the ideal laryngoscope.
Varghese et al compared the efficacy of the Macintosh blade and the Miller blade when placed in the vallecula of children between the ages of 1 and 24 months. The blades provided similar views and suffered similar failure rates. When the opposite blade was used as a backup, it had a similar success rate as the opposing blade.2 Passi et al also compared these two blades, this time placing the Miller blade over the epiglottis. Again, similar views were achieved.3
Predicting Fluid Responsiveness with ETCO2
30yo male weight lifter who 10 days ago had a painful left shoulder injury after bench press. The next morning his left anterior chest wall and left upper arm were bruised and swollen. He went to see his PCP who diagnosed him with a muscle strain. 8 days later the bruising and swelling have resolved but he still cant move his shoulder and comes to the ED.
http://321gomd.com/wp-content/uploads/2015/01/pec-major-tears.jpg
The pec major attaches to the humerus and originates from the sternum and clavicle
Injury is usually due to tendon rupture off the humerus but can also occur at the muscle tendon junction or within the muscle belly itself.
Injury is becoming increasingly common due to the popularity in power lifting sports.
Mechanism: excessive tension on a maximally eccentrically contracted muscle.
Patients will complain of pain and weakness of the shoulder.
PE: Swelling and bruising to anterior medial arm. Palpable defect and deformity or anterior axially fold (may be hidden by swelling).
Weakness and pain with adduction and internal rotation and forward flexion
Chronic presentations can be challenging to diagnose. Consider ultrasound
Non operative treatment may be indicated for partial tears (sling, ice, NSAIDs)
Operative repair of tendon avulsions is very successful. Patients age, occupation/activity level and location of injury and condition of tear are considered.
Just the Facts:
112.5-million blood donations globally and half of these come from High-income countries
High-income countries more often use blood for supportive care during surgery, in traumas or therapy for malignancies
Low and middle-income countries more often use blood to manage pregnancy-related complications or in severe childhood anemia
General availability of blood is based on the donation rate
High-income countries have 33.1 donations/1000 people
Middle-income countries have 11.7 donations/1000 people
Low-income countries have 4.6 donations/1000 people
70 countries reported collecting fewer than 10 donations per 1000 people and half of these countries were in the African region
Disease prevalence in the region is reflected in the transmission rate of transfusion-transmissible infections (TTI)
Table 1. Prevalence of TTIs in blood donations (Median, Interquartile range (IQR)), by income groups
|
| HIV | HBV | HCV |
|
|---|---|---|---|---|
| High-income countries | 0.003% (0.001% – 0.040%) | 0.030% (0.008% – 0.180%) | 0.020% (0.003% – 0.160%) | |
| Middle-income countries | 0.120% (0.020% – 0.340%) | 0.910% (0.280% – 2.460%) | 0.320% (0.090% – 0.690%) | |
| Low-income countries | 1.080% (0.560% – 2.690%) | 3.700% (3.340% – 8.470%) | 1.030% (0.670% – 1.800%) |
Submitted by: Dr. Laura Diegelmann
Non-Musculoskeletal Causes of Neck Pain
Neck pain is a common complaint of people presenting to the ED. Most of the cases will be musculoskeleteal in origin and will respond to conservative therapy with NSAIDs or acetominophen. However, other non-musculoskeletal causes of pain could be lurky behind this benign complaint.
Don't forget to consider:
Although it is summer, preparations are being made for the 2016-2017 influenza season. The Center for Disease Control (CDC) no longer recommends the live attenuated influenza vaccine (LAIV4). The American Academy of Pediatrics has supported this statement.
The LAIV4 (the only intranasal vaccine available) was offered to patients over the age of 2 years without respiratory problems. Observational studies during the 2013-2015 seasons have shown that the LAIV4 has an adjusted vaccine efficacy of 3% compared to 63% for the inactivated vaccine (intramuscular). Children who received the intranasal vaccine were almost 4 times more likely to get the flu compared to children who received the injection.
Bottom line: Only the intramuscular shot is recommended for this upcoming season. This is causing many primary care practices to scramble to obtain enough vaccine.
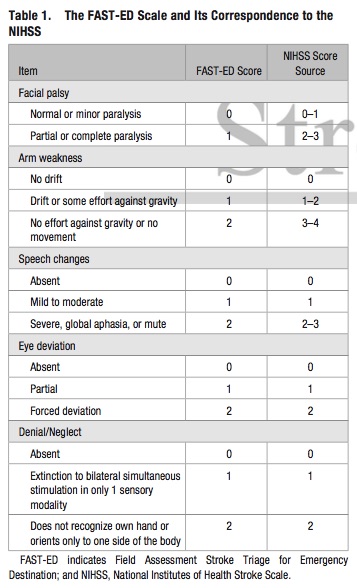
Bottom Line: Additional assessment of gaze deviation, aphasia and neglect, as included in the FAST-ED scale, increases the accuracy of predicting LVOS.
LVADs and RV Failure
Sesamoid Injuries
Unlike other bones in the human body that are connected to each other at joints, sesamoid bones are only connected via tendons (or are imbedded in muscle).
The largest sesamoid bone is the patella.
2 small sesamoid bones lie on the plantar foot near the great toe
Sesamoid bones can fracture and the surrounding tendons can become inflamed (sesamoiditis)
Traumatic injury is usually due to hyperextension and axial loading
Sx: Pain located under the great toe on the ball of the foot (Gradual with sesamoiditis and acutely with a fracture).
There may be associated swelling and bruising. Pain with palpation, flexion and extension.
The medial/tibial sesamoid is larger, has great weight bearing status and is more commonly injured that its lateral counterpart.
In many people (10 - 25%) the medial sesamoid of the foot has two parts (bipartite). This finding is bilateral in 25% of people.
This may confuse some providers as it may appear to be a fracture
Look for a smooth contour to the bones and clinically correlate (bruising, soft tissue swelling, etc.) if it is an incidental finding.
Other radiographic clues include
1) The fractured sesamoid is usually slightly larger than the lateral sesamoid while the bipartite sesamoid has a much larger medial sesamoid than lateral sesamoid
2) The fractured sesamoid shows a sharp, radiolucent, uncorticated line between the two fragments while the bipartite sesamoid has two corticated components
3) The fractured sesamoid fragments often fit together like pieces of a puzzle while the bipartite sesamoid has two components that do not fit together snugly
4) Other means to differentiate the two involve MRI and bone scanning
Treatment involves a stiff-soled shoe or applying a cushioning pad or J-shaped pad around the area to relieve pressure.
It may take months for the pain to subside.
http://www.apfmj-archive.com/afm5_3/afm50.htm#F1
There are many definitions for a disaster. Per the International Federation of Red Cross and Red Crescent Societies (IFRC), they define a disaster as:“…a sudden, calamitous event that seriously disrupts the functioning of a community or society and causes human, material, and economic or environmental losses that exceed the community’s or society’s ability to cope using its own resources. Though often caused by nature, disasters can have human origins.”
However, in the heat of the moment, a shorter definition is easier to remember. The IFRC also define a disaster as:
A shorter, more practical definition is:
Fluoroquinolone antibiotics are used to treat a wide range of infections and as prophylaxis against infection in certain immune compromised patients. In 2008 the FDA issued a boxed warning for tendonitis and tendon rupture for the fluoroquinolone antibiotic class, and in May 2016 a statement recommending the use of alternate therapies for uncomplicated UTIs and upper respiratory infections was issued. The mechanism by which fluoroquinolones causes tendon injury has not been elucidated, but may be related to oxidative stress caused by the overproduction of reactive oxygen species in tenocytes.
Adverse event reporting to the FDA is performed voluntarily by healthcare professionals and consumers through MedWatch. An analysis of tendon rupture events associated with fluoroquinolone use reported to the FDA’s Adverse Event Reporting System (FAERS) database was recently published.
What they found:
Application to clinical practice:
Plain films are commonly used to screen children for pelvic fractures or dislocations following blunt torso trauma
The sensitivity of this common screening practice is unknown
A recent study looked at this question.
Of 451 patients with pelvic fractures or dislocations, 382 had AP radiographs. Injury was correctly identified in 297 patients (sensitivity 78%).
The sensitivity was greater in the sicker subgroups :92% for those requiring operative intervention and 82% for those with hypotension
Plain AP pelvic radiographs should have a limited role in the sole evaluation of children with blunt torso trauma.
They should be incorporated in the assessment of hemodynamically unstable children and those in whom the clinician is not planning on otherwise obtaining an abdominal/pelvis CT.
Laundry detergent pods were introduced in 2012 to make washing clothes more "convenient." Since then, pediatric exposures to laundry detergent pods have increased as the use of these detergent pods have become more common in homes. Like other household chemical exposure, small, colorful candy like appearances of laundry detergent pods can attract the attention of < 3 years old children resulting in unintentional exposure due to curiosity or taste.
Most frequent clinical effects (2013 - 2014 national poison center data) from exposure to detergents in general (laundry detergent pods and nonpods & dishwasher detergent):
Laundry detergent pod vs. nonpods:
Laundry detergent pods (only) also resulted in following:
Cases of caustic exposure-like injuries have also been reported (corneal abrasion and esophageal injury)
Bottom line:
Pediatric laundry detergent (nonpods) exposures usually have self-limited symptoms. However, laundry detergent pod exposure can cause more serious clinical effects that may require hospitalization.
Multiple sclerosis (MS) relapses are defined as new or worsening neurologic deficits lasting 24 hours or more in the absence of fever or infection. Symptoms may be visual, motor, sensory, balance or cognitive. It is a clinical diagnosis, but the presence of a new gadolinium-enhancing lesion on MRI can be used as a radiologic marker of an MS relapse. However, it is unclear whether asymptomatic lesions should be treated, making it prudent to rely on the clinical evaluation rather than the MRI for diagnosis.
Moderate to severe relapses should be treated within 1 week of onset. The mainstay of treatment for relapses is IV methylprednisolone, usually dosed at 500mg to 1g per day for 3-7 days.
Similar symptoms occurring in the presence of fever, heat exposure, stress or infection (such as urinary or upper respiratory tract infections) are "pseudoexacerbations", and should not be treated as an MS relapse.
There are 4 types of respiratory failure that all providers should be familiar with
Type 1: Hypoxemic, PaO2 <50; this can include shunt , V/Q mismatch, or high altitude. Pulmonary edema, ARDS, pneumonia are common causes of this type of failure.
Type 2: Hypercapnic respiratory failure; decreased RR or tidal volume. This includes neuromuscular disorders including GBS or Myasthenia Gravis, in addition to medication overdose. COPD and asthma can lead to this type of respiratory failure as well.
Type 3: Peri-operative; atelectasis; decreased FRC from being supine or obese during the operative period.
Type 4: Shock or hypoperfusion leading to increased work of breathing and respiratory failure.
{kind=link}