Updated Guidelines for Traumatic Brain Injury
The Brain Trauma Foundation (BTF) Guidelines for the Management of Severe Traumatic Brian Injury (TBI) was recently updated and published in September 2016.
Updated recommendations include:
For the executive summary and complete guidelines, go to https://braintrauma.org/guidelines/guidelines-for-the-management-of-severe-tbi-4th-ed#/
Oxygen-ICU Trial
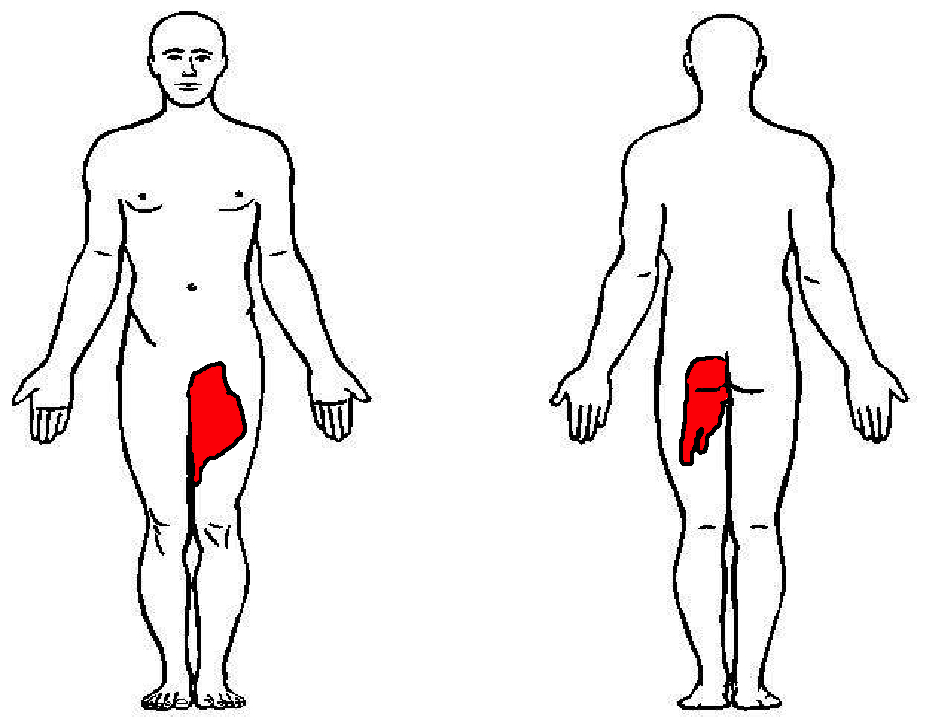
57 year-old female with history of bilateral lung transplants presents with fever, and 2 days of a painful, red, bumpy rash over the left labia and left buttock, but also notes a small tender area on the plantar surface of the left foot.
Below is a figure depicting the location of the rash, as well as a photo of her foot.
%20copy%201.JPG)
Recurrence depends on age and activity level
27% if >30yo and 72% if <23yo
Surgical Recommendations:
Large bony Bankart lesion, glenoid or humeral head defect >25%, recurrent instability, event near the end of season
Non surgical return to play:
If event occurs at beginning/early in season
Rehabilitation for 2 to 3 weeks (most return to play in this time frame)
Immobilization for 3 to 7 days in simple sling, gentle range of motion, cryotherapy
Physical therapy to strengthen dynamic stabilizers
Shoulder stabilization brace for non overhead throwing and contact sports
Fall clean up = Poison Ivy, oak, sumac (Toxicodendron species) which is ubiquitous in North America but it can also be found in British Columbia, Mexico and in parts of Asia. These plants are truly the scourge of outdoor enthusiasts and agricultural workers responsible for up to 40 million cases of miserable often temporarily incapacitating rashes annually.
Fast Facts:
Treatment Tips:
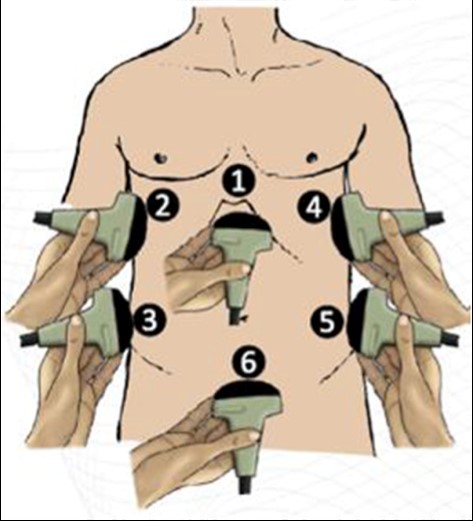
What is the FASH Exam?
Submitted by Dr. Laura Diegelmann
The delta gap is a measurement intended to assess for mixed acid-base disorders. A straightforward alternative, the strong ion difference (SID), allows for a quick and simple assessment of any non-gap acidosis or alkalosis that may be present.
The SID is simply the difference between the strong cations (Na+, K+, Mg+, Ca+) and the strong anions (Cl-) present in the serum. The abbreviated SID is the difference between the serum sodium and serum chloride levels (approximately 138-102). Values typically range from 36-40 mg/dl. Values less than 36 denote the presence of some degree of hyperchloremic, non-gap, acidosis. While values greater than 40 demonstrate the presence of hypochloremic, non-gap, alkalosis. And while on rare occasions, variations in albumin or elevated levels of cations other than sodium can lead you astray, the SID is as accurate as a delta gap at identifying mixed acid-based disorders without the added mathematical complexity.
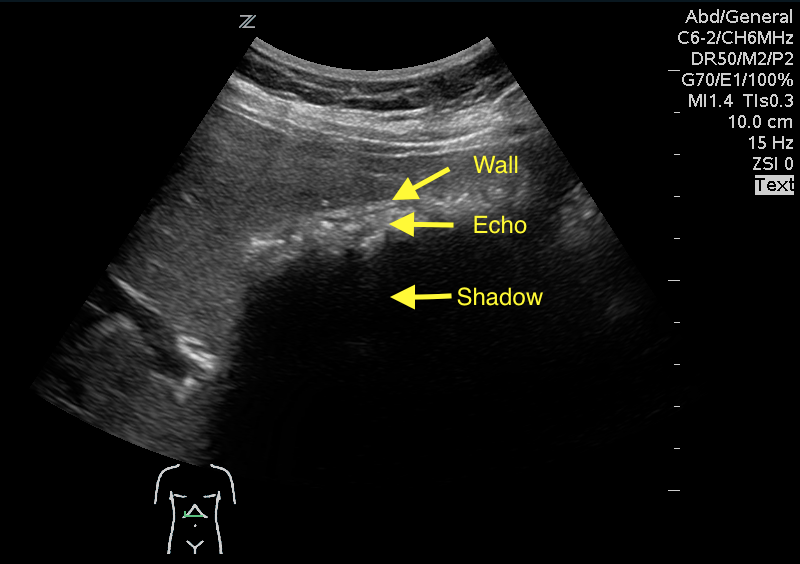
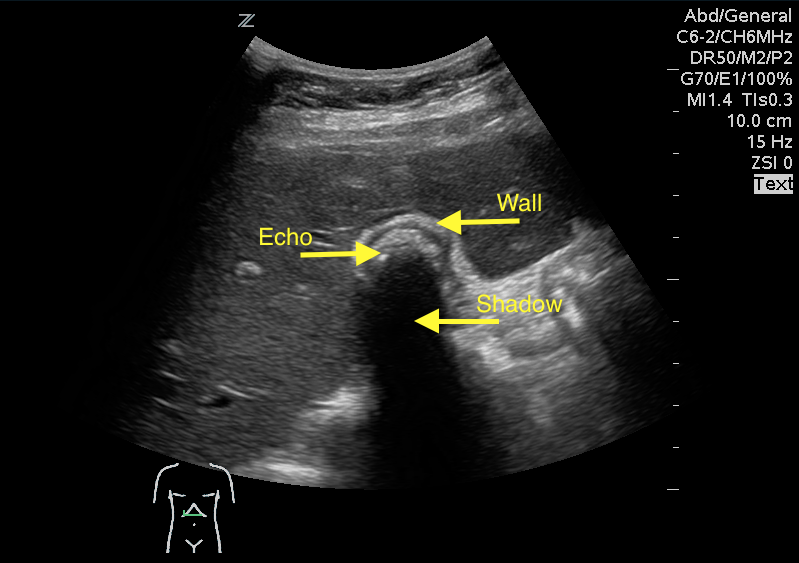
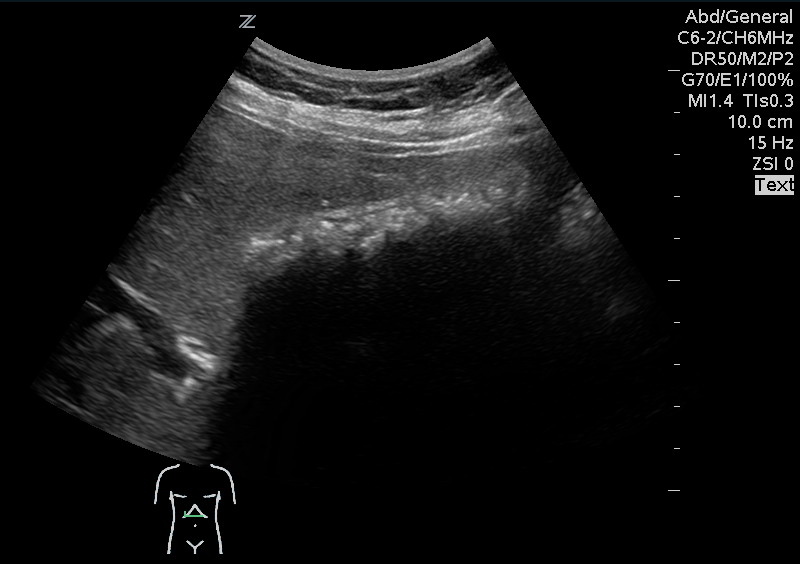
A 41 year old female presenting with intermittent RUQ abdominal pain for 1 week. An ultrasound of the right upper quadrant was performed. What is the diagnosis ?

What they did:
What they found:
Application to clinical practice:
A 12 year old male who recently started middle school presents to the ED with a rash in the periumbilical region that has been developing over the last few weeks. The rash is scaly, somewhat itchy, but otherwise benign appearing. The patient has no known medical conditions other than eczema, and is otherwise well. What is the diagnosis?
Picture courtesy of Mara Haseltine, MD

You have a patient in whom you suspect meningitis, but he is on warfarin for a history of pulmonary embolism. You started empirical antibiotics. His INR is 2.6, and you want to do a lumbar puncture (LP) to confirm your diagnosis. Can you use Prothrombin Complex Concentrate to lower his INR and safely perform the LP?
Take Home Point:
Using PCC to lower INR to enable LP is relatively safe and effective in patients on vitamin K antagonists. The dose used was individually determined by the physician according to initial INR.
Limitation:
This is a retrospective study, with no control group. One patient (2.7%) had a myocardial infarction that was “possibly related” to the PCC administration.
TAKE HOME POINTS:
-- High chloride load is associated with adverse outcomes in large-volume resuscitation (>60mL/kg in 24h), including increased risk of death [1]
-- Avoid supraphysiologic chloride solutions (i.e. normal saline) when resuscitation volumes are likely to exceed 60mL/kg (e.g. sepsis, DKA)
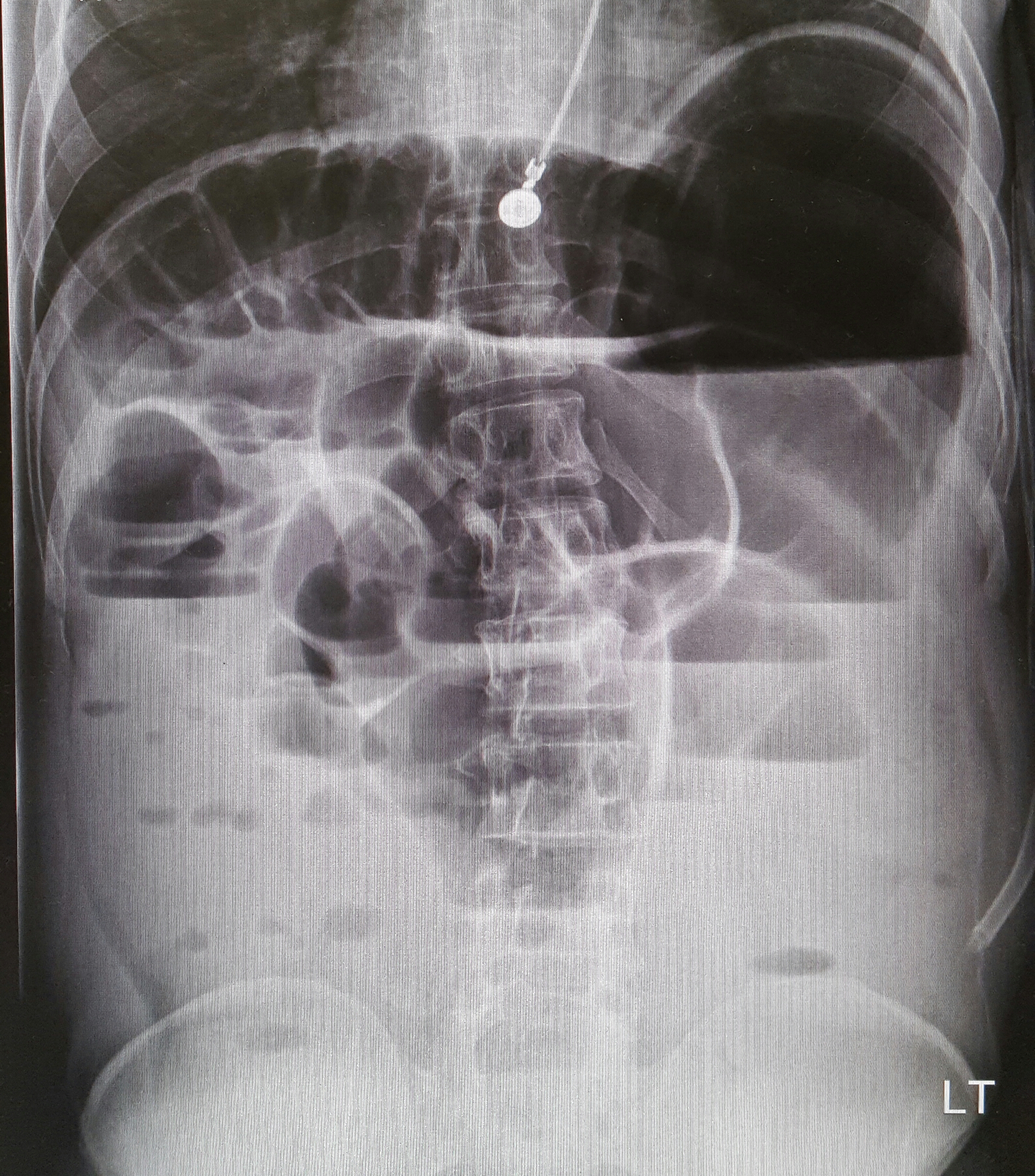
22-year-old male with history of autism, mental retardation who is non-verbal presents with abdominal pain and vomiting for one day. Patient was found clutching his abdomen and moaning. What's the diagnosis?
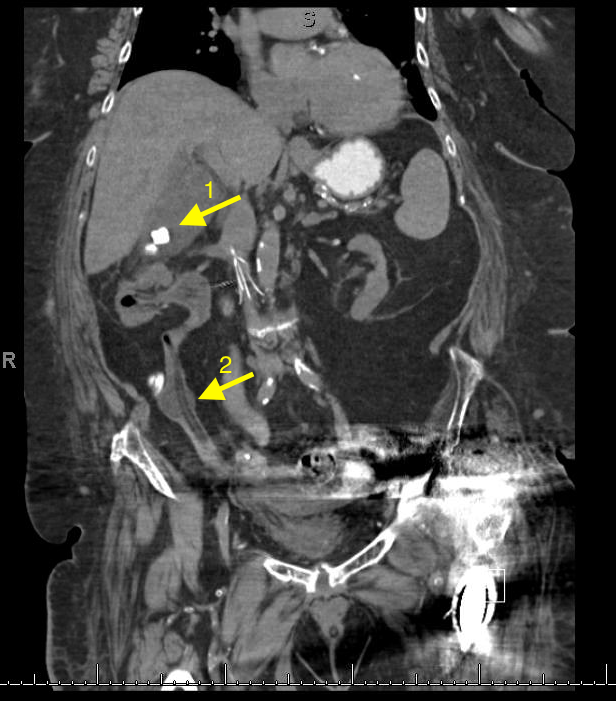
Retroperitoneal hemorrhage
The pathophysiology is unknown. Some hypothesize that occult vasculopathy and arteriosclerosis of the small vessels in the retroperitoneum may render them friable and therefore prone to rupture. This can be seen in minor trauma in sports and forceful vomiting or coughing. Spontaneous bleeding starts at the microvascular level, and large vessels become disrupted or stretched as the hematoma enlarges.
Retroperitoneal hemorrhage occurs in a variety of clinical circumstances, including spontaneous hemorrhage into a pre-existing benign adrenal cyst or bleeding from a left inferior phrenic artery, tumors of the adrenal gland and kidney, rupture of any blood vessel (most commonly infrarenal aorta); percutaneous interventions (such as cardiac catheterization), trauma, and polycythemia vera,
It is most commonly seen in association with patients with bleeding abnormalities, in HD patients and with anticoagulation therapy,. Risk is much greater with unfractionated heparin therapy than with warfarin. In most of the heparin patients studied, their coagulation parameters were in the therapeutic range.
Patients may present to the non acute area of the ED with back, lower abdominal or groin discomfort, Over time, this may progress to hemodynamic instability, and a fall in hemoglobin, Early identification is crucial to improving patient morbidity and mortality. Early symptoms depend on the location of the bleeding.
Hematoma near or within the iliopsoas muscle usually presents as femoral neuropathy (groin pain or leg weakness).
Femoral neuropathy caused by retroperitoneal hematoma can present with sudden onset severe pain in the affected groin and hip, with radiation to the anterior thigh and the lumbar region. This can easily be missed as the presentation is similar to a pulled msucle or strained hip/back. Iliopsoas muscle spasm often results in the characteristic flexion and external rotation of the hip, and any attempt to extend the hip will result in severe pain. Over time, pain and parasthesia in the antero-medial thigh and leg is seen.
Non –communicable diseases (NCDs), primarily cardiovascular diseases, cancer, respiratory diseases and diabetes, are significantly increasing globally. According to the WHO, cardiovascular diseases alone account for 17.5 million deaths annually- the most of any NCD.
If someone has return of spontaneous circulation after cardiac arrest, but does not have ST-elevations on their post-arrest ECG, should you emergently activate the cath lab?
In a just released systematic review and meta-analysis in Resuscitation, Dr. Millin and colleagues found that almost one third of patients successfully resuscitated without ST elevation on their ECG had a culprit lesion that would benefit from emergent intervention.
Bottom Line: While this is not definitive proof to emergently activate the cath lab for a NSTEMI, it is another strong indication that post cardiac arrest patients without ST elevation may benefit from emergent percutaneous coronary intervention.
Pitfalls with PLR
A 67 year old female with history of CVA, presented from a nursing home with RUQ abdominal pain and inablitiy to tolerate PO for 3 days. A CT scan of her abdomen was obtained. What is the diagnosis ?

Patellofemoral Syndrome Treatment options
Patients do best with a combined intervention (ie, exercise therapy, education, manual therapy and taping) plan or patellofemoral bracing may improve outcomes for people with patellofemoral syndrome and the subtype of patellofemoral osteoarthritis.
For for the ED, we can start NSAIDs, and then have them follow up with Physical Therapy, A sports trainer if in organized sports, or with a sports medicine physician/PCP. Physical therapy is targeted at strengthening the quadricep muscle particularly vastus medialis, which improves the patella’s tracking with knee flexion.
114 children with bronchiolitis had end tidal carbon dioxide (ETCO2) measured on presentation to the ED. The ETCO2 levels did not differ significantly between admitted and discharged patients. In the subset of admitted patients, there was no correlation with ETCO2 on admission and days of oxygen requirement or length of stay.
Bottom line: Initial ETCO2 does not predict outcome for patients with bronchiolitis.
Naloxone has been used to reverse opioid-induced respiratory depression for decades. The “standard” dose of opioid intoxication has been 0.4 mg. However, over the past decade, initial naloxone dose for opioid intoxication has evolved to recommend a lower initial dose (0.04 – 0.05 mg).
A recent article by Connors et al. reviewed 25 medical resources (internet, medical texts and study guides) of different medical specialties (internal medicine, medical toxicology, emergency medicine, pediatrics, anesthesiology, pain medicine and general medicine)
Findings:
Recent editions of emergency medicine text (Rosen’s and Tinitinalli) recommend using 0.04 – 0.05 mg IV in ED patients with history of opioid dependence. Higher doses of naloxone are recommended for non-opioid dependent/apneic patients.
However, history of opioid dependence is difficult to obtain in patients with opioid induced CNS/respiratory depression.
Administering 0.4 mg or higher dose may/can acute agitation or opioid withdrawal symptoms that can utilize more ED resources to calm agitated patient/management of withdrawal. Thus it may be prudent to use low-dose strategy (0.04 mg IV with titration) to minimize the risk of precipitating naloxone-induced opioid withdrawal/agitation.
Bottom line:
In opioid-induced respiratory depression/apneic patients:
To make 0.04 mg naloxone solution: