AKI in the Critically Ill Cancer Patient
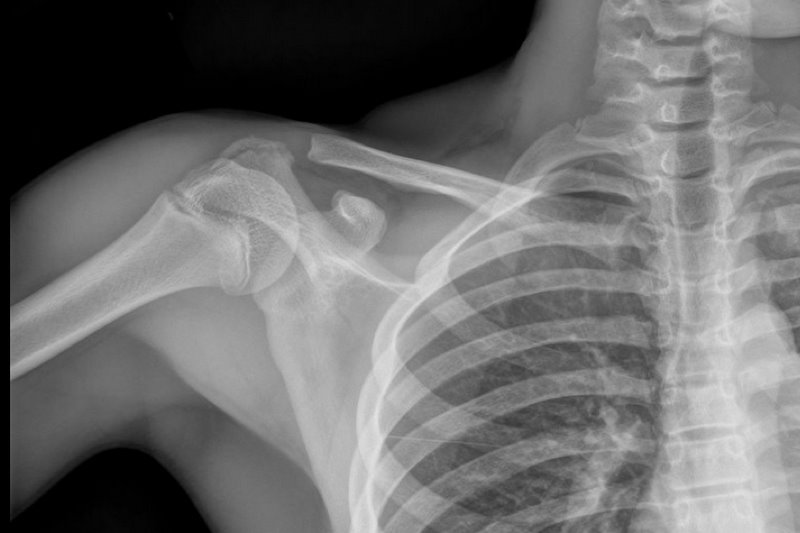
13 y.o. with shoulder trauma (during basketball game). Arm held in adduction and exquisite scapular tenderness. Diagnosis?
Proton pump inhibitors should be avoided in patients being treated with clopidogrel. PPIs appear to attenuate the effect of clopidogrel, and there's even some suggestion that the addition of PPIs to the medication regimen of patients taking clopidogrel may be associated with an increased risk of rehospitalization or death.
Kienbock’s disease is a rare entity involving collapse of the lunate due to avascular necrosis and vascular insufficiency.
Occurs most commonly in young adults aged 15 to 40 years.
Cause is unknown but believed to be due to remote trauma or repetitive microtrauma in at risk individuals.
Patients complain of wrist pain, stiffness and swelling
On exam, limited range of motion, decreased grip strength and passive dorsiflexion of the 3rd digit produces pain.
Dx: plain film in the ED and with MRI as an outpatient.
Tx: Wrist immobilization with splint and refer to orthopedics. Ultimate treatment is individualized and there is no clear consensus.
Lunate sclerosis seen on plain film
http://orthoinfo.aaos.org/figures/A00017F02.jpg
AVN of the lunate seen on MRI
http://www.assh.org/Public/HandConditions/PublishingImages/KeinbocksMRI_figure3.JPG
If there is a single truth of pediatric emergency medicine, it is that kids love to stuff things into their noses. A particular danger (aside from batteries, covered in a previous pearl) is the magnet.
Specifically, two magnets (as seen with magnet ear and nose rings, frequently worn by children and teens whose pesky parents won't allow piercings), attracted across the nasal septum can cause necrosis and perforation within hours.
Here's how to save yourself (and some noses):
Dehydration and subsequent prerenal acute kidney injury can result when temperatures begin to rise in the summer months. As a result, medications with narrow therapeutic indices that are primarily renally excreted may accumulate. Here are the specific ones to look out for:
Bleeding associated with uremia is a spectrum, from mild cases (e.g., bruising or prolonged bleeding from venipuncture) to life-threatening (e.g., GI or intracranial bleed). The exact pathologic mechanisms are not understood, but are likely multi-factorial (e.g., dysfunctional von Willebrand’s Factor (vWF) and factor VIII, increased NO, etc.)
Besides dialysis, treatments for uremic bleeding include:
A 20 year-old female presents with bilateral neck pain that occurred at rest. No other complaints. See if you can find the subtle clue on the x-ray...

Prasugrel is a new thienopyridine alternative to clopidogrel and is now listed as an option in the 2011 ACC/AHA Non-STEMI ACS Guidelines. Studies comparing it versus clopidogrel show a slight benefit in terms of adverse cardiac events, but at the expense of a slight increase in bleeding complications. Though the guidelines state no preference between prasugrel vs. clopidogral for NSTEMI ACS patients, prasugrel is finding a role in patients who appear to have a genetic resistance to the effects of clopidogrel (unlikely you'll know this in the ED, but you'll start seeing more patients started on this medication in the outpatient setting).
Prasugrel is contraindicated in patients with a history of TIA or stroke and it should not be given before cath is performed (in contrast, some protocols push for clopidogrel as early as possible, even before cath).
Pathophysiology: Angiotensin converting enzyme (ACE) catalyzes the conversion of angiotensin I to angiotensin II. It also degrades bradykinin. Thus, ACE inhibitors have the effects of decreasing angiotensin II and increasing bradykinin. In the presence of ACE inhibition, bradykinin can accumulate and interact with vascular bradykinin B2 receptors, causing vasodilation, increased vascular permeability, increased c-GMP, and release of nitric oxide.
Treatment: Even though we generally treat with standard allergic reaction medications, none counteract the mechanism causing the problem. Steroids, H1-blockers, and H2-blockers should still be considered but may not alter the progression. Airway monitoring and management is paramount.
Certain medications can cause a certain dermatologic pattern. Many fall into a generic waste basket of "contact dermatitis" but here are some more characteristic findings and the drugs that can cause them:
Alopecia - anticoagulants, chemo, phenytoin, retinoids, selenium, thallium
Erythema multiforme - allopurinol, barbiturates, carbamazepine, cimetidine, some antibiotics
Toxic Epidermal Necrolysis (TEN) - allopurinol, bactrim (sulfonamides), mithramycin, PCN, sulfasalazine, nitrofurantoin, phenytoin, prazocin
| PERIPHERAL | CENTRAL | |
| Nystagmus | ||
| Direction | Fast phase away from lesion; never reverses direction | Sometimes reverses direction if looking in direction of slow phase |
| Type | Horizontal with torsional component, never purely torsional or vertical | Can be in any direction |
| Other neurologic signs | Absent | Often present |
| Postural instability | Unidirectional instability, walking preserved | |
| Effect of visual fixation | Suppressed | Not Suppressed |
| Deafness or tinnitus | May be present | Absent |
Cardiovascular Complication of ESLD
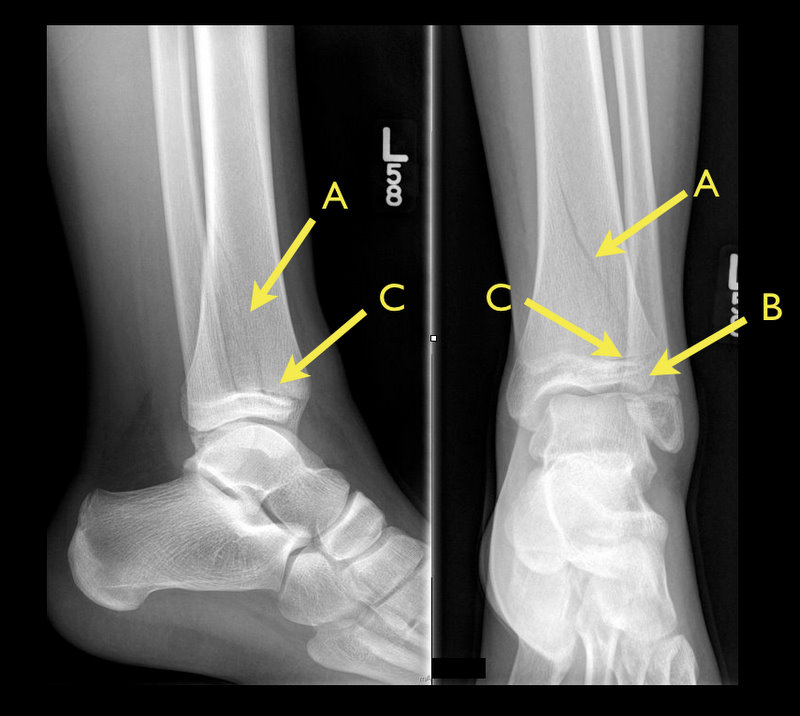
13 y.o. female with ankle pain following fall down escalator. What's the diagnosis? (Hint: Look very closely)

Therapeutic hypothermia in post-cardiac arrest patients with return of spontaneous circulation + coma (GCS < 8) is now well-accepted, and the current recommendations are for continued sedation of these patients. Consider avoiding the use of midazolam for sedation in these patients. Midazolam is metabolized more slowly in hypothermic patients, resulting in accumulation and the potential for longer ventilation and ICU time.
Transient brachial plexopathies aka Burners and Stingers
Brachial plexus injuries are the most common peripheral nerve injuries seen in athletes.
49-65% of all college football players have experienced at least one burner with a 87% recurrence rate.
Injuries most commonly occur at C5-C6 but may involve any root level.
3 Mechanisms: Commonly due to
1) Traction caused by lateral flexion of the neck away from the involved side
2) Compression of the upper plexus between shoulder pads and scapula
3) Nerve compression caused by neck hyperextension and ipsilateral rotation.
CC: Burning or numbness in the neck, shoulder and/or arm
Symptoms are UNILATERAL and tend to usually last seconds to minutes
Symptoms are reproduced by the Spurling maneuver.
Function gradually returns from the proximal muscle groups to the distal muscle groups.
Because most burners are self-limited, the most important goal is to rule out an unstable cervical injury.
TIP: Suspect when abdominal pain presents 10-14 after chemotherapy (when PMNs are lowest).