A 1 year old gets sent from their pediatrician’s office for rule out meningitis. They presented with fever for 2 days and neck rigidity. Your LP results are normal. What additional test should you consider?
· Explosions can cause a complex series of injuries, which may include subtle or delayed findings. Repeated evaluations, such as serial abdominal exams, may be required.
· Blast injuries are divided into 4 categories:
o Primary blast injuries: Injury from blast wave over-pressure. Found in gas filled structures (ear, lung, hollow organs)
o Secondary blast injuries: Injury from thrown objects (primarily penetrating trauma, but may blunt)
o Tertiary blast injuries: Injuries from patient being thrown by blast wave (blunt trauma)
o Miscellaneous (quaternary) blast injuries: Injuries from other causes, such as burns, crush injuries, rhabdomyolysis, and toxic chemicals.
· The most common primary blast injury is tympanic membrane rupture.
University of Maryland Section for Global Emergency Health
Author: Jon Mark Hirshon
Burn Patients and Antibiotic Dosing
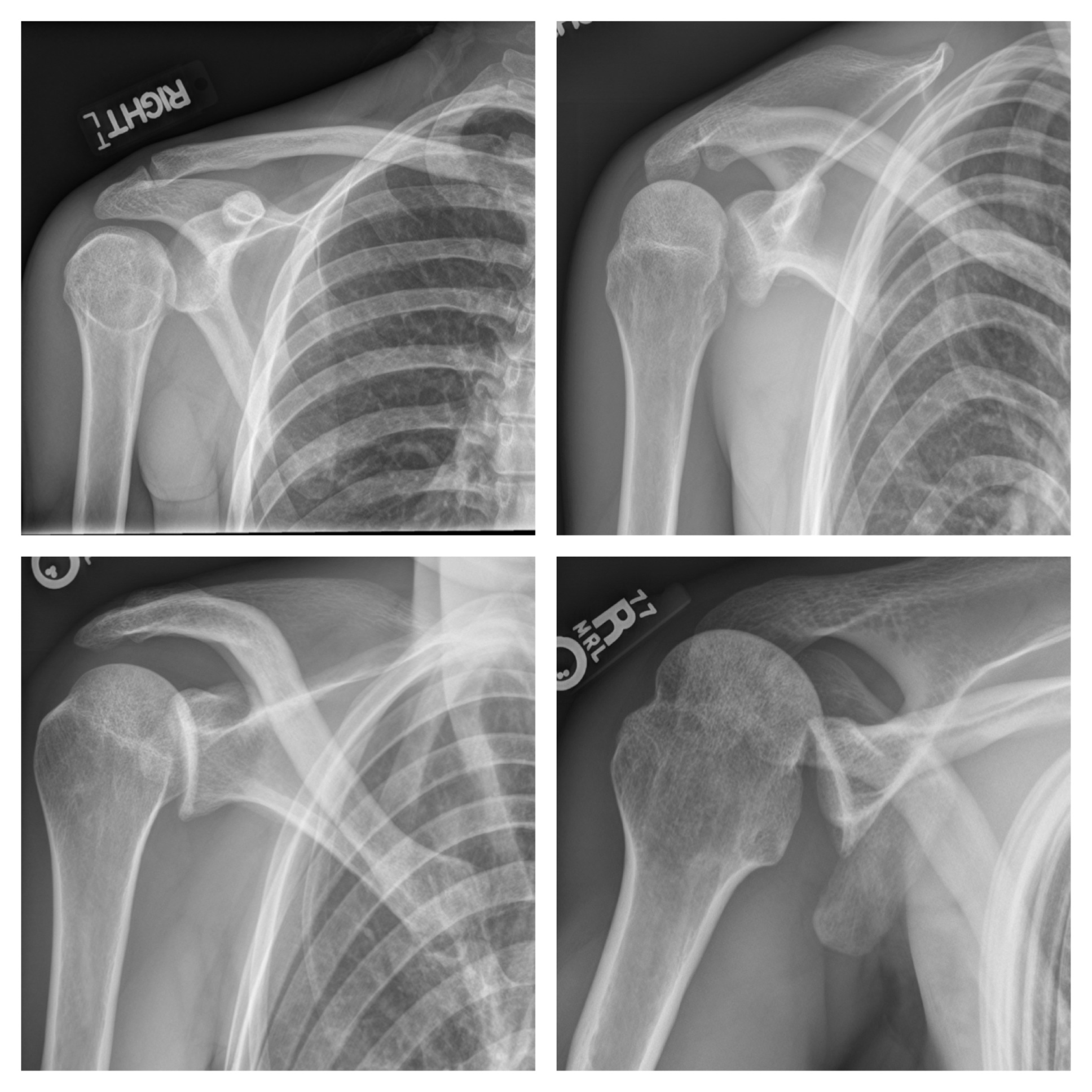
33 year-old male found unconscious by EMS and complains of right shoulder pain upon waking up in the ED. Diagnosis?
Injury is often caused by sudden dorsiflexion on a plantar flexed foot w/ the knee in extension or similarly sudden knee extension with the ankle in a dorsiflexed position.
Injury has a predilection for the poorly conditioned middle-aged athlete, with "thick calves" who are engaged in strenuous activity
Strains are treated with ice, analgesics, and compression (decreases hematoma size and facilitates healing)
Also, consider casting/splinting as dictated by injury severity, such as with a night splint or a CAM boot.
Severe strains and ruptures can be splinted in plantar flexion for 3 weeks.
Background
Patients who are intoxicated with, or emerging from, phencyclidine (PCP) highs present with acute agitation that can be challenging to treat
Risks of physical restraints for combative patients include injury, hyperthermia, rhabdomyolysis, and increased agitation or excited delirium
Haloperidol is an option for chemical restraint that is typically safe and rapid acting
Some concerns related to haloperidol use in PCP-intoxicated patients include worsened PCP-induced hyperthermia, dystonic or anticholinergic reactions, lower seizure threshold, and hypotension
Data
A recent retrospective case series assessed the frequency of adverse effects from the combination of PCP and haloperidol
Of 59 cases, only two patients experienced an adverse reaction, and neither could be conclusively linked to haloperidol administration
This analysis had several major limitations including retrospective design for identifying adverse reactions, potential for false positive PCP screens, and possible haloperidol administration more than 24 hours after PCP intoxication
Bottom Line
While haloperidol may be safe for agitated PCP-intoxicated patients, this paper adds nothing to refute or support its use. Benzodiazepines and calm environment are still first-line therapy.
It should be noted that no data exist showing poor outcomes in PCP-intoxicated patients administered haloperidol, which begs the question "Is there even an issue?" Dr. Leon Gussow, author of The Poison Review, provides a nice answer and summary of the article here.
University of Maryland Section for Global Emergency Health
Author: Andi Tenner
Previous pearls have described the increasing evidence against colloid (e.g., hydroxyethyl starch) use during resuscitation. Now it appears that the crystalloid 0.9% normal saline (NS) may be under fire.
The use of large volumes of NS has been associated with hyperchloremic metabolic acidosis and harm in animal studies. The risk of harm in humans, however, has been less clear.
Bellomo et al. conducted a prospective observational study in which patients being resuscitated in the control group received NS at the clinicians' discretion; i.e., chloride-liberal strategy. The use of NS was restricted in the intervention group, where other less chloride containing fluids were used for resuscitation (e.g., Ringer's Lactate); i.e., a chloride-restrictive strategy.
The authors found that when compared to patients in the chloride-liberal group, the chloride-restrictive group had significantly less rise in baseline creatinine, less overall AKI, and a reduced need for renal replacement therapy.
Bottom line: Although this was only an observational study, the liberal use of normal saline during resuscitation may increase the risk of AKI and renal replacement therapy.
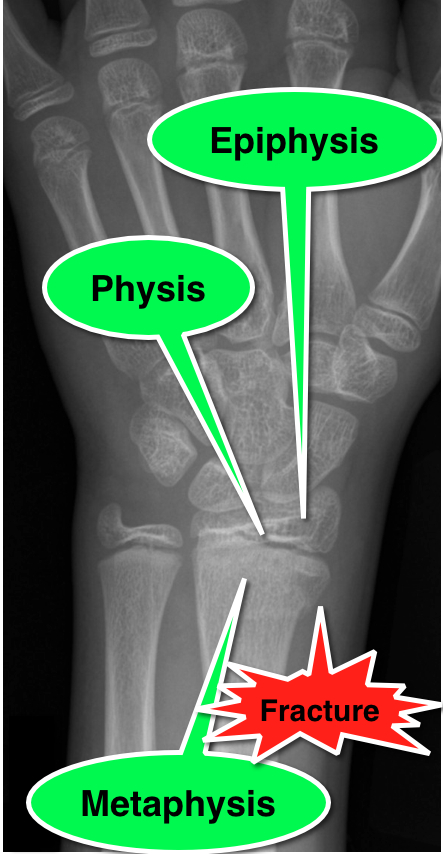
11 year-old male is tackled and falls on his outstretched hand while playing football. X-rays are shown below. What's the diagnosis?

An ECG pattern that signifies occlusion of the proximal left anterior descending coronary artery (LAD) without ST-segment elevation
It seems we've finally put to bed the myth that 10% of penicillin-allergic patients will also react to cephalosporins. Dr. Campagna, et al. recently published a review article concluding that the true cross-reactivity is negligible except when side-chains are similar [PMID 21742459].
This topic was also the subject of a recent post on the Academic Life in EM blog (http://academiclifeinem.blogspot.com/2012/08/busting-myth-10-cephalosporin.html).
But what about the reverse question? Can I give a penicillin to a cephalosporin-allergic patient?
Dr. Romano's group tested 98 patients with skin-test postitive cepahlosprin allergy (mostly IgE -mediated anaphylaxis). Patients were then skin tested for penicillin allergy. Those testing negative were challenged with a penicillin.
25% of patients reacted to the penicillin
Similar side-chain was a strong predictor of cross-reactivity
A Letter to the Editor response to this study pointed out that the authors used a smaller-than-standard size threshold for a positive response to the penicllin AND used a higher-than-standard dose of amoxicillin for testing. In light of this, the rate of subjects with cephalosporin allergy who do not have a history of penicillin allergy but with true IgE-mediated allergy to penicillin might be much closer to 5%.
Bottom line: The cross-reactivity of penicillins in cephalosporin-allergic patients is somewhere between 5-25%.
Conventional pediatric nasal cannula can safely deliver up to 4 lpm but are limited by cooling and drying of the airway. This leads to decreased airway patency, nasal mucosal injury, bleeding and possibly increase in coagulase negative staph infections.
HFNC delivers flow up to 40 lpm with 95-100% relative humidity at a controlled temperature. In infants, the initial flow rate is set between 2-4 lpm and can be increased to 8 lpm. Older children and can be started at 10 lpm and increased as high as 40 lpm. Oxygen is also adjustable.
Studies have shown improved comfort, respiratory rate and oxygenation compared to nasal CPAP.
Diagnosis should be considered in any individual over 5 years old with severe dehydration from diarrhea, regardless of exposure to an endemic area, and any patient over 2 years old with watery diarrhea in an endemic area.
Patients with severe cholera can stool as much as 1 L an hour. Replacing fluids is the most important part of treatment with oral rehydration being used as soon as possible. Oral rehydration therapy provides better potassium, carbohydrate, and bicarbonate replacement than most IV fluid solutions. Antibiotics will also decrease volume and duration of stooling but are only recommended in moderate to severe illness. Antiemetics are not useful because they can make patients sleepy and will reduce their ability to rehydrate orally. Antimotility medications will prolong the duration of illness.
University of Maryland Section for Global Emergency Health
Author: Jenny Reifel Saltzberg
Serotonin Toxicity in the Critically Ill
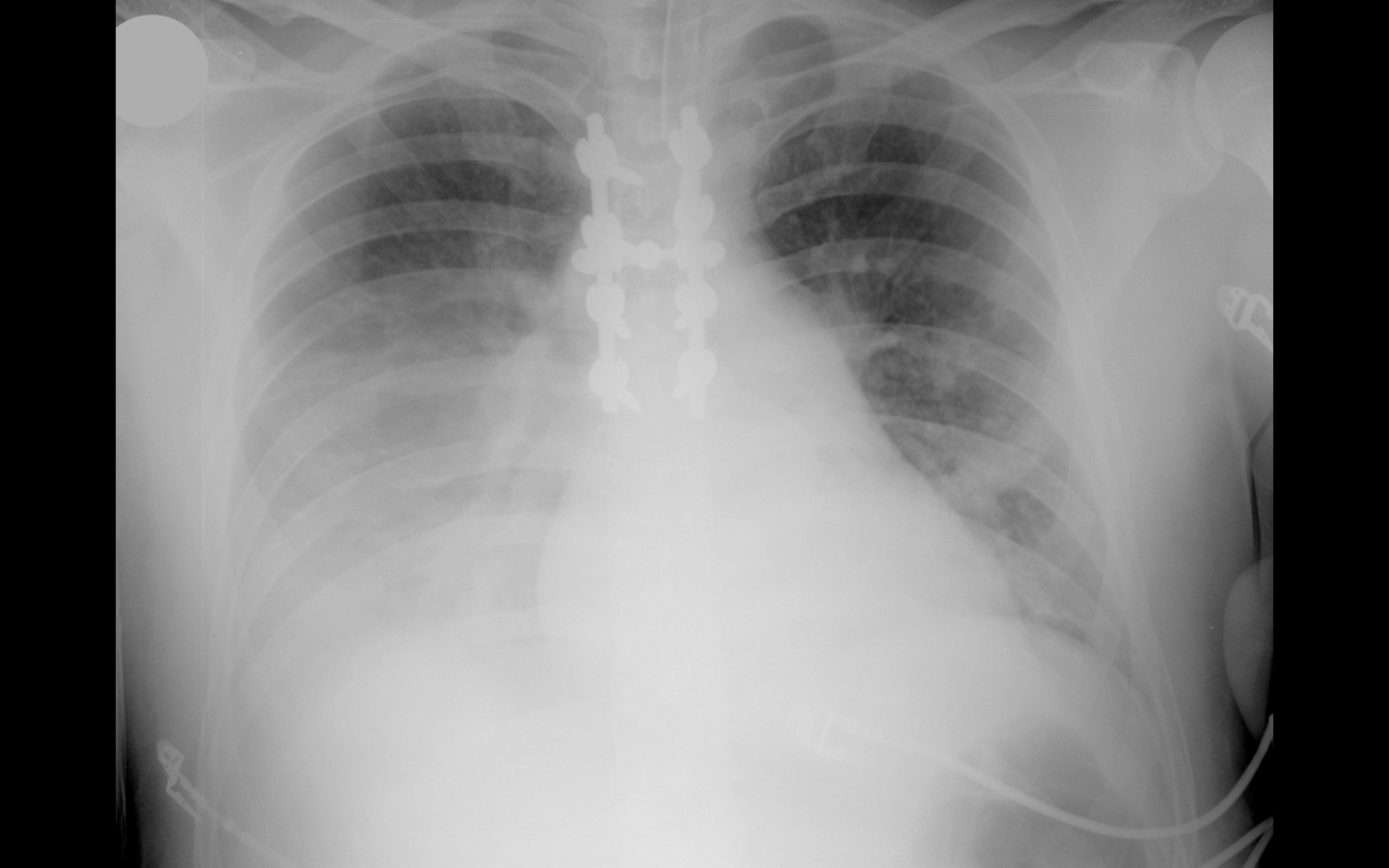
33 year-old male in respiratory distress. What's the diagnosis?
EPSS is an accurate and rapid bedside estimation of left ventricular function
First an image of heart should be obtained in the parasternal long-axis view
The ultrasound cursor should be placed through the anterior leaflet of the mitral valve
Subsequently, M-mode is applied and the distance between the anterior leaflet and the interventricular septum is measured during early diastole
A measurement of 7mm or greater indicates poor EF (see attachment below)