Acute Poststreptococcal Glomerulonephritis (APSGN) is a sequela of group A beta-hemolytic streptococci (GAS) infection of the skin or pharynx with nephrogenic strains of GAS. Damage to the kidneys is due to deposition of antigen-antibody complexes in the glomeruli.
Presentation:
Testing:
Treatment:
Prognosis (favorable):
Reference:
Kit, Brian. Assess the volume status and electrolytes in children with poststreptococcal glomerulonephritis. Avoiding Common Pediatric Errors. 2008. p356-57.
The incidence of tendon rupture related to fluoroquinolone use is reported to be in the range of 1 in 6000.
The risk of tendon rupture associated with FQ use is increased in those older than 60 years of age, those taking steroids, and in patients who have received heart, renal, or pulmonary transplants.
There is no evidence that tendon rupture is more likely for patients taking levofloxacin compared to other FQs.
Blood Pressure in the Critically Ill Obese Patient
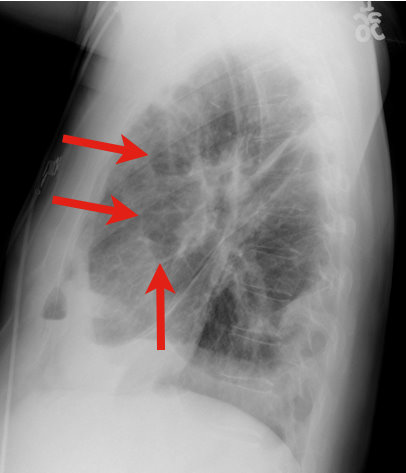
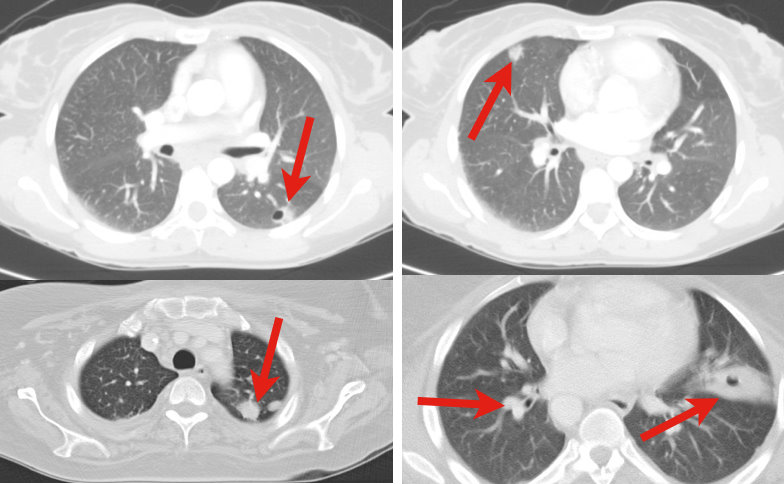
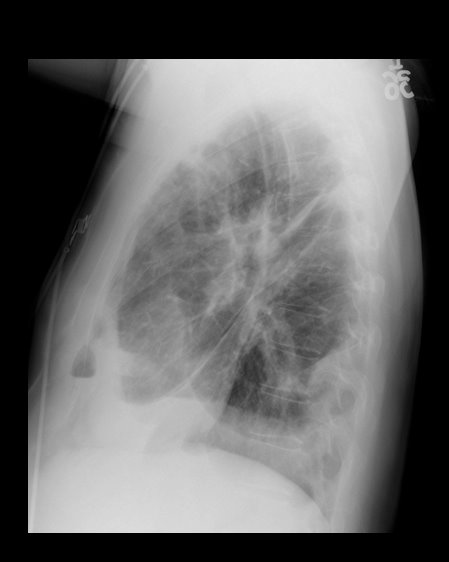
34 y.o. male with history of IVDA (intravenous drug abuse) complains of fever, chills and cough. Diagnosis?
Clues to RV infarction:
1. This almost always occurs in the presence of a concurrent inferior MI.
2. Clinical findings may include the triad of hypotension, JVD, and clear lungs.
3. ECG clues: in the presence of inferior lead ischemia or injury pattern, look for:
a. Combination of ST depression in lead V2 + ST elevation in lead V1; OR
b. Combination of ST depression in lead V2 + isoelectric ST segments in leads V1 and V3; OR
c. ST elevation in lead III markedly greater than the ST elevation in lead II; OR
d. ST elevation in right-sided leads (requires you to obtain right-sided leads)
Why is this diagnosis important?
1. It suggests a larger infarction and worse prognosis, so BE AGGRESSIVE in management.
2. Be very cautious with preload-reducing medications (e.g. nitrates) in the acute management of these patients, as they may induce significant reductions in blood pressure and extension of the infarction. Be aggressive with IVF, while maintaining close attention to the lung sounds.
Refractory Osteomyelitis is defined as a chronic osteomyelitis that persists or recurs after appropriate interventions have been performed or where acute osteomyelitis has not responded to surgery and antibiotics.
Case series, animal data and non-randomized prospective trials suggest that the addition of Hyperbaric Oxygen therapy to routine surgical and antibiotic management of previously refractory osteomyelitis is safe and improves the rate of infection resolution.
In patients with osteomyelitis involving spine, skull, sternum, HBOT is recommended prior to surgical intervention.
Typically patients require 20-40 daily dives for sustained therapeutic benefit.
How does HBOT work in osteomyelitis?
1. Restoration of normal to elevated O2 level in infected bone.
2. Leukocyte mediated killing of aerobic bacteria is restored when low O2 tension intrinsic to osteomyolitic bone is restored to physiologic or supra-physiologic levels.
3. HBOT is noted to exert direct suppressive effects on anaerobic infections.
4. HBOT augment the transport of certain abx (aminoglycosides and cephalosporins) across bacterial cell wall.
5. Enhance osteogenesis
6. Enhance angiogenesis
thank you to Dr. Sethuraman for this pearl
You're called to bedside to evaluate a "lethargic" infant. You wisely ask for a POCT glucose which returns at 35. How much dextrose do you give (since you know it's not just "an amp" of D50?
Here's a simple mnemonic:
Rule of 50-100 = multiply type of dextrose solution by ____ factor (ml/kg) to total 50-100
D10 (neonate) x 5-10 ml/kg = 50-100
D25 (infant) x 2-4 ml/kg = 50-100
D50 (child/adolescent) x 1-2 ml/kg = 50-100
There are increasing reports of bath salts which are crushed and then either injected, insufflated or taken orally. The actual substance has been found to be mephedrone as well as MDPV.(1) Both are amphetamine derivatives and the psychosis seen can appear like schizophrenia to the point that some of these patients have been admitted to the psychiatric wards. (2)(3) For those who have seen methamphetamine patients "tweaking" - where they use the drug for several days in a row without sleep - the presentation is quite similiar.
Synthetic drugs continue to present legal and regulatory problems since the compound is a "designer" synthesized drug that may not be on the DEA Schedule list. The product is labeled "Not for human consumption". Head shops and the internet remain primary sources of the drug. Bath salts present a serious and dangerous public health risk.
Heat stroke is hyperthermia (>41.6 Celsius / 106 Fahrenheit) plus neurologic findings (e.g., altered mental status, seizures, coma, etc.); it also causes systemic inflammation response syndrome (i.e., cytokine release), coagulation disorders (e.g., thrombosis in end organs) and tissue abnormalities (e.g., acute kidney injury and rhabdomyolysis)
Two classifications exist:
Treatment includes:
Despite the most aggressive therapy, up to 30% survivors may have permanent neurologic or multi-organ system dysfunction months to years after recovery
With recent national shortages of norepinephrine, our typical go-to drug in sepsis, it's become important for us all to familiarize ourselves with alternative pressors in this setting. Phenylephrine is a commonly chosen alternative.
Phenylephrine is a potent alpha-agonist associated with peripheral vasoconstriction. It has no beta effects so it is not associated with tachydysrhythmias. On the other hand, it is associated with reflex bradycardia which can be treated or prevented with atropine (although there are no specific recommendations to routinely administer atropine prophylactically). Phenylephrine may take 10 minutes to demonstrate an effect, and its duration is approximately 15 minutes. It should be used cautiously in patients with underlying cardiac disease because of the vasoconstrictive effect, and it should be avoided in patients with narrow-angle closure glaucoma.
Extravasation can cause tissue necrosis and should be treated with phentolamine.
C. Diff Colitis
The general treatment recommendations for C. Diff Colitis are to place the patient on PO metronidazole and if they fail this treatment PO vancomycin (125 mg 4x day). Vancomycin is generally reserved for resistant cases due to the fear that it could induce Vancomycin resistant enterococcus.
For severally ill patients it is recommended that you prescribe IV metronidazole and PO vancomycin when they are not actively vomiting. Remember there is no role for IV vancomycin as it does not get into the bowel lumen to eradicate the infection.
There is some great news though, the FDA recently approved a new drug, a macrolide antibiotic fidaxomicin (Dificid), for the treatment of C. Diff Colitis. Fidaxomicin was found to be as effective as vancomycin in preventing recurrence 3 weeks after treatment. Currently it is recommended that fidaxomicin be reserved for cases where patients are having recurrences after 3 weeks of vancomycin treatment.
The FDA news release can be found at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm257024.htm
Now that summer is in full swing, the question is: Should the evaluation of the febrile young infant change during the summer and fall months? And can that affect length of hospitalization and antibiotic use?
Two retrospective cohort studies from the Children’s Hospital of Philadelphia (CHOP) suggest yes! The addition of enterovirus polymerase chain reaction (PCR) testing to cerebrospinal fluid (CSF) may improve the care of infants with fever during enterovirus season (early June through late October).
Of note, at CHOP: 1) infants 56 days or younger routinely undergo lumbar puncture during evaluation for fever. 2) Most CSF enterovirus PCR test results (90%) were available within 36 hours; 95% of results were available within 48 hours.
In the King study, having positive enterovirus PCR CSF results decreased the length of hospitalization and the duration of antibiotic use for young infants less than 90 days, supporting the routine use of this test during periods of peak enterovirus season. In multivariate
analysis, a positive CSF enterovirus PCR result was associated with a 1.54-day decrease in the length of stay and a 33.7% shorter duration of antibiotic use.
Bottom line: Consider adding enterovirus PCR testing to CSF obtained during the evaluation of febrile young infants during enterovirus season, as this may reduce length of hospitalization and duration of antibiotic use. The effects, however, may be limited at institutions with slower lab turnaround times.
References:
1) King RL, Lorch SA, Cohen DM, Hodinka RL, Cohn KA, Shah SS. Routine cerebrospinal fluid enterovirus polymerase chain reaction testing reduces hospitalization and antibiotic use for infants 90 days or younger. Pediatrics. 2007 Sep;120(3):489-96. http://pediatrics.aappublications.org/content/120/3/489.full.pdf
2) Dewan M, Zorc JJ, Hodinka RL, Shah SS. Cerebrospinal fluid enterovirus testing in infants 56 days or younger. Arch Pediatr Adolesc Med. 2010 Sep;164(9):824-30.
Levamisole is an antihelminthic agent used in humans to treat certain parasitic infections and cancers. It is more commonly used for veterinary purposes. It has recently seen increasing use as a cutting agent for cocaine and heroin, found in up to 70% of cocaine sample seized by the DEA. It adds bulk and weight to powdered cocaine and is even theorized to increase the stimulant effects.
Toxicity of levamisole includes agranulocytosis and vasculitis (see attached document for recent image from NEJM).
Trivia: Levamisole was found in DJ AM and Andrew Koppel (Ted Koppel’s son), who both died of drug overdoses.
(1) immunomodulatory therapy for the underlying immune disorder, often with high dose
intravenous (IV) steroids which speeds recovery, and
(2) management of symptoms through supportive measures and amelioration of risk factors
associated with precipitating acute exacerbations such as infection through aggressive use
of antibiotics. Treatment of fever with antipyretics also key as even small increases in
temperature can significantly affect conduction through partially demyelinated fibers.
Hemodynamic Optimization in the Post-Arrest Patient
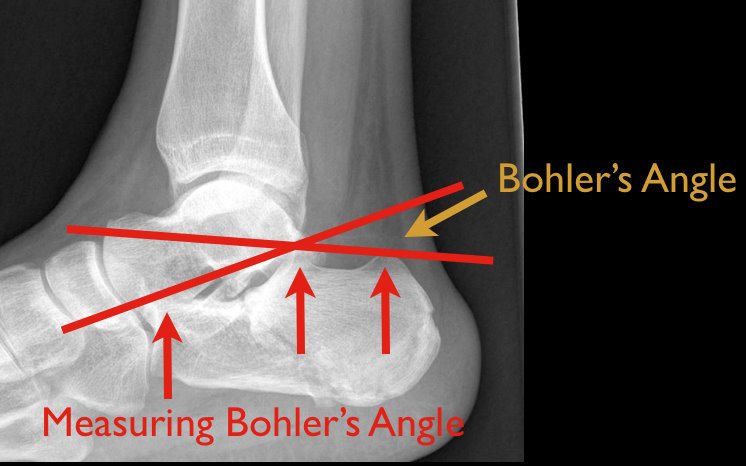
48 year old male following 15 foot fall onto both feet. What is the diagnosis?
…and why is it called the “Lover’s Fracture”?

There has been some controversy regarding the actual clinical benefit of non-invasive ventilation (NIV) for patients with cardiogenic pulmonary edema in recent years. However a recent Cochrane review has confirmed the benefit of NIV for these patients. Early (ED) use of NIV is associated with a decrease in both intubation rates and mortality. The NNT to prevent one intubation is 8, and the NNT to prevent one hospital mortality is 13. To put this in perspective, the NNT for NIV to prevent death in patients with cardiogenic pulmonary edema is lower than the NNT for thrombolytics to prevent death in acute MI.
One key point to remember is that it MUST be used early! If you wait until your patient is decompensating, it is often too late. Start the NIV as soon as possible in these patients.
Emergency physicians are often called upon to provide event coverage for marathons.
Prolonged endurance racing is safe for the majority of participants.
Hyponatremia (8.2% - 13.5%) - finishing times of greater than 4 hours is an independent risk factor
Hypokalemia – uncommon
Renal function – BUN > 30 or Cr > 1.4 mg/dL (23.6%). There is no data that this is of any clinical significance.
Cardiac Troponin - (11%) had significant increases (troponin T > or = 0.075 ng/mL or troponin I > or = 0.5 ng/mL). Elevations were more commonly seen with weight loss and increased Cr levels and may be associated with running inexperience (< 5 previous marathons) and young age (< 30 years) though interestingly not with race duration or traditional cardiac risk factors.
Findings are similar for men and women