Methotrexate is a chemotherapeutic that is utilized in non-Hodgkin lymphoma and breast CA. It is also used as an immunosuppressant for rheumatoid arthritis and psoriasis. Finally, we see it used in the ED for the treatment of ectopic pregnancy. Overdose, often unintentional, can have a lethal outcome.
Toxicity: LFTs rise, N/V, stomatitis, mucositis, leukopenia, thrombocytopenia, renal failure
Antidote: Leukovorin (Folinic Acid)
Other Tx: Carboxypeptidase G2, Charcoal Hemoperfusion, HD (possible)
- Mask-like face
- Eyelid weakness
-- leads to ptosis
-- exacerbated by sustained upward gaze
-- improved by closing the eyes for a short while
- Extraocular motion abnormality
-- usually affects more than one extraocular muscle
-- may be assymetrical
-- may result in mild proptosis
- Weak palatal muscles
-- nasal-sounding voice
-- nasal regurgitation of food
- Weak jaw muscles
- Absent gag reflex
- Pupils normal
On October 25, 2011, Eli Lilly announced a voluntary-recall of activated drotrecogin alfa (Xigris) following a recent trial (PROWESS-SHOCK), which demonstrated no survival benefit when using the drug when compared to placebo.
Activated drotrecogin alfa is a recombinant form of human activated protein C previously recommended for adults with severe sepsis and a high-risk of death (APACHE II > 25 or multi-organ failure); it is included in the 2008 International Sepsis Guidelines (Grade 2b recommendation).
The PROWESS-SHOCK trial reported an all-cause mortality rate of 26.4% in the drotrecogin alfa group compared with 24.2% in the placebo group; this difference was not statistically significant.
Interestingly, the study also found that severe bleeding (the drug's main side-effect) was found to be 1.2% in the activated drotrecogin alfa group compared to 1.0% for the placebo group (also non-significant) suggesting it does not increase the risk of bleeding as it had previously been reported.
Hospitals should revise their sepsis guidelines based on this recent news.
Weird and Unusual Symptoms
Bet you didn't know that severe and intense pruritus of the nostrils, known as Wartenberg's symptom, is an uncommon but characteristic symptom of a brain tumor.
Etiologies include astrocytoma, glioblastoma, oligodendroglioma, medulloblastoma, and metastatic tumors.
"Women experience higher mortality rates and more adverse outcomes after acute MI than men, despite less obstructive CAD and plaque burden."(1)
How can this be explained? It turns out that women have more frequent coronary remodeling of vessels. "Remodeling" refers to the concept that as plaques grow, they tend grow into the vessel wall causing outward bulging of the wall, rather than growing into the vessel lumen. That means that standard coronary angiography and even stress testing often miss significant lesions because they only evaluate lumen obstruction....which is not directly reflective of plaque size/burden.
The net effect of the above is that women are more likely to have false negative stress tests and angiograms that appear to show non-significant occlusions. Until we have reliable tests that evaluate true plaque burden rather than just vessel occlusion, we can't completely rely on stress testing and angiography to rule out the the presence of significant plaques.
The TFCC (triangular fibrocartilage complex) is a ligamentous/cartilage like complex similar to the meniscus of the knee located on the ulnar side of the wrist.
http://yanyanxu.com/wp-content/uploads/2008/01/trifibcc.gif
Hx: ulnar sided wrist pain following trauma and associated with activity related mechanical symptoms such as clicking.
PE: tenderness to palpation distal to ulnar head or at ulnar styloid . Tenderness against resisted radial deviation.
Plain film may show ulnar styloid avulsion or injury to carpal structures.
Refer to hand/wrist surgeon
Splint in ulnar gutter of long arm spica
MRI or arthrogram are studies of choice.
http://www.cobalthealth.co.uk/MImageGen.ashx?image=%2Fmedia%2F12951%2Fwrist-tfcc-tear-big.jpg&width=170&crop=true

Carbon Monoxide Toxicity and Hyperbaric Oxygen Treatment
CO disrupts cellular function by several mechanisms at a
cellular/mitochondrial level. Ultimately, these disruptions are
manifested as tissue hypoxia and hypoperfusion.
Initial symptoms may be subtle and nonspecific. Be sure to ask about
CO exposure when evaluating “viral syndrome” or patients that present
with non-specific neurological complaints especially during fall and
winter months, when people first start using their heating, or after
power outages and generator use. Dysrhythmias, cardiomopathy, MI and
sudden cardiac arrest are reported in severe CO poisoning.
Lab studies- COHb, base excess, lactate and any other studies based on
presentation.
Supplemental oxygen is the cornerstone of treatment. Oxygen
delivered at hyperbaric pressure (as opposed to sea-level) will
increase the rate of CO dissociation from hemoglobin, and mitigate
damage to cellular and mitochondrial function.
Definite Indications for HBOT: Current evidence supports the use for
HBOT to reduce cognitive sequelae in CO poisoned patients who have:
LOC , seizure, exposure >23 hours, COHb of 25% or more, and age >36.
Relative Indications: persistent symptoms after 100% O2 or change in
mental status, pregnancy, persistent cardiac ischemia, increased COHb
levels.
Disposition: Clinical judgment should guide your decision. Most
patients with mild symptoms can be discharged after treatment. If
patient has a more concerning presentation with several risk factors
(extremes of age, CAD, unconscious at arrival in the ED, etc…)
consider admission.
Differentiating Central Retinal Artery vs. Vein Occlusion Fundoscopically
SAH and Electrolyte Disorders
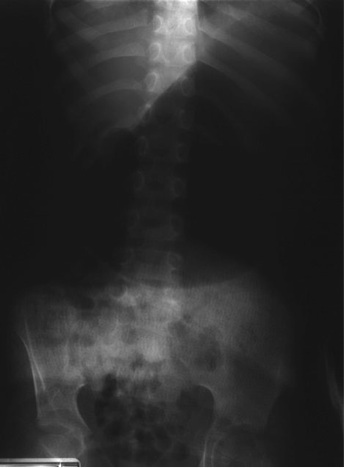
5 year-old male with developmental delay presents with intractable non-bloody and non-bilious vomiting over 10 days; bowel movements are normal. Four weeks ago he was placed in a hip-spica cast following a motor vehicle crash. Abdominal x-ray is below. Diagnosis?
Elevated BNP levels are found in conditions besides acutely decompensated CHF. These conditions can include:
Older age
Renal failure
Severe sepsis
PE
Chronic CHF
These conditions will often produce BNP elevations in an intermediate range, but if the elevation is markedly positive, the acutely decompensated CHF is much more likely.
[adapted from ACEP speaker Matthew Strehlow, MD]
Sinus Tarsi Syndrome
Lisiteria Monocytogenes is typically transmitted from ingestion of contaminated food such as unpasteurized milk or cheese, raw foods, and recently cantaloupes; transmission from veterinary exposure, infected soil and water have also been reported.
Listeria has a predilection for the central nervous system (CNS) causing several infections including meningioencephalitits, brain or spinal abscess, cerebritis (infection of brain parenchyma), and rhomboencephalitis (encephalitis of the brainstem).
Risk factors include immunosuppression, advanced age, newborns, and pregnancy.
There is no clinical way to distinguish CNS infection with Listeria from other pathogens, therefore blood and cerebrospinal fluid (CSF) culture is required.
CSF analysis demonstrates pleocytosis, elevated protein, and low glucose. CSF gram stain has a low sensitivity (~33%), but consider Listeria in the differential if "diptheroid-like" bacteria are reported on gram stain.
Ampicillin is the drug of choice and should be continued for at least three weeks (sometimes longer). Adding gentamycin is sometimes recommended for synergy in severe infection.
ST depression in the right precordial leads can be anteroseptal ischemia, but it can also be a posterior STEMI. What are the clues to posterior STEMI?
Posterior leads (a couple of leads placed in the left mid-back area below the tip of the scapula) can help confirm posterior STEMI if there's STE in those leads. If there's no STE, call it just ischemia!
Anterolateral dislocation is most common (>85%)
As the tib/fib joint has its own synovial cavity, a knee effusion will not be seen
Mechanism: fall on the flexed knee with foot/ankle inversion
Hx: swelling, variable amount of lateral knee pain (anywhere from mild discomfort to inability to bear weight)
PE: Prominence of the fibular head, ankle motion exacerbates knee pain. no associated neurovascular issues
However with less common dislocations (posterior and superior) peroneal nerve injury may occur
Reduction: Place patient supine with knee flexed to 90 degrees. Ankle should be dorsiflexed and externally rotated.
REVERSE THE INJURY: Apply firm posteriorly directed pressure to the fibular head. May head an audible pop as fibular head reduces. Reassess collateral ligament function.
Peritoneal dialysis (PD) is a commonly used form of dialysis for pediatric patients with end-stage renal disease, particularly in children less than five years of age.
One well known complication to this mode of dialysis is PD-associated peritonitis.
Children may present with fever, abdominal pain and a cloudy dialysate.
If peritonitis is suspected, obtain sample of dialysate fluid and send for cell count, Gram’s stain and culture.
Cell count in PD-associated peritonitis is usually WBC >100 with >50% neutrophils.
Both gram-positive and gram-negative organisms are involved with PD-associated peritonitis . Keep both MRSA and Pseudomonas in mind.
In the ED, empiric therapy should cover both gram-positive and gram-negative organisms. Initiate antibiotic therapy with vancomycin and either a third-generation cephalosporin (ceftazidime) or aminoglycoside, respectively.
For PD-associated peritonitis, intraperitoneal (IP) administration of antibiotics is preferred over IV.
There are an increasing number of intranasal medications commercially available for use, which is opportune as more and more intravenous medications become scarce.
These now include:
| Generic name | Brand Name | Usage |
| Fentanyl | Instanyl | Opiate analgesic |
| Ketorolac | Sprix | NSAID analgesic |
| Desmopressin (DDAVP) | Stimate | Bleeding |
| Vitamin B12 | Nasobal | Anti-migraine (yes!) |
| Sumatriptan | Imitrex | Anti-migraine |
| Zolmitripran | Zomig | Anti-migraine |
*******In addition, you can administer glucagon, midazolam and narcan intranasally as well.