Radial and femoral arteries are common sites for arterial-line placement, but are not without complications (e.g., Radial artery: malfunction with positioning and Femoral artery: contamination and infection); an alternative site to consider is the axillary artery.
The axillary artery's superficial location and large size make it a desirable choice for cannulation.
The "anatomical-landmark" and "palpation" methods have been the traditional techniques of axillary arterial cannulation, however these methods may be difficult for to a variety of reasons (e.g., obesity, anasarca, arterial disease, etc.)
Ultrasound allows visualization of the axillary artery and avoids unintended injury to structures in close proximity (e.g., brachial plexus, pleura, axillary vein, etc.); please see figures 1 and 2 in the referenced Sandhu article and http://www.youtube.com/watch?v=Z31YiyV7cNQ.
A recent study (Killu, 2011) found that ultrasound increases success rates when compared to the traditional landmark approach.
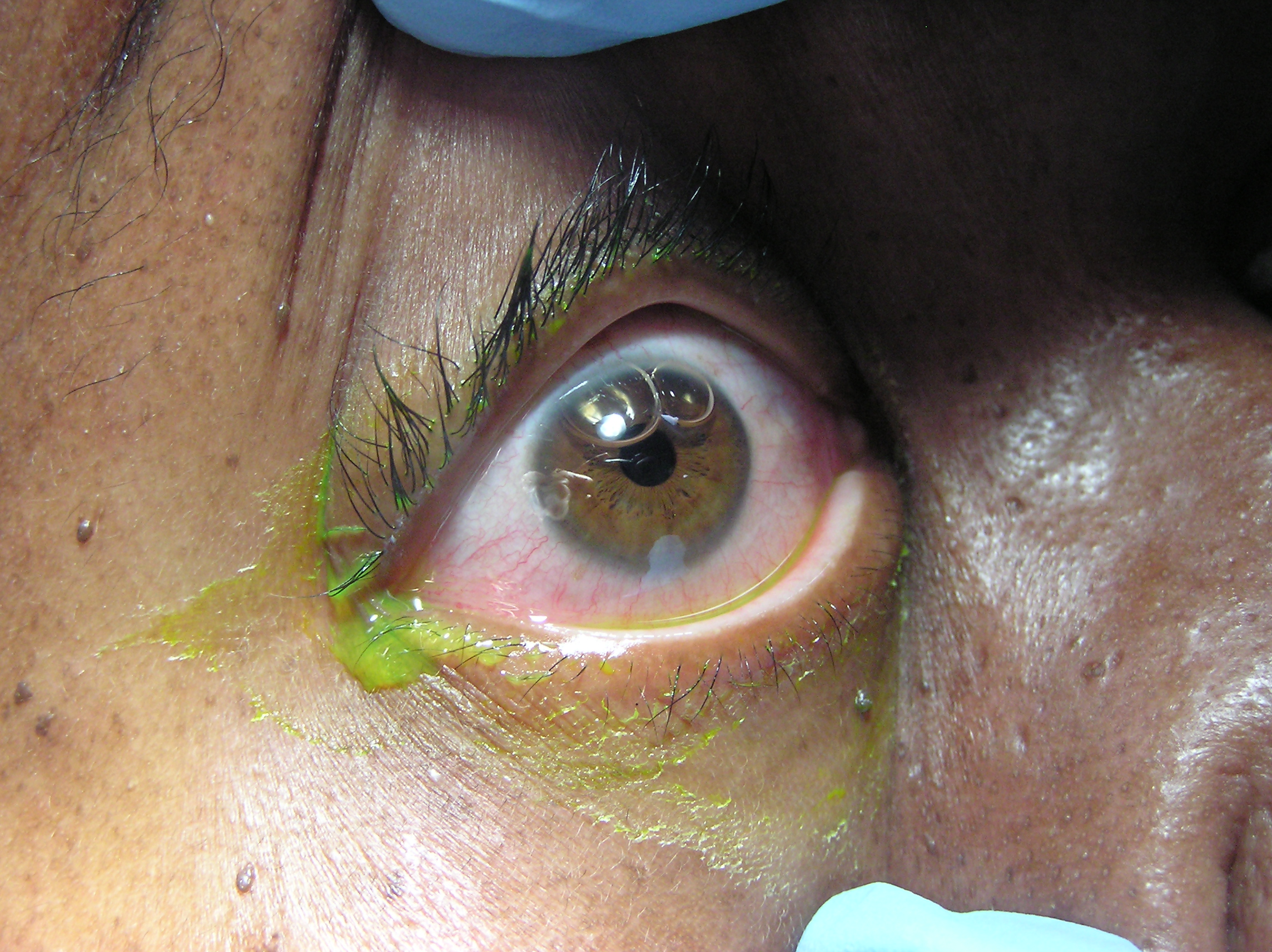
A 50 year-old patient presents after a self-inflicted eye injury. The patient had taken some type of needle and inserted it into their eye.
What is the diagnosis and what complications might result?
SVT is rarely, if ever, the presenting rhythm associated with an acute MI. As a result, physicians should not feel compelled to send troponin levels and perform rule-outs purely based on an SVT presentation. Instead, the decision to rule out a patient presenting with SVT should be based on whether there is a constellation of other concerning symptoms, exclusive of the SVT (e.g. if the patient presented with chest pressure radiating down the arm and diaphoresis, in addition to the SVT).
Two recent studies confirmed that routine troponin testing in patients with SVT is extremely low-yield, and instead often produces false-positive troponin results that lead to unnecessary admissions and workups. In other words, mild troponin elevations may occur in SVT but they do not correlate with true ACS.
Evaluation of circulatory status is the most important aspect of post reduction care.
Look for hard findings such as cool/cold lower extremity, diminished or absent pulses, pale or dusky skin, paralysis, etc.
However, the absence of these findings should not lull the clinician into a false sense of security. The degree of initial joint deformity, presence of full bounding pulses and warm skin over the dorsum of the foot can all be present in the setting of vascular injury.
The next step will be to perform an ABI (ankle-brachial index).
In one small study, no patient with an ABI greater than or equal to 0.9 had a vascular injury.
Patients with a reassuring physical exam and ABIs should be admitted for vascular checks without further imaging.
Patients with a reassuring physical examination but with an abnormal ABI should have an imaging study obtained (arteriogram/CT angiogram).
Patients with hard findings of a vascular injury should have an emergent vascular surgery consultation.
Every so often a patient arrives in PSVT with their only intravenous access being through a hemodialysis port.
Initial dose of adenosine should be reduced to 3 mg if administered through a central line. Remember a central line delivers the adenosine right where you need it. This recommendation is supported by the 2010 ACLS guidelines. Second and third doses should be 6 mg (instead of 12 mg).
Cases of prolonged bradycardia and severe side effects have been reported after full-dose adenosine through a central line. Other situations to consider lower doses include patients currently receiving carbamazepine or dipyridamole or in those with a transplanted heart.
Fungal Sepsis in the Critically Ill
Approximately 7-10% of cases of ACS are not related to atherosclerotic coronary disease. Some other causes of ACS include the following:
trauma
vasculitis
congenital abnormalities
emboli (e.g. bacterial)
thoracic aortic dissection
infectious diseases
DIC, TTP
These conditions can produce ST-segment changes that resemble those of true STEMI or non-STEMI, and therefore some of these patients are diagnosed retrospectively after a negative catheterization.
Sugar Tong Splint
The sugar tong splint is ideal for splinting fractures of the radius, ulna, or wrist. It prevents flexion and extension at the wrist, limits flexion and extension at the elbow, and prevents supination and pronation. A posterior long arm splint does not prevent supinaton and pronation, therefore, it is of limited use for radius and ulna fractures.
The traditional sugar tong can be difficult to put on a patient without an assistant as it is often hard to hold the splint in position as you begin to ace wrap it. A variation on the sugar tong, the reverse sugar tong, prevents this frustration. The splinting material is cut so that a small piece suspends the splint from the web space between the thumb and index finger. The open ends at the elbow are also easily folded under each other, preventing any bulky splint material from extending out.

The reverse sugar tong is on the left, the original sugar tong on the right.
Check out this video showing how to place a reverse sugar tong splint.
http://www.youtube.com/watch?v=r-RHdttOMf0
Multiple methods of confirming endotracheal tube placement exist, however quantitative waveform capnography is the most reliable method. Unfortunately this may not be immediately available at all medical centers.
Recent studies demonstrate that bedside ultrasound may assist in the detection of proper endotracheal tube placement.
The T.R.U.E. (Tracheal Rapid Ultrasound Exam) was demonstrated to be 99% sensitive, 94% specific, 99% PPV, and 94% NPV during intubation.
The basic exam involves placing a high-frequency linear-array probe on the anterior neck above the sternal notch and identifying the trachea and esophagus during intubation.
The following video is an example of what you DO NOT want to see during an intubation: http://www.youtube.com/watch?v=LvfThxhQ93A
Patient presents with right-sided chest and shoulder pain....
What's the diagnosis?

If you're like me, you've been a bit confused about what exactly defines "coma" in the current recommendations for post-arrest hypothermia in "comatose" patients with return of spontaneous circulation. Fortunately, a recent NEJM article has helped clarify this by suggesting that hypothermia should be induced in these post-arrest patients with either:
Naturally, if the patient was comatose before the arrest, don't bother.
Stability from 4 major ligaments (ACL, PCL, MCL and LCL)
Knee dislocation causes injury to multiple ligaments (usually 3 of the above).
Many of these dislocation spontaneously reduce prior to medical evaluation. Therefore, consider knee dislocation in a patient with multi ligament injury, significant hemarthrosis and bruising.
Vascular injury in up to 40% (popliteal artery)
Nerve injury in up to 23% (peroneal nerve) ((ankle dorsiflexion and sensation to the first web space of the foot))
After reduction, immobilize knee in 15-20 degrees flexion.
The degree of initial deformity, presence of strong pulses, or warm skin cannot be used to rule out popliteal injury.
End Tidal CO2 continuous capnography is being utilized more in the ED for procedural sedation. One of the best studies is a randomized control trial using propofol that showed you could see signs of hypoventiliation prior to hypoxia by about 60 seconds - which can be plenty of time to get your BVM and airway cart ready.

