If you have a patient who meets (or has had close exposure to someone meeting) the clinical case definition of pertussis (a cough lasting at least 2 weeks with one of the following: paroxysms of coughing, inspiratory “whoop,” or post-tussive vomiting) here are some important points to keep in mind:
Vaccination
Testing
Treatment
References:
Altunaiji SM, Kukuruzovic RH, Curtis NC, Massie J. Antibiotics for whooping cough (pertussis). Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD004404. DOI: 10.1002/14651858.CD004404.pub3
http://www.cdc.gov/vaccines/pubs/surv-manual/chpt10-pertussis.html
Femoral venous access is typically limited to the acute resuscitation of critically-ill patients. Several practice-guidelines recommend avoiding the femoral site, or removal once admitted to the ICU, because of the risk of catheter-related bloodstream infection (CRBI) and deep-vein thrombosis (DVT).
A recent systematic review and meta-analysis (including two randomized-control trials and eight cohort-studies) evaluated the risk of CRBI and DVT for catheters placed in either the internal jugular, subclavian, or femoral-venous sites. No difference in the rate of CRBI or DVT was found between the three sites, although the DVT data was less robust (i.e., contained heterogeneous data).
The authors hypothesized that improvements in sterility during central-line placement (e.g., full-barrier precautions), improved nursing care (e.g., central-line site care), and ultrasound guidance may have led to a reduction in femoral site complications.
Although a prospective randomized-control trial is necessary to confirm these results, this meta-analysis challenges the traditional teaching that femoral central-access should be avoided.
Placement of central-lines through the subclavian (SC) route has several advantages over other sites of venous cannulation:
• Lower rates of infection
• Lower rates of deep vein thrombosis
Placing a central-line through the "blind" SC approach increases the risk of non-compressible vessel injury and pneumothorax as compared to other approaches (e.g. internal jugular).
Ultrasound can help place central-lines in the SC vein while reducing the risk of complications; this video demonstrates the technique: http://ultrarounds.com/Ultrarounds/Subclavian_Ultrasound.html
Hypertrophic cardiomyopathy (HCM) is characterized by left ventricular hypertrophy (typically asymmetric) that occurs in the absence of pressure overload or storage/infiltrative disease.
HCM demonstrates remarkable diversity in disease course, age of onset, pattern and extent of LVH, degree of obstruction, and risk for sudden cardiac death.
Patients with HCM are at increased risk for sudden death, annual rate of SCD is ~1%. ICDs are recommended for all patients with prior arrest/sustained ventricular tachycardia (class I recommendation).
Apologies for the long pearl, I did not want to split this into 3 parts)
Disruptions in sleep and circadian rhythms (from travel across time zones and jet lag) are known to alter cognitive functions. Mood and complex mental performance tasks deteriorate faster than do simpler mental performance tasks.
An athlete’s circadian rhythms are believed to be optimal for performance in the early evening (reaction time to light and sound in the fastest). Interestingly, the evening is the time of day when most world records have been broken. However, activities that require fine motor control and accuracy (hand steadiness and balance) are best in the morning.
In the normal population, travel effects are seen in inattention and an increase in errors and injuries in the workplace.
Athletes who perform in international competitions immediately after time zone transitions demonstrate a decline in performance involving complex mental activities, with an associated feeling of lethargy and a general loss of motivation.
British Olympic athletes demonstrated a decrease in leg and back strength in addition to reaction time when traveling westward across 4 time zones. In the NFL, west coast teams consistently beat east coast teams in evening games.
Of course, this type of outcome data is multifactorial and travel effects likely are only one of many complex factors.
Treatment:
Full adaptation to the new time zone is NOT recommended for short trips (1 – 2 days), only for longer stays (> 3 days).
Nonpharmacologic:
Preadaptation and bright light therapy: Remember that exposure to light is the primary cue for circadian rhythms. Bright light exposure in the mornings (after eastward travel) will advance the body clock, while exposure in the evenings (after westward travel) will delay it (Level B).
Shifting the sleep schedule 1 - 2 hours towards the destination time zone in the days preceding departure may shorten the duration of jet lag (Level B).
Strategic napping: Napping in the new time zone during typical sleep times in the destination time zone will delay adaptation. Power naps (20 minutes) may be helpful in decreasing daytime sleepiness in those with jet lag (Level B). The best time to nap (in flight or post flight) is nighttime in the destination time zone (Level B).
Pharmacologic:
Melatonin: Cochrane review concludes that it is safe and effective in both treating and preventing jet lag. It is recommended for adults traveling across 5 or more times zones; and may be effective for travel across 2 to 4 time zones. Take melatonin in the morning when traveling westward, and at the local bedtime when traveling eastward (Level B). Doses of 0.5 to 5mg were similarly effective. Melatonin taken in the evening and at higher doses are effective at inducing sleep (Level A).
Sleep aids: Hypnotic sleep aids reliably induce insomnia secondary to jet lag. Benzodiazepines improve sleep quality but may cause a “hangover” effect the next day, possibly impairing performance.
Ambien (zolpidem) and Lunesta (zopiclone) can be effective while limiting the hangover effect especially in those who have previosly tolerated the medication (Level A). Zolpidem may be more effective than melatonin and placebo at countering jet lag symptoms. Note: the use of both medicines together was not more effective than zolpidem alone but did cause daytime somnolence.
Stimulants: Care should be used in the athlete as most of these medications are banned in competition. There is a potential off label use for Provigil (modafinil) for improving daytime sleepiness associated with jet lag (currently approved for narcolepsy).
Caffeine, while not banned for the World Anti-Doping Agency, is a monitored substance. It increases daytime alertness and may accelerate entrainment in new time zones when consumed in the morning (later ingestion may interfere with sleep induction) (Level A).
There is a growing recognition of patients who have a subtoxic acetaminophen level at the 4-hour mark, but then still go on to have a toxic level later.
This is concerning in that we usually can exclude the chance for toxicity if the 4-hour, post-ingestion level is < 150 mcg/mL following an acute ingestion (plotted on Rumack-Matthew nomogram).
It still is not clear exactly what subset of patients need to have a second level drawn, but a recurring theme seems to be ingestion of acetaminophen in combination with agents that slow GI motility, such as diphenhydramine or opioids. It may be worth ordering a second APAP level (possibly at 8 hours) in patients ingesting these prodcuts.
Lung Protective Ventilator Settings Still Underutilized

Takotsubo cardiomyopathy a.k.a. stress cardiomyopathy is an acute reversible disorder characterized by left ventricular (LV) dysfunction most commonly affecting postmenopausal women
The LV adopts the shape of an octopus trap (“takotsubo”) describing the narrow neck and broad base globular form during systole
Symptoms include precordial chest pain, dyspnea, or heart failure presenting with pulmonary edema mimicking ACS
Mayo Clinic Diagnostic Criteria
- Suspicion of AMI based on symptoms and STEMI on ECG
- Transient hypokinesia or akinesia of the middle and apical regions of LV
- Functional hyperkinesia of the basal region of LV
- Normal coronary arteries (luminal narrowing <50%)
- Absence of recent head injury, ICH, HCOM, myocarditis, or pheochromocytoma
Treatment is symptomatic and determined based on complications during the acute phase; occasionally requiring IABP or ECMO
Prognosis is better than those with ACS, however initial LVEF is similar to those seen with ischemic heart disease
A recent paper reviewed 53 articles to assess the utility of vasopressors in cardiac arrest. The authors aimed to determine if vasopressors improved ouctomes in this patient population. Here are their conclusions:
Although these conclusions don't support the use of vasopressors in cardiac arrest, we should not abandon these therapies. Most of the trials were completed before wide-spread recognition of the post-cardiac arrest syndrome, implementation of therapeutic hypothermia protocols, and early cardiac catheterization.
Henoch-Schonlein Purpura (aka. Anaphylactoid purpura) is a small vessel vasculitis.
Background:
Clinical Features:
Etiology:
Diagnosis:
Treatment:
Acute, uncomplicated cystitis (in the non-pregnant female):
· The drug of choice is SMX/TMP (provided the resistance rate is <20%) X 3 days.
· An alternative is nitrofurantoin X 5 days.
Acute, uncomplicated pyleonephritis (in the non-pregnanct female) may be treated with:
· Levofloxacin X 5 days, or ciprofloxacin X 7 days (provided resistance rate is <10%).
· Alternatively, SMX/TMP may be used X 14 days.
Crystalloids (i.e., 0.9% saline and lactated ringers) have been used during resuscitation for more than a century. Their invention, however, was more accidental than intentional.
Crystalloids were first used during the European Cholera epidemic of 1831. Hartog Hamburger later modified this solution in 1896 to the solution we know today as "normal" saline. Hamburger's solution was only intended for in vitro study of RBC lysis and was never intended for clinical use.
Around this time, Sydney Ringer was testing several fluids to use for physiologic studies. Ringer's lab assistant was erroneously substituting tap water for distilled water when preparing these solutions. Ringer later discovered that this tap water contained minerals making the solution "physiologic", isotonic, and safe for human use; Alexis Hartmann later added sodium lactate to create Ringer's Lactate.
Since the invention of crystalloids, many types of resuscitation fluids have been created and studied (i.e., albumins, gelatins, and starches); all have been shown to be more expensive, with no more benefit, and with possibly more harm when compared to crystalloids.
The "perfect" resuscitation fluid still alludes us today, but of all of the solutions marketed crystalloids are arguably the best...despite their accidental history.
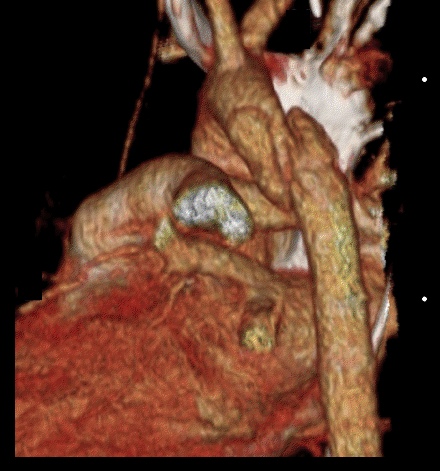
25 year-old male was struck by a car while crossing the street. Chest X-ray and CT Chest with 3D reconstruction are shown below. What's the diagnosis?

Yamaguchi Cardiomyopathy
Yamaguchi cardiomyopathy a.k.a. apical hypertrophic cardiomyopathy (AHCM) was first described 1976 in Japanese patients.
AHCM is a variant of hypertrophic cardiomyopathy that is nonobstructive with predominant involvement of the apex of the heart.
AHCM is frequently misdiagnosed as ACS or STEMI since the typical ECG abnormalities include giant inverted T waves or ST elevation in the mid precordial leads, however coronaries are characteristically clean on cardiac catheterization.
Echocardiography classically used to diagnosis HCM may frequently miss AHCM because hypertrophy is only localized to the apex.
Nuclear magnetic resonance imaging or angiography reveals the pathognomonic "ace of spades" configuration of the left ventricle with systolic obliteration of the apical region.
Unlike HCM sudden cardiac death is very uncommon.
Travel across time zones is regularly required of profession and collegiate athletes (in addition to the some of us professionally)
Jet lag is defined as insomnia or excessive daytime sleepiness/malaise following travel across at least 2 time zones
Symptoms usually persist 1 day for each time zone crossed
The sleep schedule is primarily modulated by light and melatonin
Secretion of melatonin helps induce sleep
Exposure to light stimulates arousal and inhibits melatonin secretion
Who is at risk?
Those with more rigid sleep habits have more symptoms
“Morning” people have less difficulty flying eastward
“Evening” people have less difficulty flying west
However, overall, eastward travel causes the most severe symptoms which persist for up to 7 days (versus <3 days with westward travel)
(The length of the day gets shortened and the circadian system must shorten to reestablish a normal rhythm. The human body demonstrates a natural tendency toward periods longer than 24 hours)
Those with higher levels of physical fitness adjust more quickly
Effects similar in men and women
Midday arrivals experience fewer symptoms than morning arrivals
Symptoms are less in those who have traveled the journey previously
Symptoms are less in those who had a shorter interval their last full nocturnal sleep in the departure city and their first full nocturnal sleep in the destination city
Bonus pearl: Types of Jaundice by Age
- < 24 hrs: hemolyis, TORCH, bruising from birth trauma (ie- cephalohematoma), acquired infection
- Day 2-3: Physiologic
- Day 3-7: infection, congenital diseases, TORCH
- >1 week: Breast Milk Jaundice, breast feeding jaundice, drug hemolysis, hypothyroidism, biliary atresia, hepatitis, red cell membrane disorders (SS, HS, G6PD deficiency)
CIWA-Ar (Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised)
The use of a scoring system for the disposition of an ethanol withdrawal patient can be helpful. The CIWA-Ar Score can guide both treatment in the ED as well as admission versus discharge. Most studies have verified that a score of <8 can be treated outpatient; 8-15 requires treatment and >15 wil require admission/IV benzodiazepines.
N/V: 0-7 (None to Constant N/V)
Tremor: 0-7 (None to Severe even with arms not extended)
Sweats: 0-7 (None to Drenching Sweats)
Anxiety: 0-7 (None to panic attack/delirium)
Agitation: 0-7 (None to pacing/thrashing during interview)
Tactile Disturbance: 0-7 (Mild itching to Continuous Hallucinations)
Auditory Disturbances: 0-7 (None to Continuous Hallucinations)
Visual Disturbances: 0-7 (None to Continuous Hallucinations)
Headache: 1-7 (Miild to Extremely Severe)
Orientation: 0-4
Go to this website to see the actual tool and how it should be administered:
http://www.regionstrauma.org/blogs/ciwa.pdf
Steroids and Septic Shock
