Thrombotic Thrombocytopenic Purpura (TTP)
Do you place central-lines?
Do you suture your central-lines into place?
Do you ever get worried that you are going to stick yourself with that needle?
If you answered yes to any of these questions, then maybe this pearl is for you; click here
Aortic valve (AV) stenosis associated with gastrointestinal angiodysplasia
Proteolysis of Von Willebrand (type 2A) as it passes through the stenotic valve is one culprit of bleeding
Hemostatic abnormalities e.g. GI bleed are often corrected after AV replacement
Valve replacement is only recommended for cardiac symptoms
Fight Bites
The incidence of pediatric syncope is common with 15%-25% of children and adolescents experiencing at least one episode of syncope before adulthood. Incidence peaks between the ages of 15 and 19 years for both sexes.
Although most causes of pediatric syncope are benign, an appropriate evaluation must be performed to exclude rare life-threatening disorders. In contrast to adults, vasodepressor syncope (also known as vasovagal) is the most frequent cause of pediatric syncope (61%–80%). Cardiac disorders only represent 2% to 6% of pediatric cases but account for 85% of sudden death in children and adolescent athletes. 17% of young athletes with sudden death have a history of syncope.
Key features on history and physical examination for identifying high-risk patients include exercise-related symptoms, a family history of sudden death, a history of cardiac disease, an abnormal cardiac examination, or an abnormal ECG.
Intubated patients may occasionally meet certain criteria for extubation while in the Emergency Department. Extubation is not without its risk, however, as up to 30% of patients have respiratory distress secondary to laryngeal and upper airway edema, with some patients requiring re-intubation.
Prior to extubation, Intensivists use a brief “cuff-leak” test (deflation of the endotracheal balloon to assess the presence or absence of an air-leak around the tube) to indirectly screen for the presence of upper airway edema and ultimately the risk of re-intubation. The cuff-leak test is performed by deflating the endotracheal balloon followed by one or more of the following maneuvers:
Ochoa et al. performed a systematic review to determine the accuracy of the “cuff-leak” test to predict upper airway edema prior to extubation. The authors concluded that a positive cuff-leak test (i.e., absence of an air-leak) indicates an elevated risk of upper airway obstruction and re-intubation. A negative cuff-leak test (i.e., presence of an air-leak), however, does not reliably exclude the presence of upper airway edema or the need for subsequent re-intubation.
Bottom line: No test prior to extubation reliably predicts the absence of upper airway edema. Patients extubated in the Emergency Department require close observation with airway equipment located nearby.
Guide-wires can be challenging to dispose of after central-line insertion because they are difficult to keep on the field, hard to place in the sharps box, and can splash nearby observers.
Click here for this little guide-wire disposal trick.
SLAP tear/lesion – Superior labral tear anterior to posterior
Glenoid labrum – A rim of fibrocartilaginous tissue surrounding the glenoid rim, deepening the “socket” joint and is integral to shoulder stability
http://www.orthospecmd.com/images/shoulder_labral_tear_anat_02.jpg
Injury is most commonly seen in overhead throwing athletes
Or from a fall on the outstretched hand, a direct shoulder blow or a sudden pull to the shoulder
Sx’s: A dull throbbing pain, a “catching” feeling w/ activity. Some describe clicking or locking of the shoulder. May also include nighttime symptoms. Pain is located to the anterior, superior portion of the shoulder.
Athletes may describe a significant decrease in throwing velocity
http://sitemaker.umich.edu/fm_musculoskeletal_shoulder/o_brien_s_test
Just when you think buying organic protects you from chemicals and pesticide, along comes the studies detecting arsenic in rice products and specficially in organic foods with brown rice organic sweetener. An organic toddler milk formula reportedly had 6x EPA standards for safe drinking water limit.
The more toxic arsenic is the inorganic arsenic which can cause neuropathy but after chronic exposure can cause a classic arsenic keratosis - see attached pic. The inorganic is seen commonly in seafood and is more easily excreted by the body. Unfortunately, in the study referenced here, inorganic As was the predominant type.
The Lung Transplant Patient in Your ED
27 year-old woman with AIDS presents complaining of a painful, puritic, and papular rash. What's the diagnosis?

Pericarditis is based on clinical diagnosis; typically two of four criteria are found (pleuritic chest pain, pericardial rub, diffuse ST-segment elevation, and pericardial effusion).
Treatment of pericarditis should be targeted at the cause.
Most causes of pericarditis have a good prognosis and are self-limited.
Lactate levels help to confirm septic arthritis but what about bacterial meningitis. As reported in the daily electronic ACEP newsletter a small study of 45 patients showed that all patients with a confirmed diagnosis of bacterial meningitis had a CSF lactate level > 3.5 mmol/L. Therefore, it might be true that viral meningitis will only have CSF lactate levels < 3.5 mmol/L.
With only 45 patients, this finding is clearly not ready for Prime Time but consider adding it to your next CSF study so more data can be collected on the utility of this test.
The story as seen in ACEP eNews on September 14th, 2012 is:
MedPage Today (9/14, Gever) reports, "Cerebrospinal fluid (CSF) levels of lactate were a perfect marker of viral versus bacterial meningitis in a small study, a researcher reported" at the Interscience Conference on Antimicrobial Agents and Chemotherapy. Researchers found that, "among 45 adults in whom the etiology of meningitis was microbiologically confirmed, all those with CSF lactate levels above 3.5 mmol/L had the bacterial form, whereas every patient with lower levels had viral meningitis."
Carbon monoxide (CO) and hydrogen cyanide (HCN) are two of the main gases causing injury and death from smoke inhalation in fire victims. During the first phase of a fire, and prior to depletion of oxygen reserves and subsequent production of CO, formation of HCN from the thermal breakdown of nitrogen-containing materials may be the primary cause of lethal poisoning in an enclosed-space fire.
A recent, retrospective, observational study from Poland assessed the prevalence of toxic HCN exposure in victims of enclosed-space fires.
Important findings:
Conclusion: The high prevalence of coincident HCN concentrations and COHb levels in victims of enclosed-space fires emphasises the need to suspect HCN as a co-toxin in all persons rescued from fire who show signs and symptoms of respiratory distress.
40 year-old male with severe uncontrolled hypertension presents with altered mental status (head CT below). The CXR is from the same patient. What's the connection?
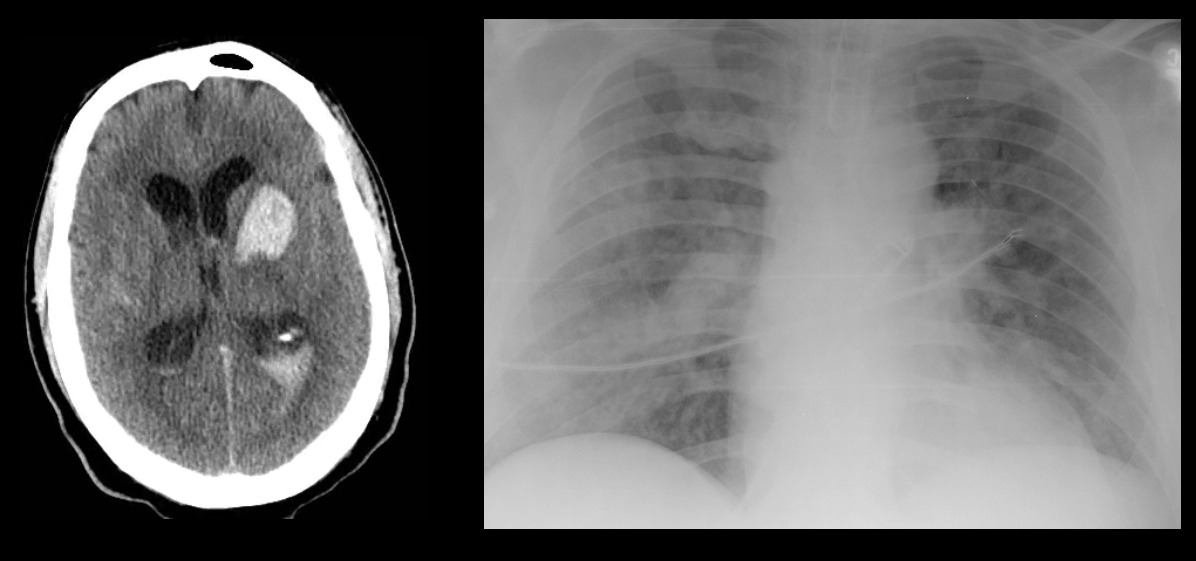
40 year-old male with severe uncontrolled hypertension presents with altered mental status. Head CT is shown here. Name three common anatomic locations generally seen for non-traumatic intracerebral hemorrhage.
{kind=link}