BOTTOM LINE:
A 2024 meta analysis from the European Society of Anaesthesiology and Intensive Care and British Journal of Anaesthesia worked to develop joint guidelines for best practices for intubation of neonates and infants.
While this guide is focused primarily on anesthesia and operative care, several of the recommendations have practical application to the EM and ICU as well.
They focused on general guidance including ensuring appropriate anesthesia and analgesia during intubation. But also discussed that videolaryngoscopy with standard blades is the most appropriate first line for all intubations in this age group. It allows for appropriate visualization either directly or by video and for learners allows instructors to observe as well.
When there are difficulties with intubation, hyperangulated blades have very high success rates, but LMA and video assisted intubation with a fiberoptic scope are also appropriate next steps for securing an airway.
When intubating, uncuffed endotracheal tubes are acceptable in all infants though cuffed are also safe in infants over 3kg in weight.
Finally, while apneic oxygenation is regularly used in adults, it is also recommended in the neonatal period to avoid hypoxia.
TenCRAOS was a phase 3 randomized, multi-center, double blind, double dummy, placebo-controlled trial in 78 patients that showed no significant difference in visual outcomes at 30 days for IV tenecteplase 0.25 mg/kg compared to aspirin 300 mg alone within 4.5 hours of central retinal artery occlusion (CRAO) symptom onset. Tenecteplase was associated with more serious adverse events, one of which was a fatal intracerebral hemorrhage.
Bottom line: Although tenecteplase has theoretical advantages in CRAO, the results of this trial do not support routine use.
This systematic literature review looking at gender differences in trauma care reveals:
In a large, randomized trial conducted in 42 ICUs in France, high-flow oxygen did not reduce 28-day all-cause mortality in adult patients with acute hypoxemic respiratory failure when compared to standard oxygen support.
A modified 2 round Delphi study was used to create 57 learning objectives in geriatric care for European prehospital providers. Based on in-hospital learning objectives and literature, these experts came up with what appears to be a very reasonable and helpful list of education objectives for pre-hospital providers that could easily apply to emergency medicine learners as a whole. Here is their table:
https://link.springer.com/article/10.1186/s13049-026-01550-3/tables/3
In this retrospective cohort study looking at splenic injury management and outcomes in the UK, patients over age 65 had much higher mortality and were more often managed conservatively (vs splenectomy or embolization) despite having a lower splenic injury grade and lower overall injury severity score compared to those under 65. Many factors are possible here including frailty, reluctance to intervene in older patients, and lower mechanism of injury bias away from evaluation and management.
Looking at trauma patients evaluated at a major trauma center before and after EMS switched from semi-rigid to soft cervical collars for immobilization found no difference in adverse outcomes. Add this to the mounting evidence that our current practice of spinal immobilization may not offer any benefit.

The 2026 Acute Pulmonary Embolism Guidelines recommend a new approach to risk stratification of patients with acute PE, including measurement of at least one cardiac biomarker and serum lactate, evaluation of RV size and function with CTA or echo (preferred when feasible), and multidisciplinary PERT assessment for all patients with acute PE and elevated clinical severity scores to assist with further risk stratification.

Bottom Line: Swimming-Induced Pulmonary Edema (SIPE) AKA Immersion Pulmonary Edema is a rare, though life-threatening pathology associated with water-based activities, especially among athletes or military personnel. Caused by physiologic effects of immersion, not from aspiration/ingestion. Consider in any patient with respiratory distress or chest discomfort onset during water activities such as swimming, diving, etc. Diagnose with physical exam and POCUS. Manage supportively, potentially including positive pressure ventilation. Screen for alternative diagnoses.
See the link for more thorough review of assessment diagnostics, pathophysiology, pharmacological options, risk factors, and long-term considerations.
Bradycardia accompanying hypotension can be found in spinal cord injury (loss of autonomic reflex), beta blocker and calcium channel blocker overdose, intrinsic cardiac electrophysiologic derangement, and, often forgotten, intrabdominal hemorrhage. In the appropriate setting (blunt trauma, ruptured ectopic pregnancy), bradycardic hypotensive patients should be considered the same as tachycardic hypotensive patients and get a work up and treatment focused on Hemoperitoneum.
Using a database of 300,000 patients and applying a predictive measure for mortality, these authors found that patients over 66 with a high likelihood of 6 month mortality at the time of presentation were more likely to be admitted to an ICU when they presented to an ED. The authors conclude there is much work to be done regarding discussion of goals of care based on this information.
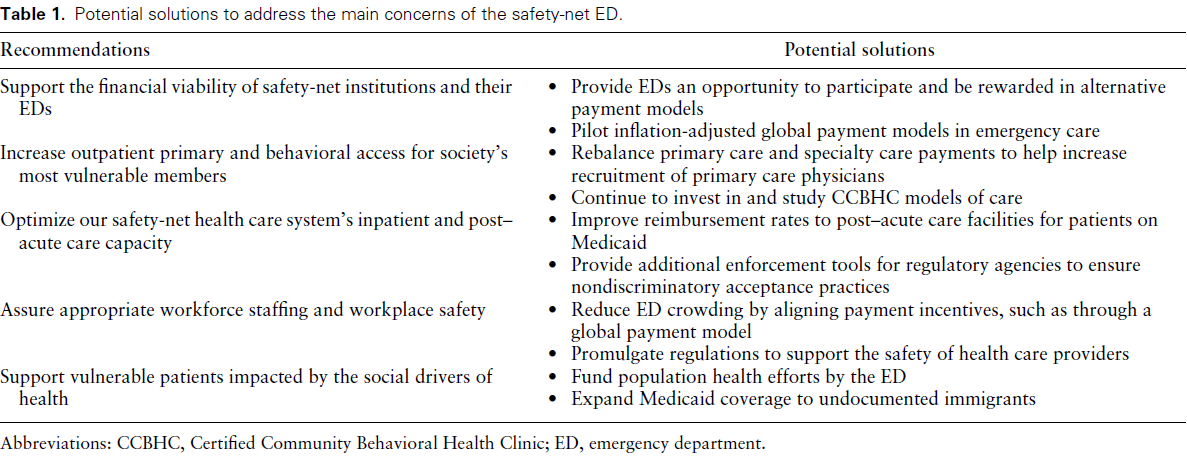
Bottom Line: Safety-net hospitals are those that see a substantial share of uninsured, Medicaid, or low-income Medicare patients. Their emergency departments (EDs) deliver disproportionally more undercompensated and uncompensated care, yet have similar operating costs as other EDs. Authors convened a group of 15 administrators of academic safety net EDs to identify and
develop a consensus understanding of barriers to delivering optimal care. See the link for details of their conclusions.
Click the link for below to read the bulleted, abridged version of the Executive Summary of the Updated SSC Guidelines for Adults with Sepsis and Septic Shock 2026…
Bottom Line: Among adult ED patients tested for gonorrhea and chlamydia, empiric treatment often does not align with confirmed infection. There are also notable sex disparities; in this study, females with confirmed infection were ~3.5 times more likely than males to not receive empiric treatment.
Looking at a national database, this study concluded the use of low titer O whole blood during trauma resuscitations was increasing at level one centers but not at level 2 and 3 centers. Is this a representation of the national blood supply as whole blood is harder to stock? We need to understand this trend to assure equal and appropriate care to trauma patients across the country.
Educational Pearls for the ED:
Many Muslim patients with diabetes will fast despite medical advice. Studies show a significant number continue fasting even when they are considered high risk.
Key medical risks during Ramadan fasting include:
- Hypoglycemia
- Hyperglycemia and diabetic ketoacidosis
- Dehydration
- Medication nonadherence or altered dosing schedules
This was review of 24 studies across 21 years that aimed to look at the complications associated with pediatric intubation in the hospital. The article also includes a list of all the articles with brief conclusions from each study for those interested.
Among a combined 7135 patients, there was an 84.7% overall success rate with a 30.1% rate of complication. There was a 69.8% first pass success rate. Desaturations < 90% was the most common complication followed by mainstem intubation. Studies also noted cardiac arrhythmia (55/3858 patients), hypotension (121/4536 patients) and cardiac arrest in 105/4836 patients). Other adverse events included esophageal intubation, surgical airway management and airway trauma.
Indications for intubation from most to least common are: neurologic, respiratory, trauma, cardiac arrest, sepsis, shock, cardiac failure and intoxication.
The debate of the best way to administer epinephrine in cardiac arrest continues. Pediatric arrests are different from adults in many ways, but some differences in arrest include 1) data supporting improved survival with early epinephrine administration and 2) less IVs are placed in children overall compared to adults making IO placement possibly quicker.
In this study, 739 patients were included with a median age of 1 year. The IO was used in 72% of patients and an IV was used in 27.6% of patients. There was no difference between survival to hospital discharge or prehospital ROSC between the two groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}