Many changes in pulmonary physiology occur during pregnancy. These changes are generally well tolerated but can become problematic when pathologic states arise.
Here are a few examples of the normal changes and potential consequences:
Progesterone increases tidal volume and respiratory rate.
“Normally" a mild respiratory alkalosis pH 7.4-7.47, PaCO2 28-32, and bicarbonate 17-22 (renal compensation).
Low metabolic reserve with systemic illness.
Weight gain, anasarca, and breast size reduces chest wall elasticity.
Potential for restrictive physiology and reduced lung volumes.
Can be challenging to to mechanically ventilate due to decreased compliance and intra-thoracic pressure
Mechanical displacement of abdominal and thoracic contents by growing uterus.
Reduced lung volumes leading to reduced oxygen reserve and decreased apnea time.
Aim higher if placing chest tube (avoid abdominal contents)
Uterine pressure on stomach can increase aspiration risk and pulmonary injury.
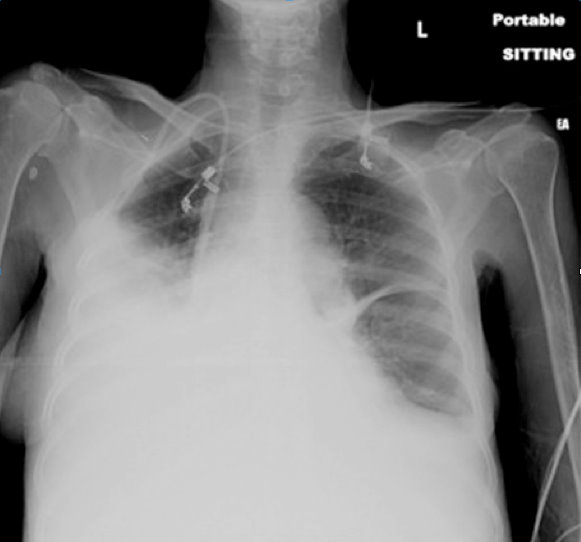
65 yo female with breast cancer presents with dyspnea and CXR shown below. Diagnosis? Can anything help clarify the diagnosis?
Elderly patients are prone to hypovolemia for the following two major reasons:
1. They have a decreased thirst response.
2. They have decreased renal vasopressin response to hypovolemia.
The result is that elderly patients have an impaired ability to compensate for a decreased cardiac output, which causes them to develop shock earlier and more easily with stressor.
Takeaway point: Always assume that most elderly patients are hypovolemic, and when they are stressed, give them fluids early!
Cubital Tunnel Syndrome aka Radial Tunnel Syndrome
Several medications/chemicals can cause unique toxicologic reactions in pediatric patients.
The onset of idiopathic seizures typically affects patients between ages 5 and 20.
Therefore, be highly suspicious of a diagnosable etiology in patients who present with new onset seizure prior to age 5 or after age 20.
Common causes of such seizures include:
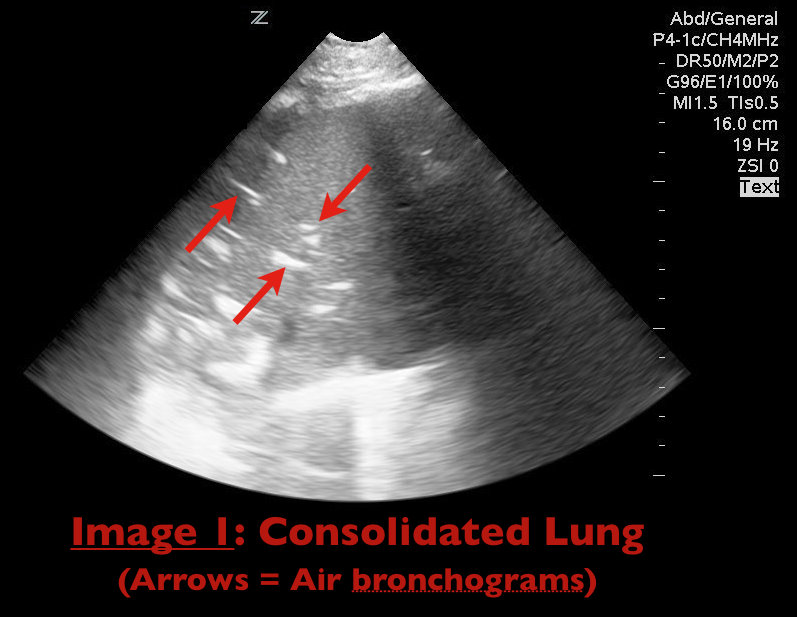
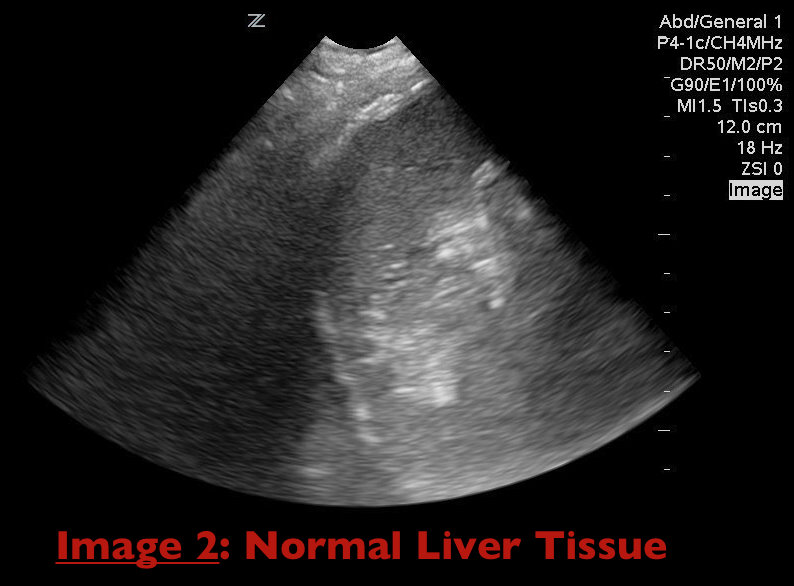
The Severely Hypoxemic ED Patient
Adverse drug effects are a major issue in geriatrics.
Elderly patients take, on average, 5 prescription medications + 2 over-the-counter medications.
Adverse drug effects account for approximately 5% of all hospital admissions.
Nearly 20% of patients brought to the ED for psychiatric complaints have symptoms that are primarily caused by medication effects.
Be very wary whenever prescribing ANY new medications for even a short time to elderly patients.
Sulfamethoxazole (SMX)/trimethoprim (TMP) is the treatment of choice for PCP pneumonia. The IV formulation has been unavailable for almost a year due to shortage. It is contraindicated in patients with sulfa allergy. Here are the alternatives with adverse effects. You'll quickly see why pentamidine should generally be reserved for those with sulfa allergy and G6PD deficiency.
Mild-to-moderate disease:
Moderate-to-severe disease:
Adverse Effects:
Now that influenza season is in full swing, remember that early antiviral treatment can reduce the risk of complications in high-risk individuals. One of those high-risk groups is children <2 years, with the highest hospitalizations and mortality in infants <6 months.
According to the CDC website:
Recommended antiviral medications (neuraminidase inhibitors) are not FDA-approved for treatment of children aged <1 year (oseltamivir) or those aged <7 years (zanamivir). Oseltamivir was used for treatment of 2009 pandemic influenza A (H1N1) virus infection in children aged <1 year under an Emergency Use Authorization, which expired on June 23, 2010. Nevertheless,
Current CDC guidance on treatment of influenza should be consulted; updated recommendations from CDC are available at http://www.cdc.gov/flu
.
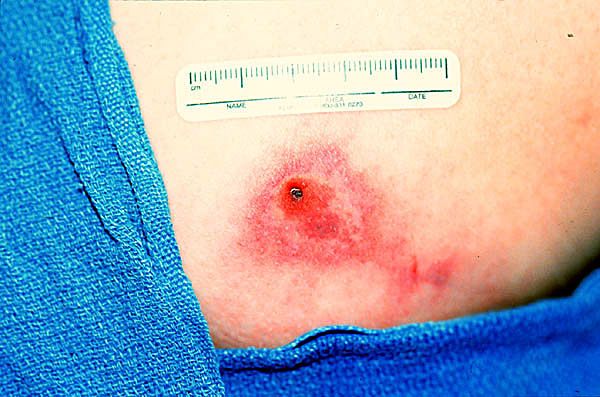
Recently a case report was published in which a child was incorrectly diagnosed with MRSA. He actually had systemic loxoscelism from a Brown Recluse spider bite.
A patient who has been bitten by brown recluse spider bite may present with pruritis, pain and swelling. The classic lesion has a bluish-purple central region, surrounded by concentric rings of pale ischemia and erythema. (“red, white and blue”) Bites may progress over days to a bleb with necrosis and eschar formation, followed by ulceration.
Systemic loxoscelism presents with a scarlatiniform rash that spreads dependently. It may have the classic purple lesion surrounded by concentric rings of pale ischemia and erythema. The patient may be uncomfortable but is usually stable. Treatment is supportive care.
24 yo woman presents with syncope, abdominal pain, and normal menses 4 days prior. Urine HCG(+) and quantitative beta-HCG is 1300 with the transvaginal ultrasound seen below. Diagnosis?

The long QT syndrome and causes of acquired long QT interval are well-known to most emergency physicians, but a short QT can be problematic as well. Short QT-syndrome is an inherited ion-channel disease that predisposes to ventricular dysrhythmias and sudden death. The QTc in these patients is generally < 340 msec. This condition is more common in children, and it should be considered in the differential diagnosis and evaluated on ECG in children presenting with syncope.
Sever's disease ,aka calcaneal apophysitis, is a common overuse injury in the pediatric and adolescent population.
Occurs secondary to traction of the calcaneus that most often occurs in young athletes (8-12 yo)
-Avg. age of presentation is 11 years 10 months in boys & 8 years 8 months in girls
-Repetitive traction to the weaker apophysis, induced by the pull of the Achilles on its insertion
Hx: Heel pain that increases with activity (running, jumping).
-May involve one (40%) or both (60%) feet
PE: Tenderness of the posterior heel at the Achilles tendon insertion and ankle dorsiflexor weakness
Imaging: Radiography is often normal. When positive, show fragmentation and sclerosis of the calcaneal apophsis. NOTE: These findings are nonspecific and also are observed in asymptomatic feet.
http://t0.gstatic.com/images?q=tbn:ANd9GcQ9R-fx1iyhbhNJpNL2W72bWdK72_mRBLNX5DUDtcMfnDli-x7Ong
DDx: Includes osteomyelitis and tarsal coalition.
Tx: Rest from aggravating activities, NSAIDs, ice (both pre and post sport). When pain free a program of stretching (gastrocnemius-soleus), strengthening (dorsiflexors) and shoe inserts (heel cups, lifts, pads, or orthotics) can provide significant pain relief.
Continuing with the synthetic/designer drug theme. Last time we were discussing synthetic marijuana. Another old drug making a resurgence under the designer drug category is mephedrone.This amphetamine-like drug has been purportedly the active substance in "bath salts". It has also been sold as "plant food" - still trying to figure that one out.
Sold in head shops under the name Bliss or Cloud 9 - they have been reported to be available in Baltimore, MD recently. They can also be bought over the internet. Crushed, snorted or ingested, the effect is similiar to cocaine with a largely sympathomimetic toxidrome. Mephedrone has been labeled an entactogen with users behaving similiar to an MDMA ingestion. A Baltimore news station incorrectly called it "synthetic cocaine" - though the effect may be similiar, completely different molecular structure.
Treatment is cooling, check lytes (especially sodium), check for rhabdomyolysis and sedation with benzodiazepines. Below is one link from a Denver News Station. Attached is a picture of a bath salt product.
The latest and greatest on the street - synthetic marijuana and bath salts!
http://www.thedenverchannel.com/news/26567376/detail.html
-- 6 to 12 months > "strongly consider" LP
-- 12 to 18 months > "consider" LP
-- 18 months and up > LP not routinely necessary; may consider after clinical assessment
-- Any infant/child with recent antibiotic treatment plus SFS > "strongly consider" LP
Hemodynamic Monitoring in the Ventilated Patient