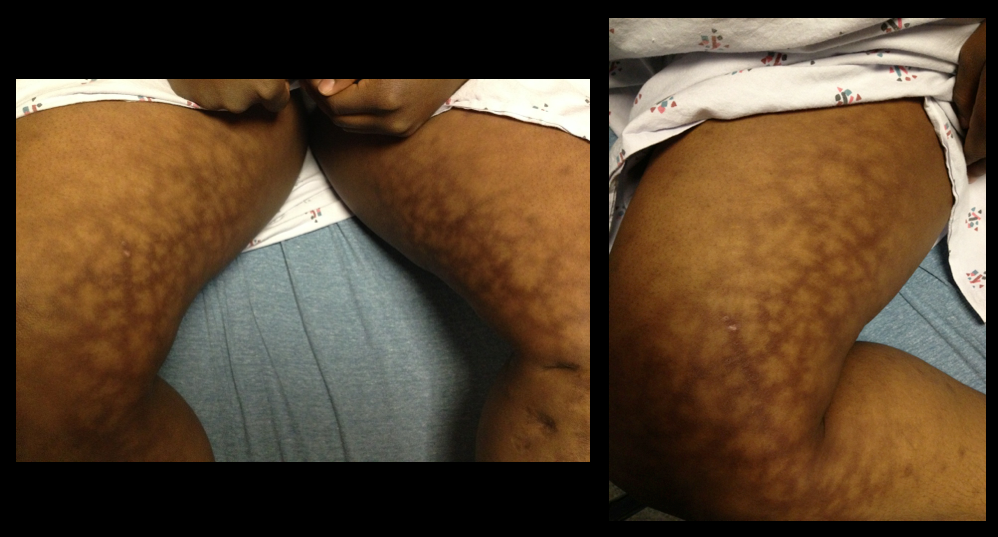
A 25 year-old female presents complaining of a "net-like" rash bilaterally on her medial thighs. She denies any pain but states that the rash looks “pretty scary” What's the diagnosis?
-Common life-threatening cardiovascular effects of cocaine intoxication include tachydysrhythmias, ventricular fibrillation, myocardial ischemia, and infarction.
-Emergency management of acute cocaine intoxication relies mainly on supportive and symptomatic treatment, w/liberal use of gamma-aminobutyric acid receptor agonists such as benzodiazepines.
-Intravenous lipid emulsion (ILE) therapy has been used successfully to treat cardiac toxicity associated with a variety of lipid-soluble drugs, such as local anesthetics, calcium/beta-blockers, tricyclic anti-depressants, and cocaine.
-The current hypothesis, called the “lipid sink” hypothesis, suggest that ILE infusion creates an expanded lipid phase in the plasma that absorbs the circulating lipophilic toxin and decreases the amount of free unbound toxin available to bind to the myocardium.
-When life-threatening cardiac arrhythmias (e.g. wide-complex tachycardia/prolonged QT) are not amenable to standard therapy (e.g. sodium bicarbonate/magnesium) consider ILE as a potential option to the current algorithm.
Estimated 3.8 million sport-related concussions per year (likely significantly higher due to underreporting)
Most patients recover within a 7-10 day period
** Children and teenagers require more time than college and professional athletes
This "accepted" time for recovery is not scientifically established and there is a large degree of variability based on multiple factors including age (as above), sex & history of prior concussions
Approximately 10% of athletes have persistent signs and symptoms beyond 2 weeks (which may represent a prolonged concussion or the development of post-concussion syndrome)
During this time the patient should have complete rest from all athletic activities, close follow-up with PCP and be educated re concussions.
If practical, "cognitive rest" should also be prescribed. This is one of the most frequently neglected aspects of post-concussion care and will be discussed in a future pearl.
Just a quick clarification to last week's melioidosis pearl:
An astute reader noted the typo: "The patient should also be covered for melioidosis, and infection caused by Burkholderia pseudomallei." The sentence should read "...meliodosis, an infection caused by Burkholderia pseudomallei."
Just to clarify, melioidosis is caused by the bacteria Burkholderia pseudomallei.
Many apologies for any confusion this might have caused.
Thanks for reading!
Andi Tenner, MD, MPH
Background Information:
Active tuberculosis (TB) develops in 5-10% of individuals who become infected with M. tuberculosis, typically after a latency period of 6-18 months (but sometimes decades later). Compliance with the 9 month self-supervised isoniazid (INH) regimen has been porr with completion rates <60%. Until recently, daily rifampin for 4-6 months has been the only alternative when the bacterium is resistant or INH cannot be used.
Pertinent Study Design and Conclusions:
Bottom LIne:
A substantially shorter course of therapy with INH-RPT is now the recommended treatment for latent TB.
University of Maryland Section of Global Emergency Health
Author: Emilie J. B. Calvello, MD, MPH
Needle Decompression - Are we Teaching the Right Location?
40 year-old male presents with fever, chills, & cough. What’s the diagnosis and the MOST likely cause?
Intraosseus (IO) access has become quite popular in critically ill patients requiring immediate resuscitation. In a patient responsive to pain, however, pain and discomfort is associated with the force of high-volume infusion through the established line.
Before flushing the line, consider administering preservative-free 2% lidocaine (without epinephrine) for patients responsive to pain prior to flush.
The suggested dose is 20-40 mg (1-2 mL) of the 2% lidocaine, followed by the 10 mL saline flush.
If preservative-free 2% lidocaine is not stocked in your ED, now is the time to consider adding it.
This winter season has brought a rise in influenza and RSV activity in Maryland and in many parts of the country. It is also important to remember other potentially lethal infections that are prevalent in the winter and early spring months, such as Neisseria meningitidis. In fact, a recent study2 showed a potential increase in meningococcal disease when influenza and RSV activity is high.
What:
Encapsulated, gram-negative diplococcus
Where:
Found in nasopharyngeal secretions, carrier rates 2-30% in normal populations
Who:
Age of incidence has 2 peaks: children < 2 years old, teens 15-19 years old
Young adults who live in shared housing, such as college dorms and military recruits
Clinical Presentation:
Early non-specific symptoms of URI, fever, malaise, myalgias
Meningitis: non-specific prodrome + headache, stiff neck (not found in younger children who often present atypically with irritability and/or vomiting)
Meningococcemia: above symptoms + hypotension + petechial rash (>60% of patients)
Treatment:
Early (!) antibiotics: 3rd generation cephalosporins (<3mo: cefotaxime; older infants, children, and teens: ceftriaxone); PCN G is antibiotic of choice for susceptible isolates
Early and aggressive management of shock
Prevention:
Tetravalent vaccine, MCV4 (Menactra, Menveo), available for serogroups A, C, Y and W-135 is given routinely at age 11-12 years old with an additional booster at 16-17 years old. MCV4 does not protect against serogroup B which accounts for 30% of infections.
There have been many attempts to reduce the incidence of contrast-induced nephropathy. Mechanism usually centers around antioxidant properties or free radical scavengers that prevent the acute kidney injury that may result after intravenous contrast. IV Fluid hydration, sodium bicarbonate and acetycysteine have been studied with only some evidence. There is also some controversial data that is beginning to surface regarding the use of atorvastatin with a recent article in Circulation 2012 that showed high dose atorvastatin (80mg) 24 hrs prior to angiography prevented contrast-induced acute kidney injury in patients with mild to medium risk. Link to article has been provided:
http://circ.ahajournals.org/content/126/25/3008
Case Presentation:
A 43 year old diabetic woman presents with dyspnea and a dry cough. Her vital signs are: BP 84/42, HR 135 RR 37 T 38.5. Lobar consolidation is seen on chest xray. She decompensates and is intubated, a central line is placed, and IV fluids are started. Her husband reports that they had just returned from a vacation in Thailand one week earlier.
Clinical Question:
Does the recent travel change your choice of empiric antibiotics?
Answer:
The patient should also be covered for melioidosis, and infection caused by Burkholderia pseudomallei.
Bottom Line:
Patients presenting with severe infections and recent travel to an endemic area should receive emperic antibiotics with ceftazidime or a carbapenem until another source is identified.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
The updated Surviving Sepsis Guidelines have been released (click here) and here are some recommendations as they pertain to hemodynamic management (grades of recommendations in parenthesis).
Fluid therapy
Vasopressors (targeting MAP of at least 65 mmHg)
Corticosteroids
Inotropic Therapy
40 year-old female drove into a ditch. Right sided chest pain and stable vitals. Here's the CT but what do you think the initial CXR showed (Hint: it's a trick)?
Hematoma Block
Provides good aesthesia for reduction of fractures. Onset in approximately 5 minutes
Benefits: No need for NPO, simple and easy to perform & can be done without additional personnel (unlike w/ procedural sedation)
Contraindications: Open fractures, dirty or infected overlying skin
1) Identify fracture site with x-ray and palpation
2) Clean skin w/ Betadine
3) Insert needle into the hematoma. * Confirm placement by aspirating blood *
4) Inject anesthetic (lidocaine 1 or 2%) into the fracture cavity and adjacent periosteum
http://www.youtube.com/watch?v=tjnsdjfwMmY
Cyclophosphamide-induced hemorrhagic cystitis is a well known to oncologists. This unique complication of this chemotherapeutic drug has a defined mechanism and could be seen in your Emergency Department.
- Hemorrhagic cystitis occurs in 46% of patients that receive cyclophosphamide
- Can occur even months after administration
- 5% can actually die from the hemorrhage
- Treatment: Bladder irrigation, hydration, supportive. Oral adminsitration of MESNA (2mercaptoethan sulfonate) and bladder irrigation with prostaglandins and even methylene blue have been attempted.
A 38 year old man is brought in by ambulance for a seizure. His medical history is not known. On exam he is post-ictal and otherwise has a non-focal neurologic exam. He has an abrasion above the right eye, a small tongue laceration, and was incontinent of urine. A head CT was done and is shown below. What was the cause of this man's seizure?

Postintubation Hypotension
