Are discharged patients who suffer minor thoracic injury at risk of developing delayed pneumonia?
Prospective study of 1,057 patients age 16 and older with minor thoracic injury who were discharged from the ED.
32.8% had at least one rib fracture
8.2% had asthma
3.4% had COPD
Only 6 patients developed pneumonia!!
Sex, smoking, atelectasis on CXR, and alcohol intoxication were not significantly associated with delayed pneumonia.
However, for patients with preexistent pulmonary disease (asthma or COPD) AND rib fracture, the relative risk of delayed pneumonia was 8.6. Patients without either of these conditions are at extremely low risk of future development of pneumonia.
Epidemiology:
Trampoline injuries doubled between 1991 and 1996, increasing from 39,000 injuries per year to more then 83,000 injuries per year. Injury rates and trampoline sales peaked in 2004 and have been decreasing since; however, hospitalization rates are still between 3% and 14%.
Risk Factors:
¾ of injuries occur when multiple people are on the trampoline at once
Smaller participants were 14x more likely to be injured then their heavier playmates
Falls account for 27-39% of all injuries
Springs and frames account for 20% of injuries
Up to ½ of injuries occur despite adult supervision
Injury types:
Lower extremity injuries are more common than upper extremity
Head and neck injuries accounted for 10-17% of trampoline injuries
Unique Injuries:
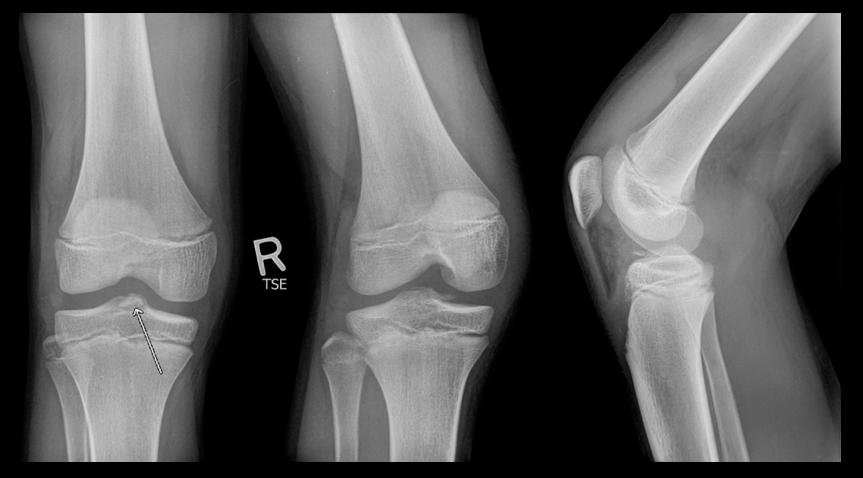
Proximal tibial fractures
Manubriosternal dislocations and sternal injuries
Vertebral artery dissection
Atlanto-axial subluxation
40 yo previously healthy male in China who presents with prolonged “seizure” after receiving a cut on his foot while fishing 5 days ago.
Dx: Tetanus
Clinical features:
· Incubation period 4-14 days
· 3 clinical forms:
1. Local spasm
2. Cephalic (rare) - cranial nerve involvement
3. Generalized (most common) - Descending spasm: facial sneer (risus sardonicus), “locked jaw” trismus, neck stiffness, laryngeal spasm, abdominal muscle spasm.
· Spasms continue to 3-4 weeks and can take months to fully recover
Complications: apnea, rhabodymyolysis, fracture/dislocations
Treatment: supportive, benzodiazepines, RSI, Tetanus IG (3000-5000 units IM), wound debridement
University of Maryland Section for Global Emergency Health
Author: Veronica Pei, MD
An 86 year-old nursing home resident presents to the ED with a urinary tract infection, four days after discharge from the inpatient service for the same diagnosis. She was discharged from the inpatient service with a prescription for ciprofloxacin to be given through her gastric feeding tube (she does not take anything orally). Could her tube feeds be playing a role in the relapse of her urinary tract infection?
11 year-old boy presents with right knee pain and swelling after falling off of his bicycle. What's the diagnosis?
In the rare circumstance you need to treat a patient with suspected PID and an allergy to doxycycline, what is the alternative?
For oral regimens, azithromycin is an option in place of doxycycline.
Suggested regimen for PID with doxycycline allergy:
It is not often that a CT will be able to give you a hint to a toxicologic diagnosis. The following are CT findings that are either suggestive and even sometimes almost diagnostic for a given to toxin:
1) Intraparenchymal or Subarachnoid Hemorrhage: sympathomimetics or mycotic anuerysm rupture secondary to IV drug abuse
2) Basal Ganglia bilateral focal necrosis: characteristic of carbon monoxide, cyanide, hydrogen sulfide and even methanol
3) Severe advanced atrophy out of proportion for age: alcoholism, toluene
General Information:
• Millions of people around the world (including our patients who travel and victims of disasters like Hurricane Sandy) are exposed to non-potable water.
• How to treat contaminated water:
♦ Filter cloudy water through a clean cloth or allow to settle prior to treatment
♦ The safest method is boiling water vigorously for 1 minute (or, at least 3 minutes at altitudes >6,000ft)
♦ Chemical disinfection is not as effective but, if boiling is not possible, use either:
• 2 drops of unscented bleach (5.52% Cl) per quart/liter of water. (Unknown strength? Add 10 drops per quart/liter.)
-Or-
• 5 drops of tincture of 2% iodine per quart/liter.
- If the water is cloudy or cold, double the chlorine or iodine.
- Notes: Pregnant women or people with thyroid conditions should not use iodine
♦ UV decontamination can be accomplished by leaving clear bottles of water in direct sun for >6 hours or special equipment, but requires clear water
• Boiling, Chlorine/Iodine, and UV will kill viruses, bacteria, and Giardia
• Only Boiling kills Cryptosporidium
Bottom Line:
• If bottled water is available, use it.
• If not, boil your water.
• In order to treat for a wide variety of pathogens, it is best to combine available methods.
University of Maryland Section for Global Emergency Health
Author: Andi Tenner
Managing Critically Ill Patients with AKI
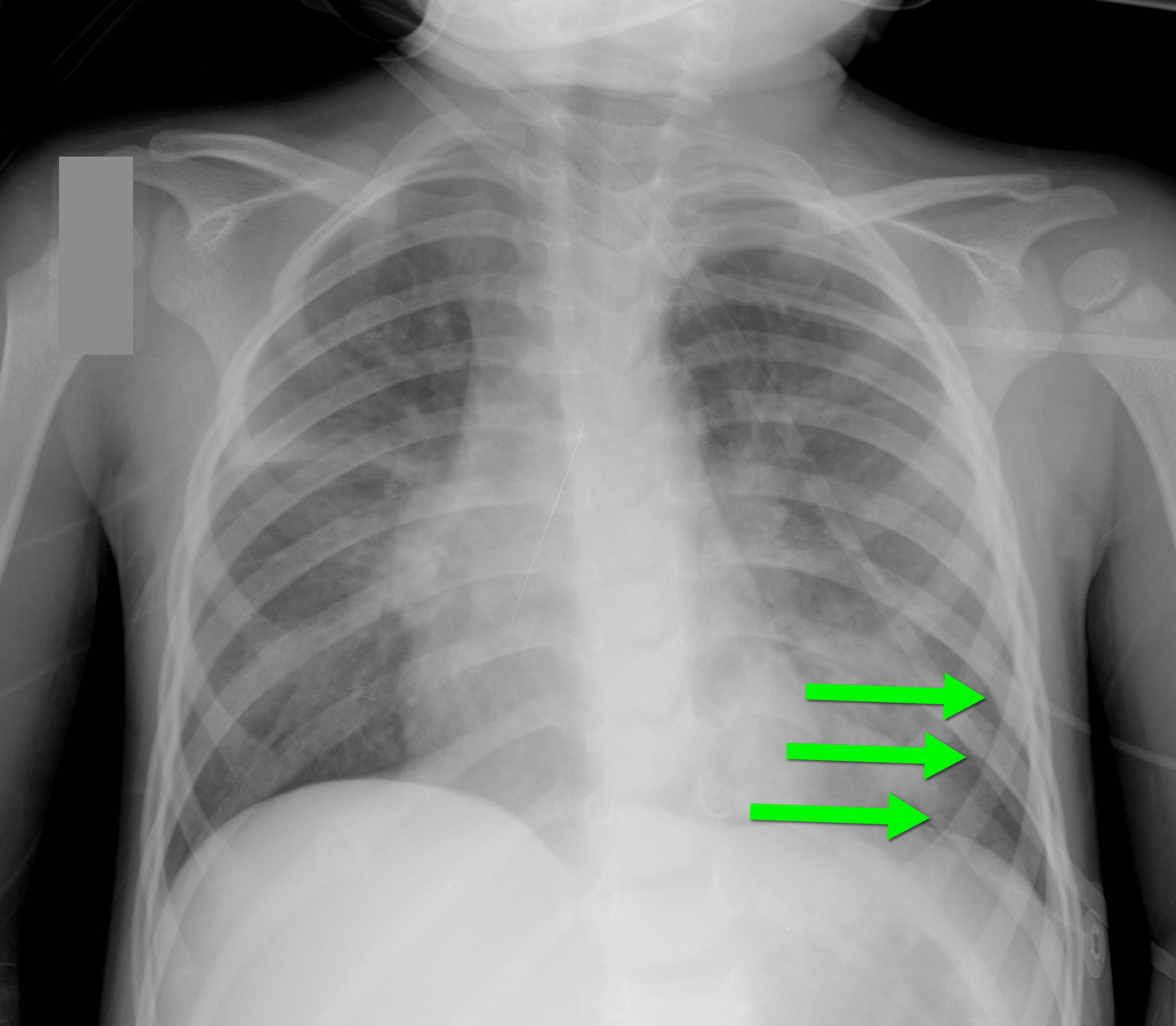
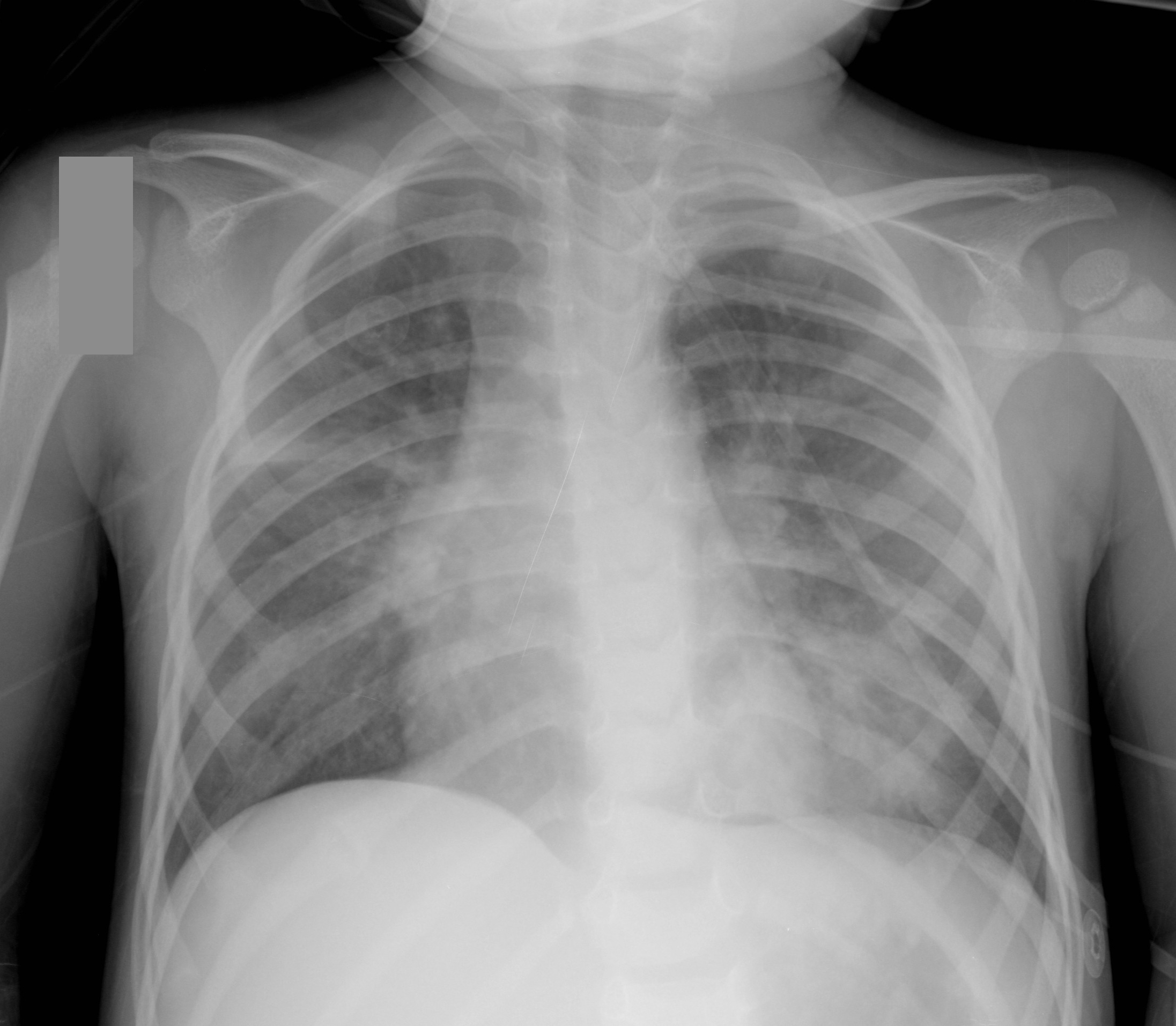
2 year-old male with past medical history of asthma presents with fever and respiratory distress. CXR is shown below. What’s the diagnosis? (Hint: ...look beyond the obvious)
Hematoma blocks for distal radius fractures
Hematoma blocks provide safe, effective analgesia without an increased risk of post procedural infections when compared with other regional blocks
Provide equal reduction quality AND pain control as procedural sedation with Propofol.
However, mean time to reduction (0.9 vs. 2.6 hours) and time to discharge post procedure (0.74 vs. 1.17 hours) were reduced with hematoma blocks.
Consider this option next time the department is busy or the patient is not an ideal procedural sedation candidate.
University of Maryland Section for Global Emergency Health
Author: Emilie J.B. Calvello, MD, MPH
A low-tidal volume (or protective) strategy of mechanical ventilation (i.e., tidal volume of 6-8cc/kg of ideal body weight) has previously been demonstrated to be beneficial in patients with acute respiratory distress syndrome (ARDS).
A meta-analysis was recently performed to determine whether this strategy of mechanical ventilation is also beneficial for patients without lung injury prior to initiation of mechanical ventilation.
Dr. Neto, et al. performed a meta-analysis of 20 studies (total of 2,822 mechanically ventilated patients) comparing a conventional ventilation strategy (average tidal volume was 10.6 cc/kg) to a protective ventilation strategy (average tidal volume was 6.4 cc/kg) of mechanical ventilation.
The authors concluded that patients ventilated with a protective lung-strategy had reductions in:
Bottom-line: This meta-analysis supports the notion that a strategy of low-tidal volume ventilation may have benefits for patients without ARDS, however prospective studies are needed.
Do you like placing ultrasound-guided IV catheters? Check out this trick for covering the probe during the procedure.
http://ultrarounds.com/Ultrarounds/The_Vascular_Probe_Protector.html
or
https://www.youtube.com/watch?v=ZuOq6Ea_FbA&feature=plcp
Tarsal Tunnel Syndrome (TTS)
Prior pearls have addressed Carpal Tunnel Syndrome and Cubital Tunnel Syndrome, which affect the median and ulnar nerves, respectively. Tarsal tunnel syndrome, is a similar compression neuropathy of the tibial nerve as it transverses through the tarsal tunnel of the foot.
The tarsal tunnel is located behind the medial malleolus, and is where the posterior tibial artery, tibial nerve and several tendons transverse. Patients will present complaining of numbness of the foot radiating into Digits 1-4, pain, burning , and tingling of the base of the foot and heel. TTS has many causes and is more common in athletes.
Consider the diagnosis in patients with foot pain and numbness. If interested in more information about TTS please consider reading this eMedicine article, http://emedicine.medscape.com/article/1236852-overview