Pediatric forearm fractures:
The Crashing Patient with PAH
Metaphyseal bucket handle and corner fractures are almost pathognomonic for child abuse
These injuries were originally identified by clinicians evaluating children with subdural hematomas
These injuries are typically seen in the ankles, knees, elbows and wrists
Violent twisting, shaking, or pulling across a joint creates shearing forces across the weak epiphyseal growth plate and metaphysis
This leads to
1) A thin rim of mineralized metaphyseal bone aka “bucket handle”
http://rad.usuhs.mil/rad/home/peds/bucketarrow.jpg
OR
2) Small flecks of bone from the metaphyseal corner adherent to periosteum
http://t2.gstatic.com/images?q=tbn:ANd9GcT0kZ3VR1f7MwRj7oIa6jaYVp_-f8kZ1NhSbw4kCTRGNLDJ1pKK9g
A recent study highlighted the challenges we face managing ED patients on warfarin therapy. Some key observations about how we're doing:
Literature continues to show warfarin is the most dangerous medication for our patients. Meticulous monitoring and follow up will help us potentially avoid serious interactions and adverse events.
-- occurs during or immediately following urination, often when bladder is full.
-- occurs at night or after standing from the recumbent position of a deep sleep to urinate.
-- risk factors: enlarged prostate, alpha blocker therapy, dehydration, alcohol, fatigue.
Up until recently, a tight-fitting mask was one of the only ways to deliver non-invasive positive-pressure ventilation.
High-flow nasal cannulas (HFNC) have been adapted from use in neonates to adults to deliver continuous positive airway pressure (CPAP).
HFNC provides continuous, high-flow (up to 60 liters), and humidified-oxygen via nasal cannula providing positive pressure to the pharynx and hypopharynx. Patients tolerate it well and it is less claustrophobic than tight-fitting masks.
HFNC does not generate the same amount of pressure as CPAP so it may be best utilized as an intermediate step between low-flow oxygen (i.e., traditional nasal cannula) and non-invasive positive pressure ventilation with tight-fitting masks.
Check with your respiratory department if these devices are locally available.
Minimizing interruptions in chest compressions during CPR is critically important. As an example of the adverse consequences of interruptions, consider the following finding from Edelson (Resuscitation 2010): for every 10 seconds of hands-off time during cardiac arrest, the patient's chances of successful return of spontaneous circulation decreases by 50% due to reductions in cerebral perfusion.
Next time you are involved in a code, keep this in mind, and do EVERYTHING POSSIBLE to minimize those interruptions in chest compressions.
You just finished assessing a 6 month old in the Pediatric ED who can’t move his right leg. You suspect child abuse. You’re ready to order labs, a head CT, ophtho consult, skeletal survey and call Child Protective Services. While your doing all of this, your medical student asks you, “What exactly are you looking for on the skeletal survey?”
A skeletal survey is mandatory for cases of suspected child abuse in children under the age of 2 years. Approximately 60% of the fractures seen in abused children are younger than 18 months old.
When you are looking at a skeletal survey, carefully look for the following:
1. Multiple, healing fractures of various ages
2. Rib fractures, especially in the posterior ribs
3. Metaphyseal chip and buckle fractures
4. Spiral fractures in long bones (especially in children that can’t walk)
5. Skull fractures which are not simple and linear
6. Scapula fractures
More to come about child abuse….
A recent article estimated 100,000 emergency hospitalizations for adverse drug events in U.S. adults 65 years of age or older each year. Nearly half of these hospitalizations were among adults ≥80 years old and two-thirds were due to unintentional overdoses.
Four medications or medication classes were implicated alone or in combination in 67% of hospitalizations:
Opioids were #5. Digoxin was #7 and resulted in the highest percentage of hospitalizations per ED visit at 80%.
High dose insulin is recommended in treatment of beta-blocker and calcium channel blocker overdose. In a recent observational case series of cardiogenic shock, high dose insulin was evaluated for efficacy and safety.
Hypotension in the PAH Patient
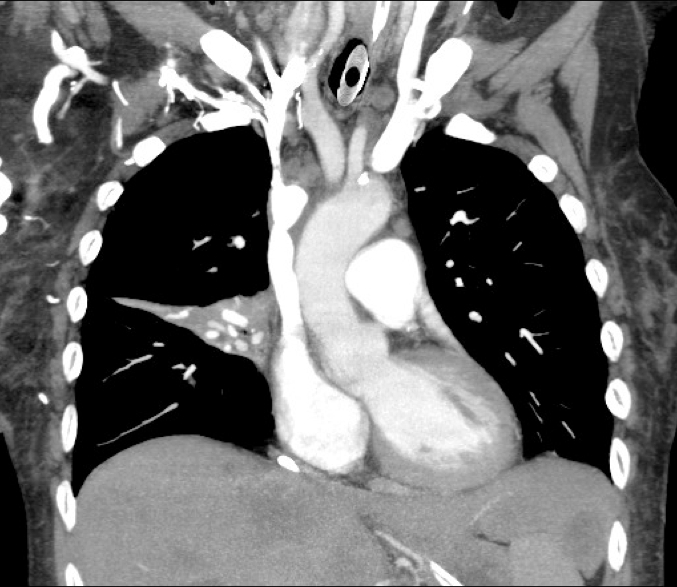
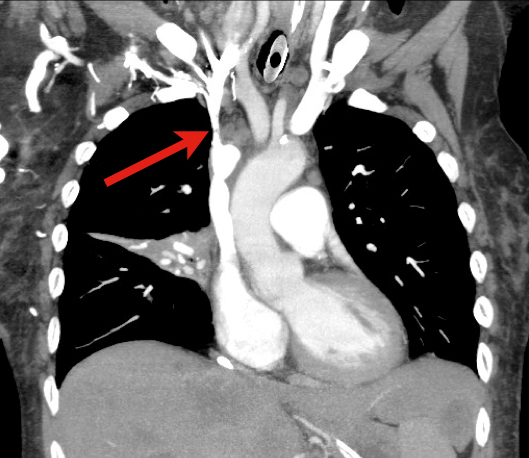
9 year-old boy with sudden onset of unilateral facial swelling. What’s the diagnosis?

Right heart endocarditis is much more common in patients that are injection drug users. Fortunately for them, they have a lower mortality than patients with left heart endocarditis because they have a lower rate of developing heart failure. This is a reminder that the most common cause of death from endocarditis is heart failure.
The Weber classification system
A commonly used, simple, easily remembered system used to describe ankle fractures. The system focuses on the integrity of the syndesmosis.
http://www.accessemergencymedicine.com/loadBinary.aspx?fileName=simo_c017f013t.gif
- TYPE A: fibula fracture below the ankle joint/syndesmosis (which is intact). Deltoid ligament intact. Medial malleolus can be fractured. Usually treated with closed reduction.
http://www.gentili.net/image1.asp?ID=-241442344&imgid=AnkleWeberAAP600.jpg&Fx=Weber+A+Fracture
- TYPE B: is a transsyndesmotic fracture with usually partial rupture of the syndesmosis (though may be intact). No gross widening to the tib/fib articulation.. Deltoid ligament intact. Medial malleolus often fractured. Variable stability. Any clinical or radiographic injury to the medial joint complex make this an unstable fracture
http://www.gentili.net/image.asp?ID=145&imgid=AnkleWeberBmortise600.jpg&Fx=Weber+B+Fracture
- TYPE C: Fibular fracture above the level of the syndesmosis with usually a total rupture of the syndesmosis (seen as widening of the distal tib/fin articulation), resulting in instability of the ankle mortise. Associated with medial malleolus fracture or deltoid ligament injury. Unstable.
http://www.gentili.net/image1.asp?ID=146&imgid=anklewebcapoblx2600.jpg&Fx=Weber+C+Fracture
Classic Kawasaki is diagnosed by fever for greater than 5 days plus 4 out of 5 classic signs.
But what about an 8 month-old with 6 days of fever plus nonexudative conjunctivitis, unilateral cervical adenopathy and a diffuse maculopapular rash? Send some labs!
Incomplete Kawasaki is defined as fever for >5 days with 2 or more of the classic findings plus elevated ESR (>40mm/hr) and CRP (>3.0mg/dL). It is most common in infants under 12 months of age.
Disposition for the 8 month-old?
If the echo is normal, follow up in 24-48 hours and will need a repeat echo if fever persists.
TREAT kids with IVIG and aspirin (which generally means admission) if echo is positive, or with normal echo and the presence of 3 or more supplemental criteria: