Situations Where ECMO Will Likely Fail
https://www.youtube.com/watch?v=sCFOObsx_W4
What is their risk of MI???
Anger outbursts are bad for your heart. Out of 300 patients with an acute MI, just over 2% reported losing their temper within 2 hours of the event. A review of nine studies of rage and cardiovascular events all found an increase in cardiovascular events in the 2 hours preceding an anger outburst. Examples included arguments at home, at work or by road rage. Compared with their usual anger levels, the relative risk of heart attack from a fit of rage was 8.5.
What about those of us who are just fanatics, I mean fans....A recent study of World Cup soccer found that the intense strain and excitement of viewing a dramatic soccer match more than doubles the risk of acute heart attack, particularly in men with known coronary heart disease. This was regardless of the outcome of the match!
Patients with chronic digoxin toxicity generally have multiple co-morbidities such as renal failure, dehydration, and cardiac failure. Sick patients with chronically high digoxin levels may have more than just digoxin toxicity as the cause of illness.
A New Study
Prospective observational study with the primary objective to investigate changes in free digoxin concentrations and clinical effects on heart rate and potassium concentrations in chronic digoxin poisoning when digoxin immune Fab are given.
What They Found
One to two vials of digoxin immune Fab initially bound all free digoxin confirming Fab efficacy. However, this was associated with only a moderate improvement in HR (49 to 57 bpm) and potassium (5.3 to 5.0 mmol/L).
Application to Clinical Practice
Want to learn more about how to read a brain MRI? Here are the basics:
Stay tuned for more pearls in this series on brain MRI!
Zika virus has received significant media attention in the US due to its recent link with teratogenicity. But Zika is also associated with critical and life-threatening complications, including death. Differentiating it from other Flavivirus diseases such as Dengue or Chikungunya can be challenging.
Diagnosis
Complications
Ketamine is often thought to be the induction agent least associated with hypotension in the peri-intubation period. However, reports of hypotension following ketamine do exist, including 2 cases of cardiac arrest. [1] There are limited objective means to predict which patients may have an adverse hemodynamic response.
New Study
A new prospective observational study followed 112 patients in the prehospital setting who received ketamine for rapid sequence intubation. 81 had a low shock index [< 0.9], 31 had a high shock index. [2]
Shock index = HR / SBP
What They Found
Patients with a high shock index were more likely to experience hypotension (SBP < 90 mm Hg) in the peri-intubation period compared to those with a low shock index (26% vs 2%).
Application to Clinical Practice
Why are selfie deaths on the rise?
People travel everywhere now with their camera equipped smart phones. Capturing a selfie while travelling is very common. This leads to more distracted people and lack of situational-awareness.
Where and how do these deaths occur?
Selfies taken from a height, on a bridge, near motorized traffic, during thunderstorms, at sporting events and near wild animals
Other information:
Submitted by Dr. Laura Diegelmann
Neonatal jaundice- Incidence ~85% of term newborns
Bili levels are EXPECTED to rise during first 5 days of life
Be aware of CONJUGATED hyperbilirubinemias (biliary atresia, infection)
Majority of cases due to increase in unconjugated (indirect) bilirubin 2/2 residual fHgb breakdown and insufficient capacity of hepatic conjugation
Severe hyperbilirubinemia (Tbili >20mg/dL) <2% of term infants
⇒
Acute bilirubin encephalopathy(ABE)- Hypertonia, arching, opisthotonos, fever, high pitched cry
⇒
Kernicterus (5% of ABE)-CP, MR, auditory dysfunction, upward gaze palsy
When to refer for phototherapy/exchange transfusion
A 25 year old patient presents to the emergency department (ED) with a first unprovoked seizure. His ED workup is normal and he is back to his baseline, and you plan to discharge the patient with outpatient follow up within 1 week. The patient is requesting to be discharged on an anti-epileptic drug (AED). What do you do?
Educate the patient about the risk of recurrence, and the possible side effects of AEDs!
The American Academy of Neurology (AAN) specifically addressed this in their 2015 guidelines. A few points to remember:
- The risk of recurrence is greatest within the first 2 years, and occurs in 21-45% of patients.
- The risk of recurrence increases with a remote brain lesion or injury, abnormal EEG, significant brain imaging abnormality or nocturnal seizures.
- AED therapy is likely to reduce the risk of a 2nd unprovoked seizure by about 35% over the next 2 years, but the delay in initiating therapy does not increase the long-term remission risk.
Is it different if the patient had multiple seizures within 24 hours?
Patients presenting with multiple seizures in a 24-hour period were as likely to have seizure recurrence as those presenting with a single seizure, irrespective of etiology or treatment.
A recent survey looked at resuscitation practices that could help improve survival during in-hospital cardiac arrest
Exercise and the heart
Exercise increases the risk of sudden cardiac death (SCD) acutely.
Exercise decreases the risk of SCD in the long term.
Regular physical activity (even as little as 15 mins/day) reduces the risk of cardiovascular disease (CVD).
Up to 15% of MIs occur during or soon after vigorous physical exercise. This is typically in sedentary men with coronary risk factors.
In a 1993 study, in the first hour after heavy exertion, risk of heart attack rose more than 100-fold from baseline for habitually inactive persons. However, for frequent exercisers, this risk rose less than three-fold. Think of snow shoveling after a winter storm.
Both the Physicians’ Health Study and the Nurses’ Health Study show that the risk of SCD during exertion is reduced by habitual exercise.
If you are physically active, stay active. If you are not active, you should be because exercise has innumerable personal benefits. However, it is important to start gradually Some individuals at higher risk need to start under the guidance of a physician.
The terms and concepts of “waiver of informed consent’ versus “exception from informed consent” are often confused. Within the U.S., these concepts are not the same.
Bottom line:
Waiver of Informed Consent ≠ EFIC
These are the rules and regulations for the U.S. The regulations for emergency research in other countries may or may not be similar to these.
Can NIV be Used in ARDS?
Typically, if an infant or young child presents to the ED with concern for intracranial hemorrhage (ICH), CT is performed as a rapid diagnostic tool. Now that clinicians are more aware of the radiation associated with head CT, the possible use of ultrasound was studied. Ultrasound is commonly used in the neonatal population for detecting ICH. A study by Elkhunovich et al looked at children younger than 2 years who had cranial ultrasounds preformed. Over a 5 year period, 283 ultrasounds were done on patients between 0 to 485 days old (median 33 days). There were 39 bleeds detected. Ultrasound specificity and sensitivity was calculated by comparing the results with CT, MRI and/or clinical outcome. For significant bleeds, the sensitivity for ultrasound was 81%. The specificity for detecting ICH was 97%.
Only 2 patients in the study were older than 1 year. The proper windows are easiest to visualize in children younger than 6 months.
Bottom Line: The sensitivity of cranial ultrasound is inadequate to justify its use as a screening tool for detection of ICH in an infant with acute trauma, but it could be considered in situations when obtaining advanced imaging is not an option because of availability or patient condition.
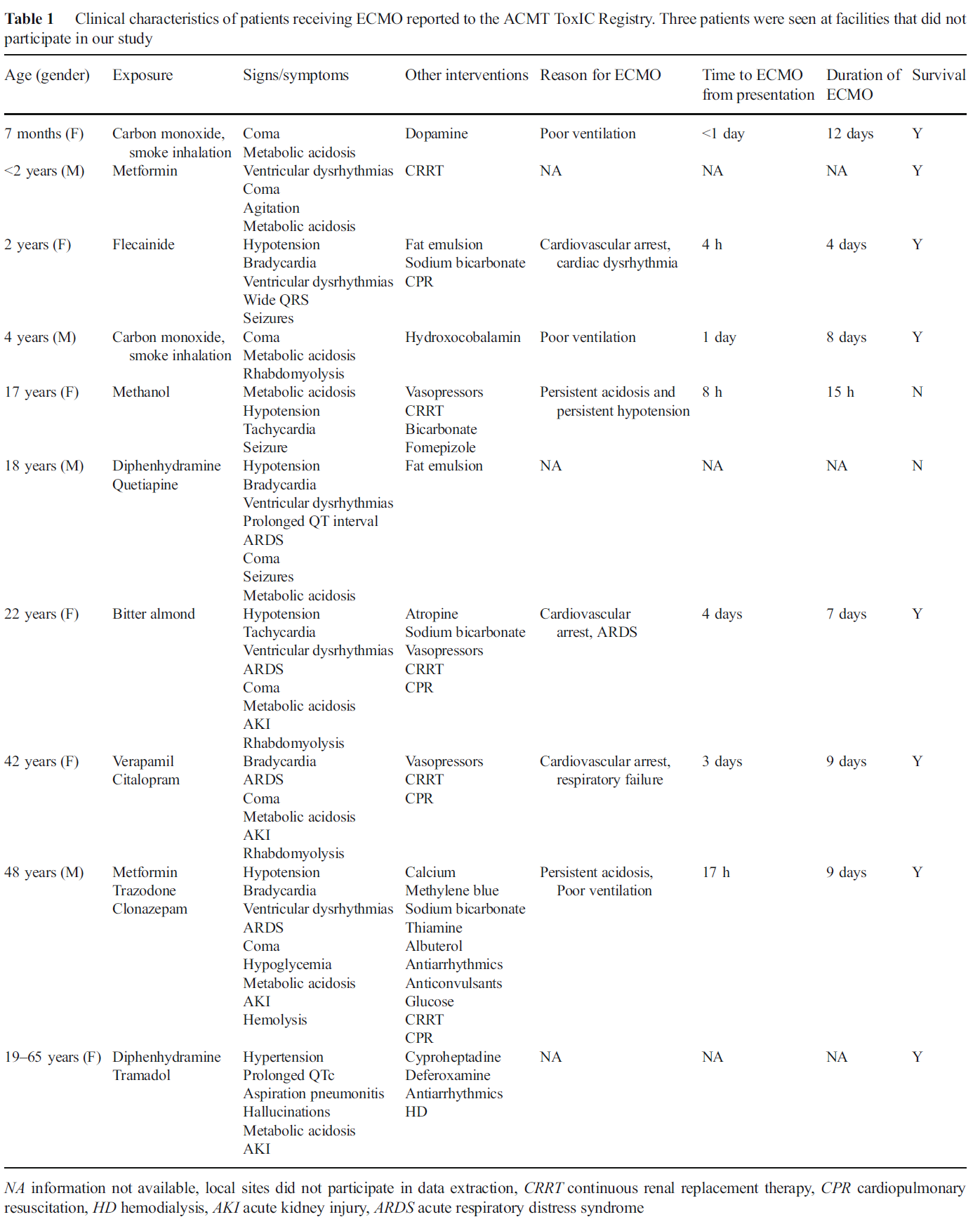
The American College of Medical Toxicology's ToxIC Registry is a self-reporting database completed by medical toxicologists across 69 insitutions in the US.
Application to Clinical Practice
In settings where ECMO is available, it may be a potential treatment option in severely poisoned patients. From the limited data, ECMO was generally administered prior to cardiovascular failure and might be of benefit particularly during the time the drug is being metabolized.
Table from the Case Series
What Do You Mean By Dizzy?
Table 1 shows common benign and serious causes of these vestibular syndromes.
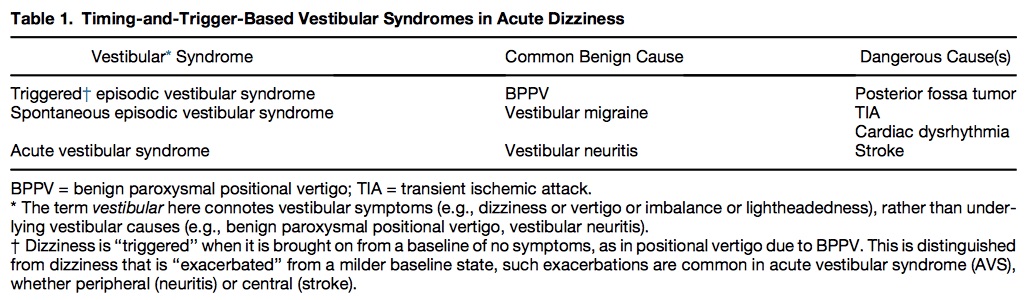
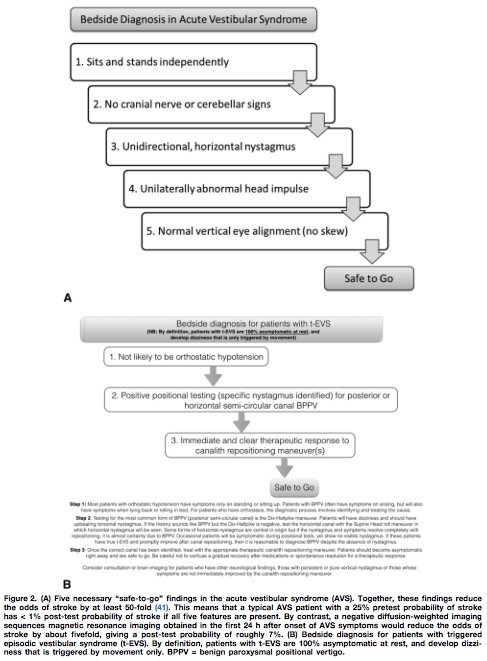
Utilizing the HINTS battery or the Dix-Hallpike maneuver, a “safe to go” algorithm for acute vestibular syndrome and triggered episodic vestibular syndrome is outlined in Figure 2.
Disclaimer: Talking about seizures/status that is NOT due to eclampsia
TAKE HOME: While no AEDs are completely safe in pregnancy, treatment and stabilization of maternal status epilepticus is paramount for fetal health. Involve neurology/epileptology and OB/maternal-fetal medicine.
Orthopedic documentation
1) Document location with specificity and laterality.
2) Document the location with as much specificity as possible
-Name of specific bone and specific site on bone (Shaft, head, neck, distal, proximal, styloid)
3) Document fractures as open/closed, displaced vs. non-displaced, routine or delayed healing,
-Orientation of fractures, such as transverse, oblique, spiral
- Document intra-articular or extra-articular involvement
4) For a particular injury, a complete note will include mention of the following
The joint above (e.g. for shoulder injuries this would be the neck, for hip injuries - the back)
The joint below
Motor (e.g. for arm injuries document the distal median, radial and ulnar motor innervation)
Sensory
Vascular
Skin (for all fractures document intact overlying skin esp. when covering with a splint)
Compartments (a simple mention of compartments are grossly soft/not tense will suffice)
*Especially relevant for forearm and tib/fib injuries
[CORRECTION]: Versed dose is 2-2.5 mg total not mg/kg
Patients with severe agitation present a unique challenge to the emergency department. Acute delirium is often due to psychostimulants such as cocaine, amphetamines, PCP, or synthetic cannabinoids, alcohol, or psychiatric illness. These patients require urgent evaluation necesssitating the use of physical and chemical restraints, not only for their own safety but also the hospital staff's. Fingerstick glucose, pulse oximetry, and vital signs must be expeditiously obtained. Severely agitated combative patients who are physically restrained are at high risk for morbidity from asphyxiation, hypermetabolic consequences (acidosis, hyperthermia, rhabdomyolysis), and death can occur.
Ketamine is phencyclidine derivative that causes dissociative state between the cortical and limbic systems which prevents the higher centers from preceiving visual, auditory, or painful stimuli. Ketamine has a wide safety profile and has been used worldwide for many years with few complications. It possesses ideal characteristics for rapid sedation of agitated patients:
Experience with Ketamine in patients with excited delirium has shown good initial control of agitation however, patients often require additional medications for deeper or longer duration of sedation. Benzodiazepines are recommmended as second line agents particularly intravenous or intramuscular Midazolam 2-2.5 mg /kg.
As noted previously, injuries cause substantial morbidity and mortality globally. How does it vary by age group?
The following table shows that unintentional injuries are the leading cause of death for individuals 1-44 years of age. Even when they are not the leading cause of death, injuries cause substantial mortality in all age groups.