HSV infection of the CNS is one of few treatable viral diseases. HSV encephalitis of older children and adults is almost always caused by herpes simplex virus type 1 (HSV-1), and in individuals older than 20, is due to HSV reactivation.
Temporal lobe localization is characteristic for HSV encephalitis in individuals older than 3 months, and is responsible for its characteristic presentation, namely bizarre behavior and expressive aphasia.
CSF analysis will usually reveal an elevated protein level, and a lymphocytic cellular predominance.
CSF protein concentration is a function of disease duration, and will continue to rise even with administration of treatment (acyclovir) and may remain elevated after the completion of therapy.
5% of CSF samples will be totally normal, and the diagnosis will only be revealed with positive PCR detection of viral DNA in the CSF, which is the gold standard for diagnosis.
The sensitivity of MRI is similar to CSF analysis, with 5% of patients with HSV encephalitis having a normal MRI on presentation, and subsequently developing abnormalities.
Of note, HSV-2 tends to cause aseptic meningitis rather than encephalitis in adults, and has a benign course.
Bottom Line? Keep a high index of suspicion for HSV encephalitis, and treat the patient empirically despite a normal CSF/MRI pending PCR results.
The EuroTherm3235 Trial was a randomized, multi-center trial to study hypothermia (32-35oC) in severe, traumatic brain injury1:
Quick pearl for those that are trying to complete their holiday shopping.
Mulder's sign is not a sign that there is an extra-terrestial in your ED, But rather a sign that your patient is suffering from a Morton's Neuroma (see pearl from 2012)
Patients will often complain of pain in 3rd and 4th intermetatarsal space and if you can reproduce the pain by compressing the metatarsal heads together then you have a Positive Mulder's sign. Check out the original pearl at https://umem.org/educational_pearls/1684/
Synthetic cathinones, known as bath salts, are a frequently used street drug in the United States. They have been discussed in a number of previous pearls. But from where did cathinone originate?
Khat (Catha edulis) is flowing plant native to the Arabian Peninsula and the Horn of Africa. It contains the monoamine alkaloid cathinone, which is an amphetamine-like stimulant that also causes euphoria. Historically, khat has been chewed for thousands of years and predates the use of coffee. Khat chewing is particularly popular in Yemen.
Khat contains many different compounds, which cause a number of different effects. Many of these effects are considered harmful to health. Khat chewing primarily impacts the central nervous system and the gastrointestinal system. However, it also has effects on cardiovascular, respiratory, endocrine, and genitourinary systems. In addition to the amphetamine like central nervous effects, other toxic effects include elevated blood pressure, tachycardia, insomnia, anorexia, constipation and general malaise.
Next time you see a patient with confusion and hallucinations from Yemen, Ethiopia, Somalia and other countries around the Horn of Africa, consider Khat in your differential.
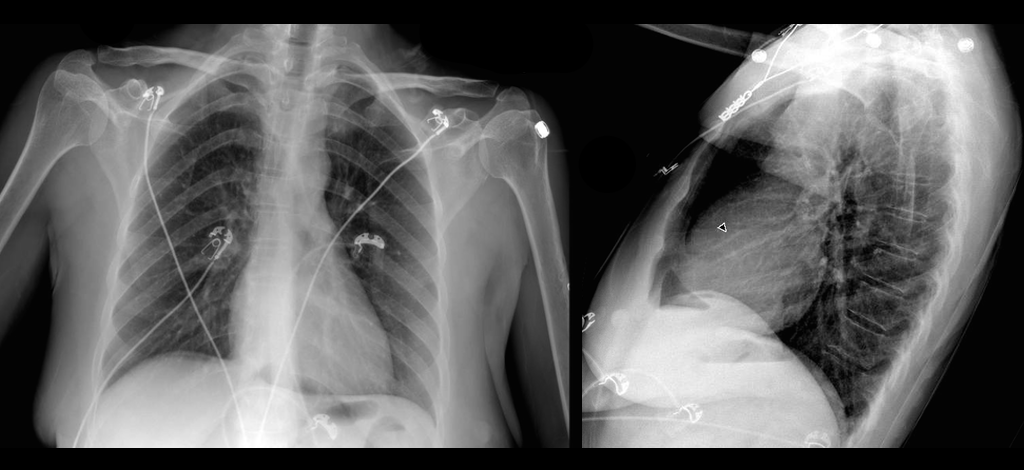
A patient arrives in acute respiratory distress with left sided chest pain. Ultrasound of the left anterior chest is shown; what's the diagnosis and name one false positive?
Parental Knowledge of pediatric concussion
Sample: Parents of children brought to pediatric hospital or outpatient clinics for evaluation of orthopedic injuries.
Participants scored an average of 18.4 (0-25) on knowledge and 63.1 (15-75) on Attitudes toward concussions.
Safest attitudes were seen in white females. Knowledge increased with income and education levels.
Parents from low income or education levels may benefit from additional education in the ED prior to discharge in addition to providing paper information which may not be read or understood.
The American Academy of Clinical Toxicology's Lipid Emulsion workgroup has published its first of 4 systematic reviews on the use of lipid emulsion in toxicology, this one on lipid's effect on laboratory analyses. [1] As expected, administering a fat bolus can significantly alter labs drawn subsequently.
The key point: If you are considering lipid for overdose, draw labs prior to giving it.
Which labs are affected? Most. Here's a helpful mnemonic courtesy of Dr. Kyle DeWitt.
Also remember to give lipid in its own line. It isn't compatable with most resuscitation drugs. [2]
A recent study compared the original NIHSS with the shortened 11, 8, and 5 item versions.4
Bottom Line: The original 15-item NIHSS should still be used to evaluate patients’ stroke severity.
The reliability of the NIHSS has been found to improve with personal and videotaped training.
The Bottom Line: This was a nicely designed study to evaluate the safety of both fluids. It does suggest that either fluid type is for the most part OK. But in patients requiring hefty fluid boluses, we should be cautious in what type of fluid we choose.

Tramadol has a reputation for being a safe, non-opioid alternative to opioids. Nothing could be further from the truth. Several blogs have published about the dangers of tramadol:
But what about seizure risk? Previous studies have been unable to confirm an increased seizure risk with therapeutic doses of tramadol (Seizure Risk Associated with Tramadol Use from EM PharmD blog). However, a new study refutes that premise.
22% of first-seizure patients had recent tramadol use!
This was a retrospecitve study without laboratory confirmation of tramadol intake. Nevertheless, it behooves us not to think of tramadol as a safer alternative to opioids. It is an opioid after all, and it comes with significant adverse effects.
Carbon monoxide (CO) is a colorless, odorless, tasteless toxic gas produced by incomplete combustion in fuel-burning devices and is a leading cause of poisoning morbidity and mortality.
Symptoms can be easily misinterpreted (e.g., headache, nausea, dizziness, or confusion) thus victims may not realize they are being poisoned.
CO detectors use an audible alarm and are effective in alerting potential victims of presence of CO. Some versions offer a digital readout of the CO concentration. Detectors are not a simple alarm level (as in smoke detectors) but are a concentration-time function.
In the UL 2034 Standard, Underwriters Laboratories specifies response times for CO alarms:
Current Occupational Safety and Health Administration permissible exposure limit for CO is 50 parts per million as an 8-hour time-weighted average concentration.
CO detectors have a limited lifespan of up to 7 years.
Forty percent of residential detectors studied failed to alarm in hazardous concentrations, despite outward indications that they were operating as intended.
CO detectors 10 years and older had the highest failure rates.
On a day when the 355th mass shooting this year in the USA occurred in San Bernardino, California, it seems appropriate to discuss gun violence.
A recently accepted publication in the American Journal of Medicine compared morality data from the USA to other high-income countries, and found the following:
The US homicide rates were 7.0 times higher than the aggregated rates of all other high-income countries.
The overall US suicide rate is average
Unintentional firearm deaths were 6.2 times higher in the US.
The overall firearm death rate in the US from all causes was 10.0 times higher.
Bottom line: As stated in the article: “The US has an enormous firearm problem compared to other high-income countries with much higher rates of homicide and firearm-related suicide.”
Mechanical Ventilation for Septic Patients in Resource-Limited Settings
Patient presents with right elbow pain after a fall. What's the diagnosis and what other injury should you look for?

Medial elbow pain is common among baseball pitchers and is also seen in other sports including football, javelin and gymnasts.
More than 97% of elbow pain in pitchers is located medially.
The ulnar collateral ligament of the elbow is an important structure in these patients.
http://www.aafp.org/afp/2014/0415/afp20140415p649-f3.jpg
While initially primarily seen in professional throwers, these injuries are now being seen in younger athletes.
Initially, patients may only note changes in stamina or strength of throws.
Later, they will note pain during the acceleration and follow through-phase of throwing
http://stlhealthandwellness.com/wp-content/uploads/2013/02/elbow03.jpg
The Valgus stress test for UCL deficiency is similar to the valgus test for the knee
https://www.youtube.com/watch?v=f6YvPSVk6G8
Treatment: splinting, ice, NSAIDs
Surgical indications: Failure of non-operative treatment with desire to return to same or higher level competition.
Ketamine has been the drug du jour for everything from agitation to pain, but status epilepticus?
Looking at the pathophysiology of seizures, they occur due to an imbalance between excitatory mechanisms (through glutamate at the NMDA receptors) and inibitory mechanisms (at GABA receptors). The mainstay for seizure treatment has been mostly potentiation of the inhibitory mechanisms, but why not inhibit the excitatory mechanisms at the NMDA receptors?
Ketamine is the only NMDA antagonist that has been investigated for refractory status epilepticus, mostly in retrospective small series, with only 3 prospective cohort studies, totaling to 162 patients (110 adults and 52 pediatrics). Variable results were recorded, from studies with complete response in all patients to complete treatment failure, with a total of 56.5% of the adult patients having electrographic response. The optimal bolus dose appears to be 1.5-4.5 mg/kg, with an infusion of up to 10 mg/kg/hour.
Bottom Line? Consider using ketamine in patients who are in refractory status - after benzodiazepines, a 2nd line agent (such as fosphenytoin, valproic acid or levetiracetam) and IV anesthetics have failed.
(NMDA: N-methyl-D-aspartate, GABA: -aminobutyric acid)
--The role of antibiotics in acute exacerbations of COPD remains controversial in many settings. However, a recent Cochrane review concludes that antibiotics have "large and consistent" benefit in ICU admissions [1]:
--However, patients on antibiotics had increased side effects, are at risk for increased drug-drug interaction (think azithromycin/levofloxacin), and the effect on multi-drug resistance is unclear.
--GOLD Guidelines are a bit more liberal with their recommendations for antibiotics [2], recommending antibiotics based on symptoms or in patients needing mechanical support.
--TAKEAWAY -- if your patient needs BiPAP or ICU, they should also get antibiotics!