[Here's a nice simple pearl from Jeff Tabas, MD (Prof of EM at UCSF).]
3 causes of bradycardia to consider when the rhythm is not clearly sinus bradycardia:
1. Junctional bradycardia
2. Hyperkalemia
3. Digoxin toxicity
Distal Radius Fractures
Typically distal radius fractures are treated with closed reduction and splinting in the ED, followed by operative repair. This is done because it is felt that patients will have the best functional outcomes if the bones are restored to their normal anatomic alignment. However, two studies published in 2010 suggest differently.
The study by Neidenbach showed that after one year there was no difference in functional outcomes between patients that were just splinted in the ED in the position the fracture was found versus those that had closed reduction with splinting.
The second study by Ego showed that there was no difference in outcomes between those that underwent conservative treatment with closed reduction and splinting versus those that underwent operative repair.
The take home point from these studies for the EM physician is that most distal radius fractures can be splinted in the position found with them following up with an orthopaedist. There is probably little advantage to performing a closed reduction in the ED knowing that this procedure can use a lot of valuable time and resources.
Sold under the name of K2, Spice. Patients exposed to this will present with dry mouth, paranoia, tachycardia, hallucinations but will resolved rather quickly over several hours. Observation in the ED and supportive care is usually all that is needed. A little history about synthetic marijuana:
(Please note the prior version of this pearl was incorrect with respect to the images referenced. This version is corrected.)
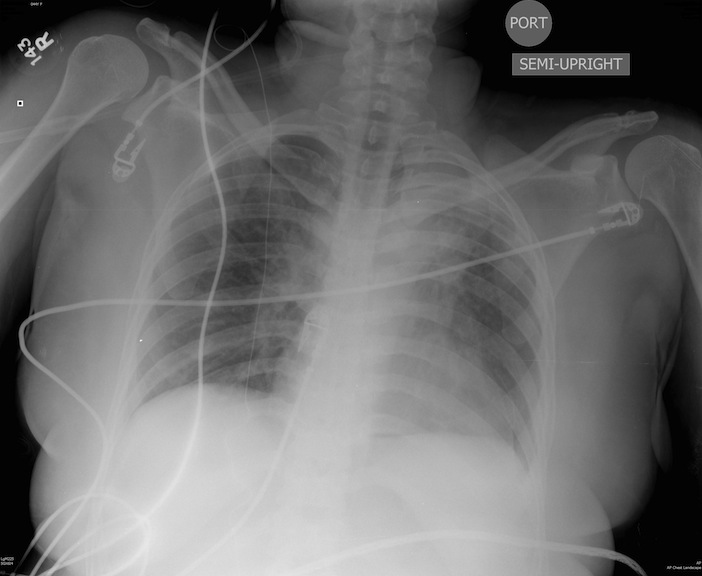
Patient s/p blunt chest trauma. CXR (image 1) vs. lung ultrasound (image 2), do you see any inconsistencies?
Is there a difference in the workup, etiologies, or prognosis between patients with syncope vs. near-syncope? Traditional teaching indicates that there is no difference, but that doesn't necessarily reflect common practice. Physicians sometimes are a bit less concerned about patients with near-syncope vs. patients with true, full-blown syncope; and many syncope studies exclude patients with near-syncope.
Grossman and colleagues recently published a useful reminder that patients with syncope and near-syncope have a similar 30-day rate of adverse outcome. However, they have a lower admission rate, reflecting the lower level of concern physicians have in their evaluation. Be wary of those patients with near-syncope. Don't be reassured just because they didn't hit the floor...yet!
Many consider Paracelsus (1493–1541) as the father of modern toxicology.
The introduction of the dose–response concept might have been his most important contribution to toxicology, meaning that everything is toxic at the right dose (even oxygen and water).
-- Age > 80 years old
-- NIH Stroke Scale > 25
-- History of combination of previous stroke and diabetes
-- On anticoagulation medication, regardless of INR
Acute LV Dysfunction in the Critically Ill
Great resource for teaching in the emergency department....
Here is a great new app that you can use when teaching residents and students in the ED. It's the NEJM app. Great pics, videos, audio, procedures, and articles. And, it's FREE.

Just go to the App store and search "NEJM"
For those that listen to EmedHome's EM Cast, you may have already heard this but I thought it's worth sharing with everyone else:
Many of us learned in our training that you should never give calcium to a hyperkalemic patient that is on digoxin or has digoxin toxicity. However, there's a paucity of data to support this contention. Here's one more article suggesting that calcium in the presence of digoxin or dig-toxicity may, in fact, be okay.
Levine and colleagues retrospectively evaluated 161 patients with digoxin toxicity, of whom 23 patients received calcium for hyperkalemia. None of the patients developed significant dysrhythmias in the first hour after calcium, and there was no increase in mortality rate.
Though not definitive, this is further support for treating hyperkalemia with calcium even in the presence of digoxin toxicity.
Many patients report an allergy to iodinated RCM, sometimes adding to the complexity of diagnostic decision making. Here are a few pearls to help:
Bottom line: Despite the lack of cross reactivity with shellfish/iodine allergies AND the very low risk associated with today’s low osmolality agents, premedication is still indicated in patient’s with a history of IHR to RCM.
Head injuries in children under 2yo are stress provoking, particularly with regard to when you should be getting a head CT. Luckily, a large (42,412 children, 10,718 <2yo) multi-center trial exists to guide your behavior.
The optimal hemoglobin concentration during critical illness is unknown. Although a liberal transfusion strategy (Hb 10-12 g/dL) was once believed to be beneficial for hemodynamics, evidence suggests targeting a conservative strategy (Hb 7-9 g/dL) does not increase mortality, while the unnecessary transfusion of blood products can cause harm (transfusion associated lung injury, infection, etc.) in the non-hemorrhaging patient.
44 y/o female restrained driver s/p motor vehicle crash complaining of chest pain and shortness of breath.