Dabigatran (Pradaxa), an antithrombin medication, was discussed in an earlier pearl and thought I would play devil's advocate and explain the possible concerns:
Toxicology Mantra: You never want to be the first person or the last person to use a drug
|
Valproic Acid in Status Epilepticus
Well, there may finally be a replacement for patients with atrial fibrillation who take warfarin (Coumadin).
In late 2010, the FDA approved the drug Dabigatran (Pradaxa) for use in patients with atrial fibrillation.
Dabigatran is an oral direct thrombin inhibitor that has been approved for stroke prevention in patients with A Fib. The drug does not need monitoring like warfarin, and has been deemed to be safer than warfarin.
Be on the lookout for Dabigatran...
Bretylium was touted for many years as the drug of choice for patients with ventricular dysrhythmias in the setting of hypothermia...in fact it still is recommended by some. Bretylium was actually touted to be effective based on animal studies in which the dogs were PRE-treated with bretylium and then hypothermia was induced. It was found that dogs that were pretreated had fewer episodes of ventricular fibrillation than dogs that were not pretreated. On the other hand, if bretylium was used as a treatment for VFib rather than a prophylactic, it was ineffective. The bottom line....don't bother with bretylium.
Iliotibial band syndrome (ITBS)
http://footcarexpress.com/foot-orthotics/wp-content/uploads/2009/01/iliotibial-band-syndrome.jpg
Hx -
PE-
Tx
Brain death is the permanent absence of cerebral and brainstem functions (coma, absent pupillary reflexes, no spontaneous respiration, etc.). Legally, brain death is equivalent to cardiopulmonary death.
If brain death is suspected, confirmation is necessary. The apnea test is most commonly used, evaluating for spontaneous breaths when disconnected from the ventilator. If apnea testing is not possible (e.g., ambiguous clinical exam or cardiopulmonary instability) ancillary testing is needed:

Boxer's (or Brawler's) Fracture
Up to 30-40% of patients with infective endocarditis have neurological symptoms as a result of embolization. This is a good reminder of the frequency of embolization, and also that infective endocarditis should always be part of the differential when you are evaluating a patient with fever + neurological abnormalities.
FARES Method for Reduction of Anterior Shoulder Dislocations.
This method that was recently highlighted in a publication had a ~78% success rate with the authors able to reduce the shoulder in an average of 2.36 ±1.24 minutes without having to give the patients any analgesics or sedatives. The technique is done by:
Consider trying this with your next shoulder dislocation. No single method of reduciton is 100% successful, but methods like this that only require a single provider and do not require analgesics are extremely helpful in improving patient flow as they do not utilize a lot of ED resources..
The Rumack-Matthew nomogram is a well studied and validated tool to help assess the potential for liver toxicity following acute acetaminophen poisoning. Here is a brief review of when it is best utilized.
Outside-the-box situations:
Dexmedetomidine for Sedation in Acute Neurologic Disease
FILE RESEND. This was tested via email and will hopefully work. I apologize for errors - Dlemkin (webmaster)
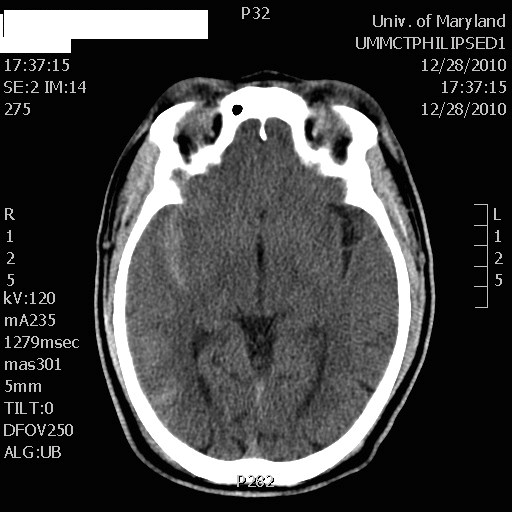
What is the diagnosis? (DON'T LOOK DOWN AT THE ANSWER)
50 year-old male prisoner s/p assault, + LOC
CT shows right-sided traumatic subarachnoid hemorrhage
Therapeutic hypothermia is generally accepted as a useful intervention that should be employed in patients that are resuscitated after cardiac arrest. Many protocols for cooling are relatively complicated, involving endovascular catheters, cooling blankets, cooling helmets, or other devices that are expensive and not widely available. The cooling process can actually be fairly simple, however, with ice and cool IV fluids. The most recent study that demonstrated this used nothing more than application of ice to the groin, neck, and axillae; and administration of 4o C IVF infused at 30cc/kg at 100ml/min via two peripheral catheters. Sedation or paralysis + intubation was used as per the norm.
Patients receiving this simple intervention were able to achieve goal temperature of 32o-34o C within 3-4 hours, and hypothermia was maintained for a full 24 hours before rewarming.
The study shows that expensive equipment and complicated protocols are not necessary for therapeutic hypothermia.
Involves an avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx.
Ring finger is most commonly involved.
Usually occurs from a grabbing attempt (resulting in forced DIP extension during maximal FDP contraction) as would occur while attempting to grab someone’s jersey such as in football or rugby.
Clinically, there is normal passive DIP ROM with loss of active flexion. Examine this by asking the patient to flex the fingertip at the DIP while the PIP joint is held in extension.
*Remember that patients with a 90% full-thickness tendon laceration may still have normal (albeit painful) range of motion. The examiner must evaluation the strength of the tendon against resistance. This injury is commonly missed as it is diagnosed as a “jammed” finger.
Plain films may show a bony avulsion, but are often negative.
Treatment is primary repair especially with large bony fragments. Partial ruptures can be treated nonoperatively at the discretion of the hand surgeon.
Hyponatremic seizures are a frightening entity. Anticonvulsants don't work well, and will likely cause apnea well before they halt the seizure. Hypertonic saline carries with it the fear of inducing central pontine myelinolysis (CPM) with overly rapid correction of the hyponatremia.
However:
So, you can safely correct hyponatremia rapidly in the setting of seizures. Do it like this:
Give 2-3 mL/kg of 3% NaCl in rapid sequential boluses, until seizures stop. A theoretical maximum dose is 100mL/kg, but recall that only a relatively small correction is required to stop the seizure.
After you've stopped the seizure, correct the hyponatremia slowly, as you would otherwise.
{kind=link}