68 yo man presents with new-onset seizures; his CT is shown below. What is your differential diagnosis?
Here's some numbers to consider regarding typical radiation exposre associated with cardiac imaging tests relative to naturally occurring background radiation exposure:
Test type Relative exposure
Naturally occurring annual background radiation
exposure for a person living in the US (~ 3 mSv) 1
Coronary artery calcium score 0.5
Cardiac CT angiography 1-4
Nuclear stress test (single-photon emission CT) 3-4
Exercise treadmiil testing (with no imaging) 0
Cardiac MRI/echocardiogram 0
[above estimates are typical, but may vary between individuals and among different centers]
Luxatio erecta, aka inferior shoulder dislocation, is an uncommon form of shoulder dislocation (0.5-2%)
2 Mechanisms: 1) Forceful, direct axial loading of an ABducted arm.
2) Hyperabduction of the arm leads to impingement of the humeral head against the acromion, If forceful enough, this leverage can rupture the capsule and drive the humeral head downward, resulting in an inferior dislocation. This mechanism is more common.
Classic presentation: Arm locked in marked ABduction with the flexed forearm lying above the head.
http://uconnemig.files.wordpress.com/2011/11/emimages-8c.jpg
http://img.medscape.com/pi/features/slideshow-slide/sdrt/fig1.jpg
http://www.mypacs.net/repos/mpv3_repo/viz/full/76563/3828172.jpg
One may palpate the humeral head against the lateral chest wall
Bony injuries include fractures to surrounding structures such as the coracoid process, acromion, glenoid rim, clavicle, greater tuberosity and humeral head.
Nerve injuries include damage to the brachial plexus/axillary nerve (usually reversed with reduction)
Vascular injuries: Axillary artery thrombosis
Submersion injuries are the 2nd leading cause of accidental death in children with 1/3 of survivors sustaining significant neurologic sequelae. 50% of drownings occur from May to August.
40% of all drowning victims are children under age 4, with males affected 3 times as often as females. Most drownings occur with 10 feet of safety. Infants and toddlers drown most often in bathtubs (especially if <1 year old), buckets, toilets, pools and hot tubs (most often the pools are in-ground). Those with seizure disorders have a 10-14 fold higher likelihood of drowning.
Aspiration of as little as 1-3ml/kg of fluid may cause pulmonary edema, surfactant inactivation or washout, pulmonary shunting with resulting V/Q mismatching, or direct injury to the alveolar membrane.
Immediate and adequate resuscitation, including intubation, is the single most important factor determining survival. Always check body temperature as hypothermia is common. In general, prophylactic antibiotics and steroids are not indicated unless drowning occurred in grossly contaminated water/sewage.
Dexmedetomidine is an alpha2-agonist that has a similiar mechanism of action to clonidine. Short half-life and no respiratory depression make it possibly more effective than propofol in procedural sedation. Cost/Availability are the biggest barriers. Transient bradycardia is also possible but the actual incidence of clinically significant bradycardia is not yet elucidated.
I am still awaiting the first emergency department study looking at dexmedetomidine for procedural sedation.
A recent article actually brought up the possibility of utilizing it intranasally which could have some tantalizing pediatric applications.
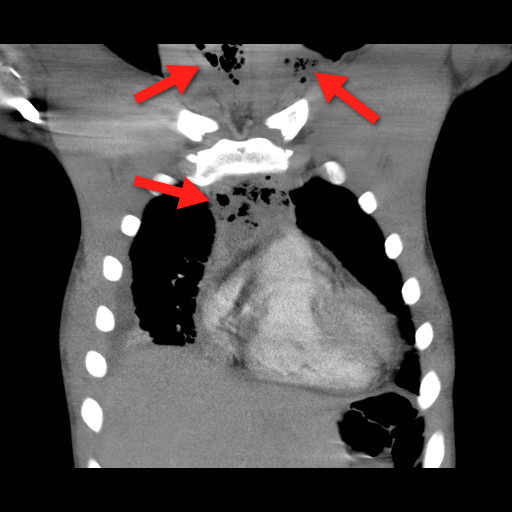
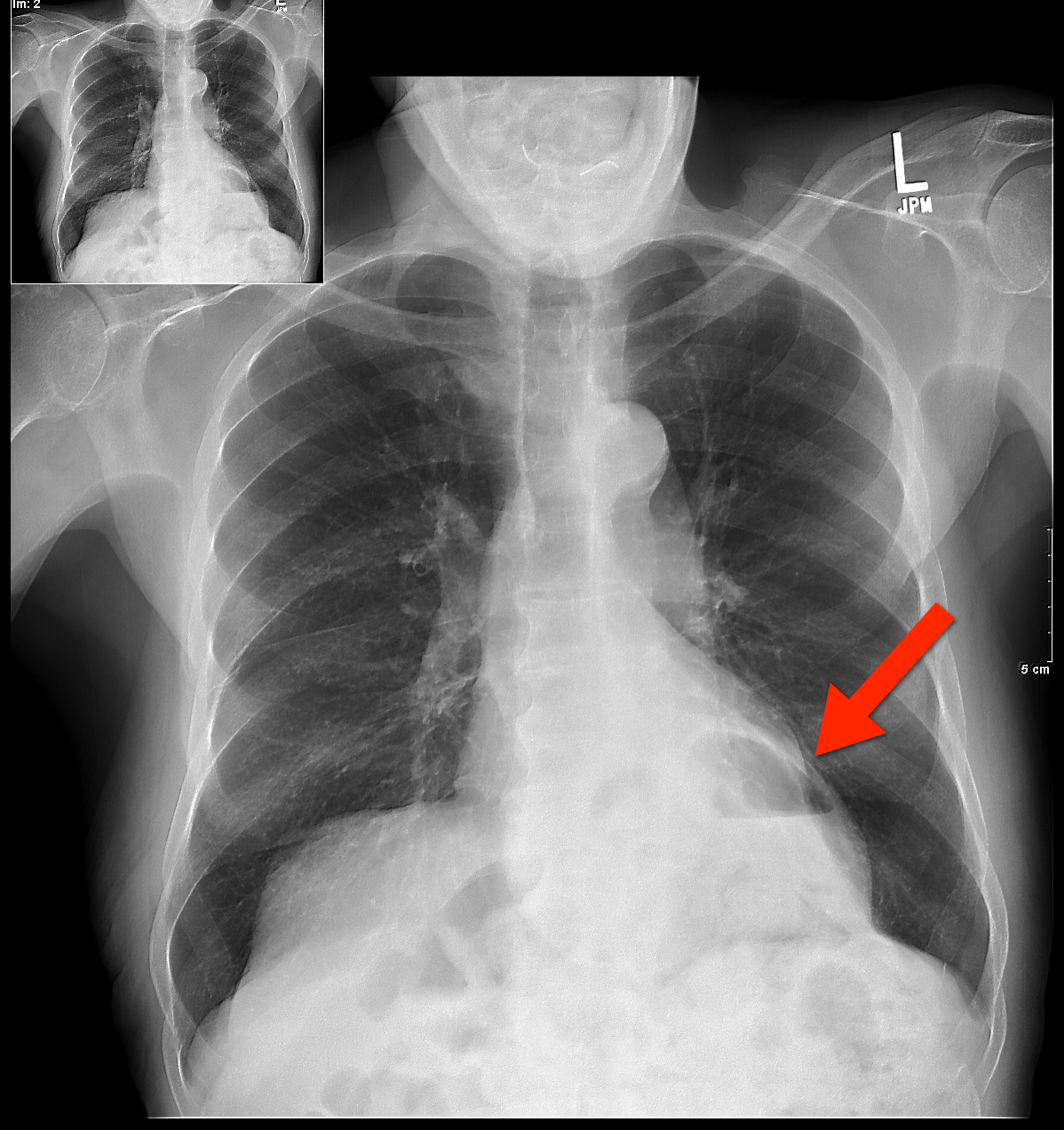
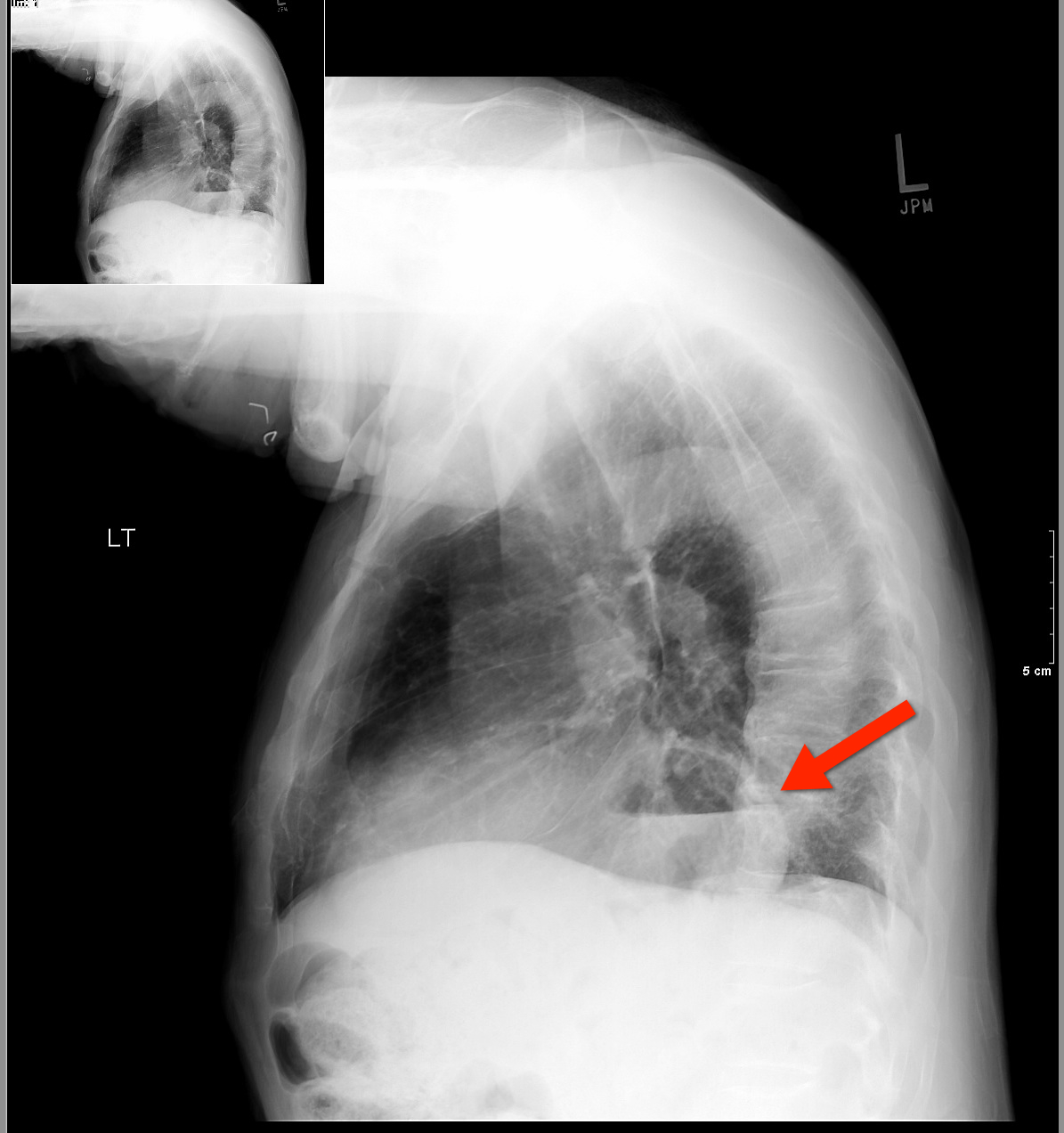
Mediastinitis is an infection of the mediastinum; a rapidly fatal surgical emergency if not recognized and treated early.
Causes include esophageal perforation, oropharyngeal infections (e.g., Ludwig’s angina), prevertebral or carotid space infections, and iatrogenically (endoscopy, hypopharyngeal perforations during intubation, etc.).
Plain films (neck / chest) may serve as a screening tool, but CT best defines the source and extent of disease; the CT below demonstrates gas within the soft-tissues and the mediastinum (red arrrows).
Infections may be polymicrobial and broad-spectrum antibiotics with anaerobic coverage (e.g., pipercillin-tazobacam) should be started initially.
Immediate treatment should also include:
Bonus Pearl
Can't keep up with all the great educational stuff in Emergency Medicine and Critical Care? Let the professionals at Life in the Fastlane do it for you (http://lifeinthefastlane.com). These guys scour the web and blog about the best educational pearls, podcasts, and radoiolgic finds...and they're also quite the laugh. Check them out today!
[Pearl provided by Dr. Semhar Tewelde]
Who are the experts at deciphering ECG's
Authors looked at 240 ECGs which activated the cath lab activation for STEMI. They excluded patients with LBBB or paced rhythms. Retrospective chart reviews were used to determine if there was actually a STEMI. The ECGs were then shown to 7 experienced interventional cardiologists and interpreted for acute STEMI.
Of 84 subjects, there were 40 patients with a true STEMI and 44 without (13 of whom had NSTEMI) Recommendations for immediate PCI varied widely, from 33%-75%. Sensitivities were 53%-83%, specificities 32%-86%, PPV 52%-79%, and NPV 67%-79%. When the cardiologist chose non-ischemic ST elevation, LVH was thought to be the cause in 6% to 31% and old MI/aneurysm in 10% to 26%.
Moral, even cardiologists can be wrong... EM physicians must scrutinize every ECG and challenge ourselves to be the best at interpreting ECG's.
Some quick board review pearls. Remember these fractures/dislocations and the neurologic injury that is associated with them
Children are at higher risk for complications related to the transfusion of blood products compared with adults. So when should we consider transfusion?
Normal hemoglobin values:
- highest at birth (14 - 24 g/dL),
- decreasing to 8 to 14 g/dL at 3 months,
- increasing to 10 to 14 g/dL at age 6 months to 6 years, 11 to 16 g/dL at age 7 to 12 years, and 11.5 to 18 g/dL in adulthood.
- Although the number of platelets are in the normal range at birth, their function is impaired.
For infants younger than 4 months, thresholds for red blood cell transfusions:
- hemoglobin levels are 12 g/dL for preterm infants or term infants born anemic,
- 11 g/dL for chronic oxygen dependency,
- 12 to 14 g/dL for severe pulmonary disease,
- 7 g/dL for late anemia in a stable infant,
- 12 g/dL for acute blood loss exceeding 10% of estimated blood volume.
For infants older than 4 months, thresholds for red blood cell transfusions:
- hemoglobin levels are 7 g/dL in a stable infant,
- 7 to 8 g/dL in a critically unwell infant or child,
- 8 g/dL in an infant or child with perioperative bleeding,
- 9 g/dL in an infant or child with cyanotic congenital heart disease (increased oxygen demand).
- 9 g/dl in children with thalassemia major (to slow bone marrow stimulation)
For children with sickle cell disease (SCD):
- threshold is 7 to 9 g/dL, or more than 9 g/dL if the child has previously had a stroke.
- perioperatively for major surgery: 9 to 11 g/dL, and sickle hemoglobin should be less than 30%, or less than 20% for thoracic or neurosurgery.
Bottom line:
A threshold of 7 g/dL is indicated for the transfusion of packed red blood cells in most children.
Reference:
1) Transfusion guidelines in children. Anasethesia and Intensive Care Medicine. 2012;13(1);20–23.
2) Medscape clinical education briefs
Cuff Pressures and the Prevention of VAP
67 yo male presents with burning substernal chest pain; worse with meals and when supine. What's the diagnosis?
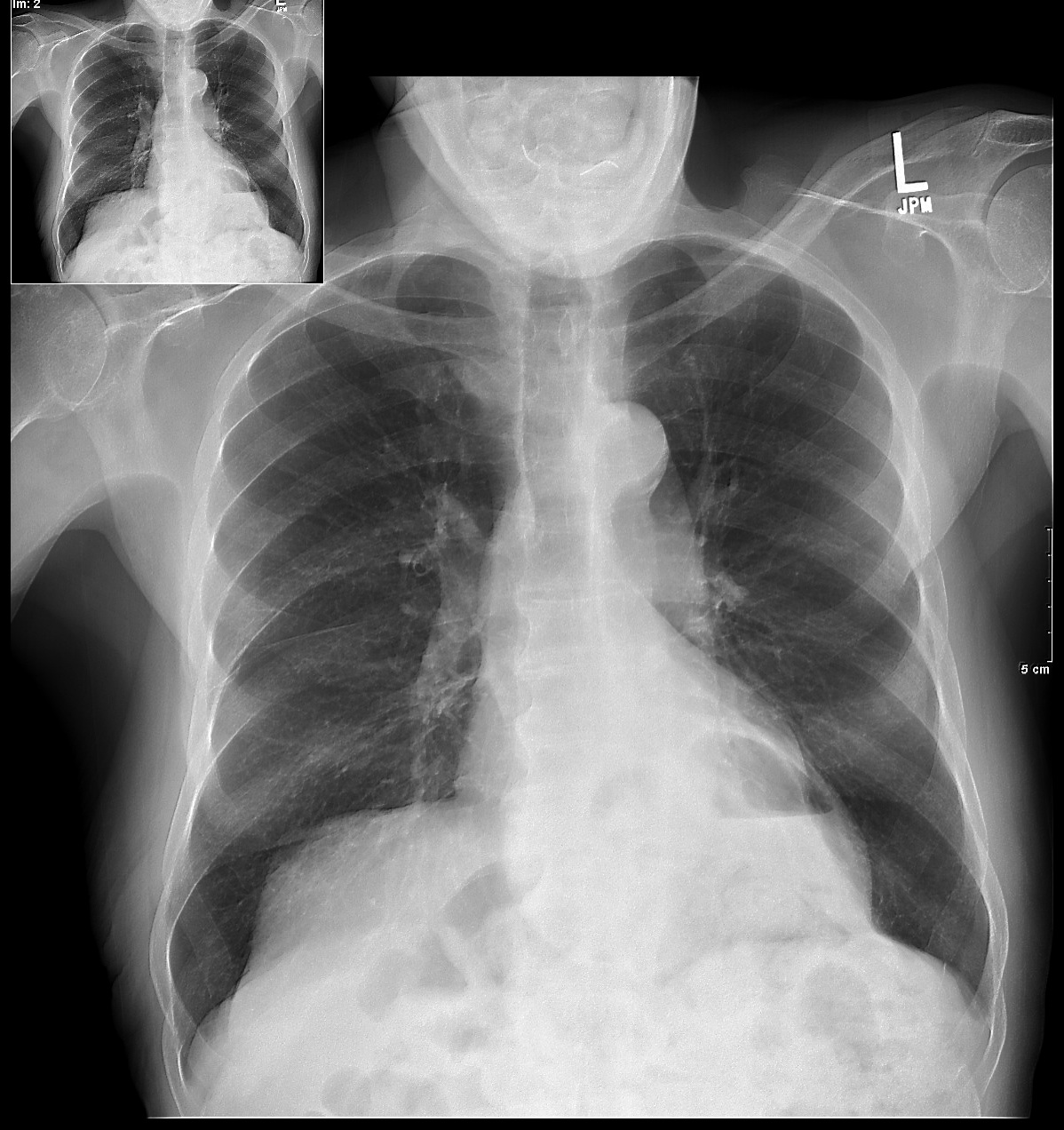
(from Dr. Semhar Tewelde)
Stress testing is one modality used to screen for CAD. The goal is to identify a fixed obstruction to coronary blood flow (typically plaque > 50%) such as in stable angina. However, in ACS, both USA and AMI, the underlying pathophysiology is plaque rupture (typically plaque < 50%) and thrombus formation that may not have been significant enough to cause a positive stress test.
The use of a prior negative stress test to determine the disposition of ED chest pain patients is questionable. The history of present illness should dictate patient disposition. In one study 20.7% of patients presenting to the ED with a negative stress test within three years of presentation still had significant CAD defined as a positive cardiac markers, subsequent positive stress test of any type, cardiac catheterization requiring intervention, or death due to medical cardiac arrest within 30 days of ED presentation.
Chronic exertional compartment syndrome (CECS)
An overuse injury common in young endurance athletes
In athletes with lower leg pain, CECS was found to be the cause in 13.9% - 33%.
*This is likely under diagnosed as most recreation athletes will discontinue or modify their activity level at early symptom onset
Common in runners and most often involves the anterior compartment
Occurs due to increased pressure within the fascial compartments, primarily in the lower leg
Symptoms are bilateral 85 - 95% of the time
Exercise increases blood flow to leg muscles which expand against tight surrounding noncompliant fascia. This, in turn, increases compartment pressures and eventually reduces blood flow which leads to ischemic pain. Pain usually begins within minutes of starting exercise and experienced athletes can often pinpoint the time/distance required for symptom onset.
Symptoms are primarily pain (tightness, cramping, squeezing) but may also include paresthesias and numbness. Symptoms gradually abate with cessation of activity.
Diagnosis: Although some physicians’ make a clinical diagnosis based on Hx and exam, definitive diagnosis requires measurement of compartment pressures both at rest and post exercise.
Nonsurgical treatment: activity modification and rest
Surgical treatment: >80% success with anterior and lateral compartments vs. 50% with deep posterior compartment.
Over the last few decades, the rate of breastfeeding has increased steadily in the developed countries of the world. During this time, opioid use in the general population has steadily increased as well. Despite this, clinicians remain unclear whether opioid use is safe during breastfeeding.

Sepsis is one of the top 10 causes of death in the U.S. and its incidence is on the rise.
The financial burden of sepsis is also growing; it is estimated that between 2000 and 2005 the overall cost of ICU hospitalization rose from $56.6 billion to $81.7 billion per year with severe sepsis accounting for $16.7 billion.
Although we may not be able to immediately modify the incidence of community-acquired sepsis, hospital-acquired sepsis can be reduced; for example, many cases of nosocomial sepsis are associated with catheter blood stream infections secondary to central-lines.
There are several simple strategies to prevent catheter-related blood-stream infections:
Remember: We play a large role in reducing nosocomial sepsis; be vigilant about your sterile techniques during central catheter insertions and question the need for every single line.
Bonus pearl (only for iPhone): MDRNTools is a FREE app (that’s right, FREE!) with lots of ED and ICU applications such as an IV med calculator, an RSI handbook, a Stroke Scale calculator, and more.
Download http://itunes.apple.com/us/app/mdrntools/id505794224?mt=8&ls=1

Well, here is a cool little app that has recently been released. It's an app that can predict what a child's height will be as a mature adult. This is not a joke.
A free mobile application developed by the International Center for Limb Lengthening (ICLL) at the Rubin Institute for Advanced Orthopedics (RIAO) of Sinai Hospital (right in our very own Baltimore) can predict the future mature height and bone lengths of children with the input of basic information.
That's right people. The formula has amazing accuracy and has been studied in many different centers. It's supposedly 97%+ accurate in predicting height.
The Multiplier App, available for Android, iPhone and iPad devices, is based upon the Multiplier Method, a series of formulas used to calculate and predict height and bone length in children. These formulas were developed by a team that included members of the ICLL.
Here is what it looks like. Just click on "Height" (see enclosed jpg image of the app) and then type in the child's birthday and current height in either inches or cm. The formula will then calculate what there predicted height will be.
Very, very cool ( at least I think)
(Pearl provided by Dr. Semhar Tewelde)
Physiological LV hypertrophy in trained athletes is defined by an isolated increase in QRS amplitude, normal axis, normal atrial and ventricular activations patterns, and normal ST-segment T-wave replorization; athletes of African/Caribbean descent have prominent cardiovascular remodeling leading to pronounced voltage criteria for LV hypertrophy and BER
Despite the presence of voltage criteria for LVH, pure QRS voltage criteria for LVH in an asymptomatic athlete without family hx of cardiovascular diseases or SCD, and lack of non-voltage ECG criteria does not warrant systematic evaluation with echocardiography.
In other words, young patients, especially men, especially those of African/Caribbean descent, will be expected to have large voltage QRS complexes and sometimes abnormal repolarization, and this is not necessarily a pathologic finding.
Exertional leg pain in the athlete carries a wide range of possible etiologies. In a recent review article, etiologies included, stress fracture (25%), exertional compartment syndrome (33%), medial tibial stress syndrome (13%), nerve entrapment (10%), and popliteal artery entrapment syndrome.
Medial Tibial Stress Syndrome (MTSS) is also known as shin splints. It is a repetitive-stress overuse injury.
Risk factors include: hyperpronation, higher BMI, increased hip internal rotation, and hyperplantar flexion.
While MTSS may be on a stress reaction spectrum that includes fracture, the causes are likely to also include tendinopathy and muscle dysfunction (tibialis anterior, posterior and soleus).
Radiographs will be normal with this condition. MRI and bone scan may show signal abnormality along the posterior medial tibial surface.
Treatment: In most cases participation in sports may continue. Also consider, rest/activity modification, ice, NSAIDs, physical therapy for calf stretching and strengthening, and rigid orthotics (to correct foot hyperpronation). Semi rigid and neoprene orthotics may be considered for prevention in those with a prior history.
In a recent multicenter, double-blind, randomized, non-inferiority trial, vancomycin was compared to fidaxomixin for Clostridium difficile infection.
Location: 45 sites in Europe and 41 sites in the USA and Canada
Patients: Age 16 years or older with acute toxin-positive C difficile infection.
Treatment: Oral fidaxomicin (200 mg every 12 h) or oral vancomycin (125 mg every 6 h) for 10 days.
Endpoint: Clinical cure, defined as resolution of diarrhea and no further need for treatment.
Results: 198 (91.7%) of 216 patients in the per-protocol population given fidaxomicin achieved clinical cure, compared with 213 (90.6%) of 235 given vancomycin (one-sided 97·5% CI -4·3%). Occurrence of treatment-emergent adverse events did not differ between groups.
Author conclusions: Fidaxomicin could be an alternative treatment for infection with C difficile, with similar efficacy and safety to vancomycin.
Funding: Optimer Pharmaceuticals.
{kind=link}
{kind=link}
{kind=link}