It is likely that during ones career in Emergency Medicine, one will be faced with how to work up a child presenting to the ER following exposure to common house electrical current. The older recommendations were such that all children exposed, received a screening EKG and were admitted to telemetry for monitoring. However, a relatively recent article in the Annals of Emergency Medicine suggests otherwise.
In fact, after reviewing several studies the authors conclude that, although there is not enough literature to support evidence based practice “guidelines”, there appears to enough evidence to support that practice of “safely discharging these children without an initial EKG evaluation or inpatient cardiac monitoring after a common household current exposure.” This includes both 120V and 220 V exposures.
Clearly, some patients may require work up and/or admission based on other injuries or clinical presentation.
References:
Chen E H, Sareen A, Do Children Require ECG Evaluation and Inpatient Telemetry After Household Electrical Exposures? Ann Emerg Med. 2007;49:64-67.
Protamine for enoxaparin overdose
Transferring Multidrug-Resistant Organisms
Pearl provided by Dr. Semhar Tewelde
The Athlete's Heart and ECG Abnormalities
Up to 80% of athletes have common training related ECG changes/abnormalities including: sinus bradycardia, asymptomatic sinus pause, sinus arrhythmia, first degree AV block, incomplete right bundle branch block, benign early repolarization (BER), and isolated QRS voltage criteria for left ventricular (LV) hypertrophy.
Approximately 5% athletes exhibit uncommon training unrelated ECG changes/abnormalities including: T-wave inversions, ST-depression, pathological Q-waves, left axis deviation/left anterior fasicular block, right axis deviation/left posterior fasicular block, right ventricular hypertrophy, complete left or right bundle branch block, long or short QT interval, ventricular pre-excitation/WPW, Brugada pattern, and arrhythmogenic right ventricular dysplasia (ARVD).
Animal studies can pave the way for new clinical treatment modalities. In the setting of lung injury due to smoke inhalation, one of the problems (if you can get the ET tube in) are the elevated ventilatory pressures due to the massive edema. In this sheep model of smoke inhalation, nebulized epinephrine improved ventilatory pressures, PaO2/FiO2 ratio and pulmonary shunting.
We may have these sheep to thank for this new treatment.
The supine position during rapid sequence intubation may result in posterior lung atelectasis thereby reducing lung volumes, oxygenation reserve, and ultimately apnea time.
Several studies have shown that elevating the head of the bed by at least 20 degrees or placing a patient in reverse Trendelenberg position (for patients with contra-indications to elevating the head of the bed) during RSI may significantly increase apnea time.
Elevating the head of the bed may be especially helpful for patients with BMIs >35
26 year old male with pain when he extends his 4th finger as well as swelling of that digit. Diagnosis?

Cardiogenic shock pearls from Dr. Semhar Tewelde:
1. CS is most commonly secondary to a large MI where > 40% of the myocardium is involved; however mechanical, valvular, dysrhythmogenic, and infectious etiologies should also be considered: papillary or chordal dysfunction, free wall or septal defects disease, insuffiency of any valve, myopericarditis, endocarditis, Tako-tsubo, end stage cardiomyopathy, and tamponade.
2. Incidence of 5-10% STEMI and 2.5-5% NSTEMI
3. Mortality ~50%
4. Immediate coronary reperfusion is the best treatment (NNT 8). Medical therapy is a distant second choice in management, with reperfusion and pressors as needed. Early intra-aortic balloon pump use is key.
5. Recent case reports have shown imporved outcomes when induced hypothermia was used in patients refractory to traditional therapy with pressors/inotropes/IABP.
A recent study looked at the risk of sudden cardiac death during a marathon.
Many isolated reports of sudden death make headlines in the national news.
However, of nearly 11 million runners, only 59 went into cardiac arrest during a race. This equates to an incidence rate of 0.54 per 100,000 participants,
This rate appears to be on par with sudden death from other athletic endeavors such as triathlons and college athletics.
Median age was 42. Men affected more than women (men also more likely to die from the event).
71% of events were fatal.
Further, risk is greater for both cardiac arrest and sudden death for full marathons than half marathons.
Interestingly, older patients fared better (increased survival in those >40yo), thought to be due to an increased incidence of hypertrophic cardiomyopathy in younger aged runners.
Patellar dislocations:
References:
1. http://emedicine.medscape.com/article/90068-overview
2. New England Musculoskeletal Institute. http://nemsi.uchc.edu/clinical_services/orthopaedic/knee/patellar_dislocation.html
High-Frequency Oscillatory Ventilation for ARDS?
Every heard of the Khan Academy website? If you have, you will instantly recogize what a powerful force this website has become in education. If you haven't, what are you waiting for? Head to http://www.khanacademy.org/ and check it out! This site gets millions of hit PER DAY.
The Khan Academy was developed by, guess who, a guy named Kahn, Salman Kahn. This website is amazing. My kids use it for some of their school work. Trust me, check it out. If you want to know just how good this guy is...check out the size of the check Bill Gates wrote him.
What does this have to do with medical education? The videos put together by Khan utilize a teaching modality called a "whiteboard." This type of teaching technology is changing they way educators deliver material. Programs like Doceri (www.doceri.com) utilize this concept. You can build presentations and teaching materials with audio included.
My pearl for you today is really more of an assignment...go to the two websites and check them out. First, visit the Khan Academy site and then the Doceri site. THIS kind of thing is the future of education...

How likely is coronary artery disease to occur in young patients?
An autopsy series in US communities evaluated young patients (avg age 36 years old) who died of "non-natural" causes revealed coronary atherosclerosis in > 80% of the autopsy sample, with 8% having significant obstructive disease.
The bottom line is simple....be wary of discounting the risk of ACS purely based on a patient's age. The HPI is the most important factor in predicting ACS.
Rashes that include palms/ soles
- Hand-Foot-Mouth Disease
- Kawasaki
- Erythema multiforme/ Stevens Johnson's Syndrome/ Toxic Epidermal Necrolysis
- Rocky Mountain Spotted Fever
- Scabies
- Syphillis
Rashes that have +Nikolsky's sign
- Scalded Skin Syndrome
- TEN
- Pemphigus Vulgaris
Rashes that desquamate
- Scalded Skin Syndrome
- Toxic Shock Syndrome
- Scarlet Fever
- Kawasaki
- TEN
Coumadin Wannabe's - have indication non-valvular atrial fibrillation
1) Dabigatran (Pradaxa)
2) Rivaroxaban (Xarelto)
Clopidogrel Wannabe's - both are antiplatelets
1) Ticagrelor (Brilinta)
2) Prasugrel (Effient)
If you were looking for the first case reports of lethal hemorrhage due to pradaxa that could not be reversed - look no further. One patient fall from standing dies from ICH and another death in a spine trauma patient on pradaxa. I am waiting for the first epidural hematoma due to pradaxa, xarelto, etc in ED. Watch out! :
1: Garber ST, Sivakumar W, Schmidt RH. Neurosurgical complications of direct thrombin inhibitors-catastrophic hemorrhage after mild traumatic brain injury in a patient receiving dabigatran. J Neurosurg. 2012 Mar 6. 2: Truumees E, Gaudu T, Dieterichs C, Geck M, Stokes J. Epidural Hematoma & Intra-operative Hemorrhage in a Spine Trauma Patient on Pradaxa® [Dabigatran]. Spine (Phila Pa 1976). 2012 Feb 16.
Pre-oxygenation prior to rapid sequence intubation (RSI) is performed to prevent hypoxemia during endotracheal intubation.
An appropriate period of pre-oxygenation will potentially increase the amount of apnea time during intubation, however patients with certain critical illnesses (e.g., severe pneumonia) may desaturate faster than expected.
Apnea time can be increased by maintaining high-flow oxygen by nasal cannula (e.g., 15L), during application of the bag-valve mask and during the time of attempted endotracheal tube placement; this concept is known as apneic oxygenation.
Apneic oxygenation is based on the principle that when patients are apneic, alveoli absorb oxygen into the blood stream at a rate of approximately 250 mL/minute, creating a diffusion gradient from the pharynx (containing a high-density of oxygen from the nasal cannula) to a lower concentration of oxygen in the alveoli.
Although a patient’s oxygenation can be maintained longer using apneic oxygenation, its application does not remove the continuous buildup of CO2 in the alveoli during apena. Therefore, respiratory acidosis can result after a prolonged period of apneic oxygenation.
The complete article describing the physiology and practical applications can be found here....it's free! http://www.annemergmed.com/article/S0196-0644(11)01667-2/fulltext
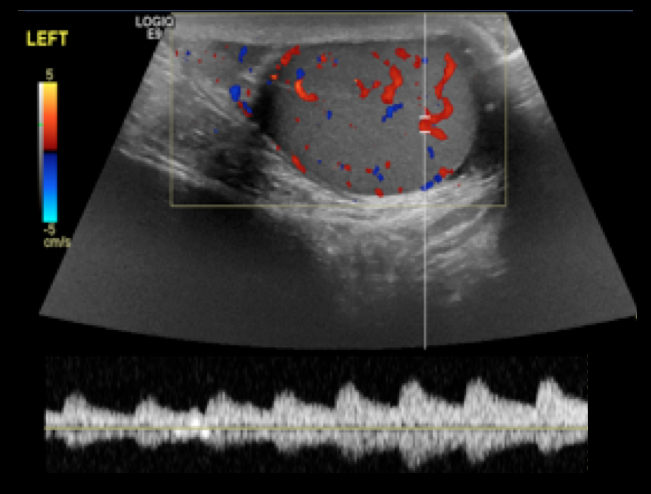
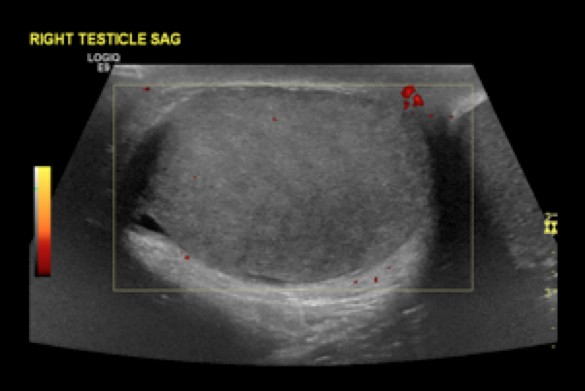
14 year-old male presents with right-sided testicular pain. What's the diagnosis?
A recent study in JAMA has provided further evidence regarding some key issues in ACS/MI presentations which seem to be commonly taught but often forgotten in actual practice. Here's just a few of the key findings from this study:
1. Generally speaking, women were more likely to present without chest pain than men, and the difference between the sexes was most apparent in the < 45yo groups. Overall, 42% of women presented with painless MIs. [remember from a recent prior cardiology pearl that painless MIs have a higher mortality as well]
2. Women had a higher mortality than men within the same age groups, and the difference between the sexes was most apparent in younger ages.
3. Almost 1/5 of women < 45 yo with MI did not report chest pain. [We've always assumed it's just the older women that present with painless MIs....not true!]
A final point that should be re-stated: young women DO have MIs, they DO often present without pain, and they DO often die. Be wary.
The plantar fascia arises from the medial tuberosity of the calcaneous and extends to the proximal phalanges of the toes.
Pkantar Fasciitis is the most common cause of heel pain in adults.
Etiology is thought to be from a degenerative tear at the fascial origin followed by a tendinosis type reaction and .
Affects women 2x> men
More common in overweight patients.
Onset is insidious and not related to trauma.
Hx: Pain and tenderness directly over the medial calcaneal tuberosity and 1-2cm distally along the plantar fascia.
Pain is worse with prolonged standing/walking. Pain is most intense however when rising from a resting position such as first thing in the morning.
PE: Pain is increased with passive dorsiflexion of the toes. Tenderness to palaption over the medial calcaneal tuberosity and 1-2cm distally along the plantar fascia.(At times, one may have to apply increased pressure to approximate weight bearing type stress)
XR: Usually not necessary with a good history and exam. Heel spurs are seen in up to 50% with the disease (and in up to 20% without it!)
DDx: Tarsal tunnel syndrome. Calcaneal stress fracture. Fat pad atrophy. traumatic rupture of planter fascia.