So the magnesium didn't work, and the baby is on the way! You're prepared with everything you need for the delivery from bulb suction to a tripod for Dad's camera... But what is going to special about this baby?
Babies born to mothers who received magnesium therapy for any reason are at risk for hypotonia and severe respiratory depression.
· In the event a nuclear power plant accident, people may be exposed to a mixture of radioactive products. The main radionuclides representing health risk are radioactive caesium and radioactive iodine.
· Iodine-131 is concentrated in the thyroid gland and may eventually lead to development of thyroid nodules and thyroid cancer.
· Radioiodine uptake by the thyroid can be blocked by taking potassium iodide (KI) pills or solution, preventing these effects.
· KI should not be taken in the absence of a clear risk of exposure to a potentially dangerous level of radioactive iodine because KI can cause allergic reactions, skin rashes, salivary gland inflammation, hyperthyroidism or hypothyroidism.
· Since radioactive iodine decays rapidly, current estimates indicate there will not be a hazardous level of reaching the United States from this accident.
· There are three FDA approved KI products: Iosat, Thyrosafe and ThyroShield.
Hemorrhagic bullae in an ill-appearing patient with underlying cirrhosis should prompt consideration for an invasive infection due to Vibrio vulnificus.
V. Vulnificus is a gram negative rod and causes a highly lethal infection in patients with cirrhosis.
Antibiotics for these patients should include coverage for this organism. This should include doxycycline and a third genaration cephalosporin.
Severe hemolysis/hemolytic anemia in a patient with a prosthetic cardiac valve suggests a paravalvular leak. In this condition, a portion of the valve becomes dislodged from the valve annulus. It can occur immediately after surgery or delayed if from endocarditis. Paravalvular leaks are more common with mechanic valves. Patients may also present with sudden pulmonary edema.
The treatment will focus on management of the pulmonary edema and prompt surgical repair.
For patients with normal renal function, enoxaparin dosing for treatment of VTE is 1 mg/kg subcut every 12 hours OR 1.5 mg/kg subcut every 24 hours.
Studies have evaluated dosing for patients weighing up to 190 kg and found the 1 mg/kg q 12 hours dose to be safe and effective. It can even be used for patients heavier than 190 kg, but anti-Xa monitoring is recommended.
Extravasation from radiocontrast, phenytoin and promethazine have resulted in significant tissue necrosis sometimes requiring surgical debridement and reconstructive plastic surgery.
Pearl: Keep the infiltrated peripheral IV in and inject hyaluronidase 3-5mL (150U/mL) into the same subcutaneous pocket of medication. Hyaluronidase will increase the systemic absorption of the drug, decreasing its time in the SQ tissue. Extremely safe drug (we have the enzyme in our body) and has been used in neonates as well as adults. Also used for SQ hydration in palliative care and pediatrics.
Controversy: Hot vs Cold - Heat will cause vasodilation and hopefully increase systemic absorption but will likely also increase SQ spread possibly increasing the surface area of injury. Cold will cause vasoconstriction and decrease size of injury however will concentrate drug and possibly worsen the local injury.
Emergency Medicine physicians are gaining experience with non-invasive ventilation (i.e., Bi-level ventilation and continuous positive-pressure ventilation) in managing respiratory distress and failure. Although NIV is commonly used across a variety of pathologies, the best data exists for use with COPD exacerbation and cardiogenic pulmonary edema (CHF, not an acute MI)
Although other indications for NIV have been studied, the data is less robust (eg., smaller study size, weak control groups, etc.). If there are no contraindications, however, many experts still support a trial of NIV in the following populations:
Failure to clinically improve during a NIV trial should prompt invasive mechanical ventilation.
25 year old male presents after falling from 10 feet and landing on right shoulder. Diagnosis?

Aortocaval compression occurs often when gestational age is > 20 weeks. This compression significantly compromises the chances of maternal survival in cardiac arrest. Because it is often difficult to know the exact gestational age, it is commonly recommended that emergency C-section in maternal cardiac arrest be performed when the fundus extends above the level of the umbilicus.
GOUT part 1
Gout is an inflammatory arthritis that classically affects the first metatarsal phalangeal joint
Gout prefers cool ambient temperature hence gouty tophi prefer the great toe (one of the coldest parts of the body) and avoids "warmer" joints such as the hip and shoulder.
Remember that gout can affect other joints as well (elbow, wrist, knee and ankle) and can cause painful bursitis and tendonitis
Multiple joints can be involved simultaneously (leading to confusing with RA and OA)
The involved joint will often be red, hot, swollen and very painful leading to easy confusion with cellulitis and or a septic arthritis
Diagnose gout by demonstrating monosodium urate crystals in the synovial fluid.
**Remember previous pearl by Dr. Bond regarding the coexistence of gout with septic joint**
Serum uric acid levels are commonly elevated but can be normal or even low
Use caution with this test because asymptomatic hyperuricemia is much more common than gout
Note that yesterday's Neurology pearl should have read as follows -
Amongst others, diagnostic criteria for NMS includes:
Exposure to a dopamine ANTAGONIST (NOT AGONIST) or dopamine agonist withdrawal within past 72 hours.
Apologies for the type-o.
Could this be another risk factor for DVT/PE. Maybe not yet but it is worth mention. A recent observatioal study in BMJ showed that there was an associated increase with DVT or PE. From a database of 25,532 patients over a 3 year period of time and finding match controls, the results were:
Limitations were this is was an observational study with missing data. BMI was missing in these records and it is always difficult to tease out the multiple medications these patients are on. Also don't have a great biological mechanism (yet). Still makes you go hmm....
Antipsychotic drugs and risk of venous thromboembolism, Parker, BMJ, 2010.
- Exposure to dopamine agonist or dopamine agonist withdrawal within past 72 hours
- Hyperthermia
- Rigidity
- Mental status alteration
- Elevated creatinine phosphokinase
- Sympathetic nervous system lability (2 or more of the following: elevated blood pressure, fluctant blood pressure, urinary incontinence, diaphoresis)
- Tachycardia and tachypnea
- Negative work-up for infectious, metabolic, neurologic, or toxic etiologies.
Aspiration Pneumonitis and Pneumonia
Rib fractures are associated with significant morbidity and mortality in the elderly, and the risk increases dramatically with each successive rib fractured. An elderly patient with 3 rib fractures has a mortality of 20% and risk of pneumonia is 31%. As a general rule, you should really think twice about discharging home any elderly patients with rib fractures.
[credit to Dr. Joe Martinez for bringing forth this information]
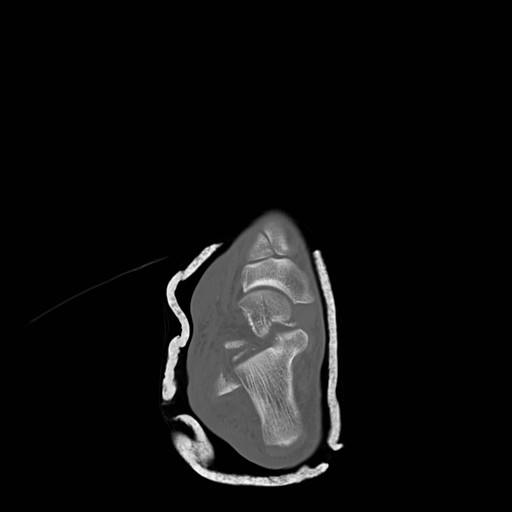
Talar Neck Fractures
Have a high rate of avascular necrosis (AVN), nonunion, and arthritis. Almost all require ORIF


Most have converted from succinylcholine to rocuronium for their choice of paralytic in RSI. Succinylcholine-induced hyperkalemia secondary to muscle fasciculations is considered usually clinically insignificant though there may be a hyperkalemic renal patient that this may tip them over. The fasciculations also may worsen traumatic long bone fractures. Here is the argument in a head to head comparison:
| Succinylcholine | Rocuronium | Winner | |
| Onset | 1-1.5min | 1.5-3min | Tie |
| Duration Recovery Index | 3-7min 2min
| 30-40min 10min | Mild S |
| Fasciculations | Yes | No | Roc |
| Histamine | Yes - Released | None | Roc |
| Pulse | Rare Brady | Rare Tachy at high dose | Tie |
Duration = injection of drug to 25% recovery of single twitch height (clinically relevant recovery in ED - essentially breathing may return)
Recovery Index = time from 25% to 75% recovery of single twitch height
The main reason succinylcholine was utilized was because of its fast onset and short duration. Rocuronium is comparable enough to succinylcholine in these characteristics tilting the overall benefits to rocuronium. If the FDA ever approves it, suggamadex is a possible reversal agent for rocuronium - currently used in Europe. Imagine having that in your RSI kit.
