Sedation for the Mechanically Ventilated Adult ICU Patient
This study looked at exposure to gun violence and found increased use of mental health resources, depression and suicide risk even with a single exposure. Repetitive exposure increased suicide risk as well as mental health service utilization, depression and overall health service utilization. While further work is needed, screening our patients for gun violence exposure could undercover mental health needs.
In the April edition of Annals of EM, there are opposing view points on the optimal antibiotic regiment for necrotizing soft tissue infection. One group proposes linezolid alone will cover all the worrisome pathogens namely group A Strep and Staph. There are less side effects including C. Diff infection with this medication. Another group suggests sticking to vancomycin plus/minus BLactam along with clindamycin. Their arguement centers around clindamycin is useful as an antitoxin more so than its antibacterial property.
Both offer reasonable evidence and neither is compelling enough to say one is superior to the other.
Pseudo-Brugada pattern in hyperkalemia
Category: ECG
By: Chuck Siegel
Keywords: Brugada sign, hyperkalemia, ECG, arrhythmia
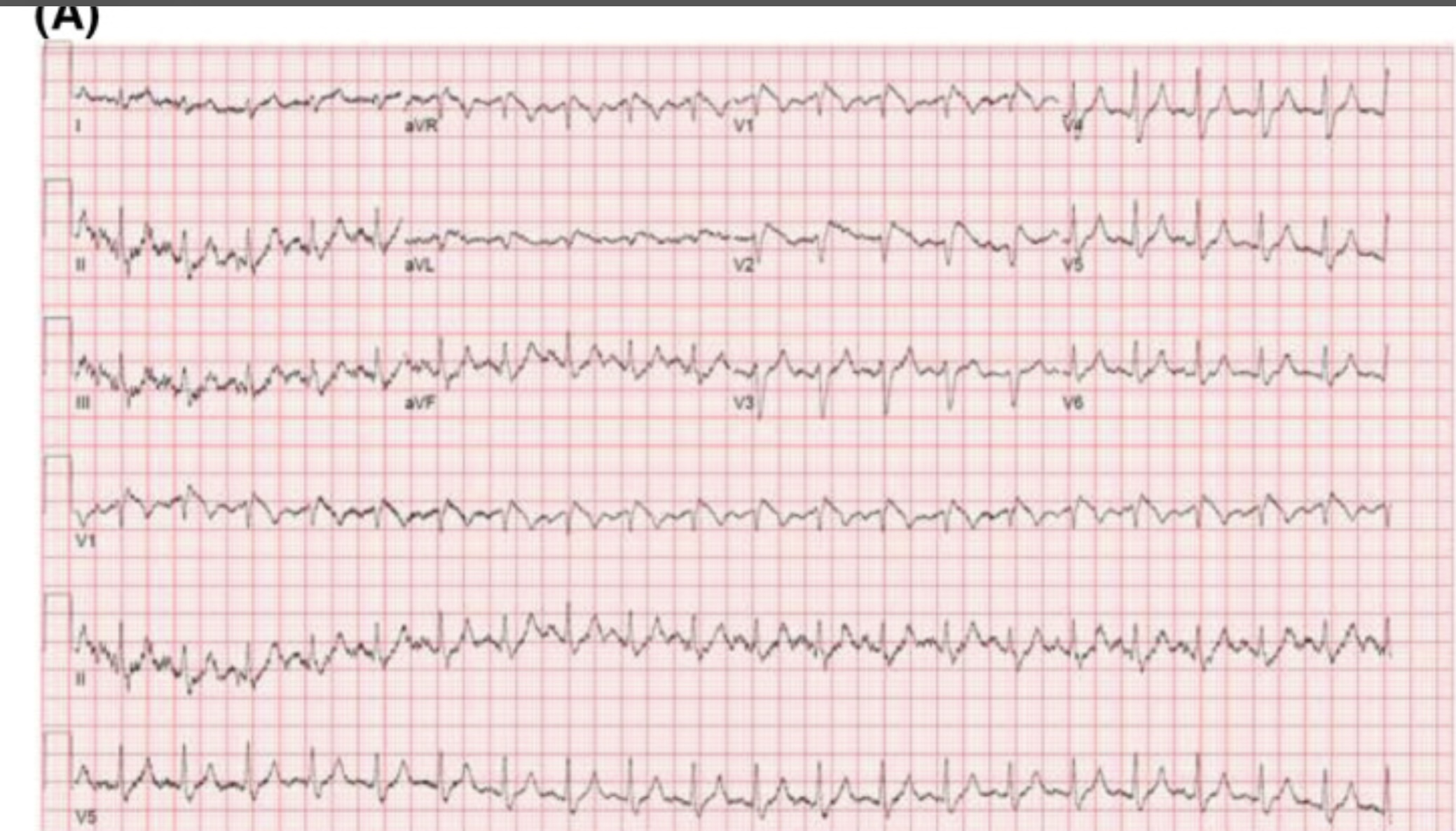
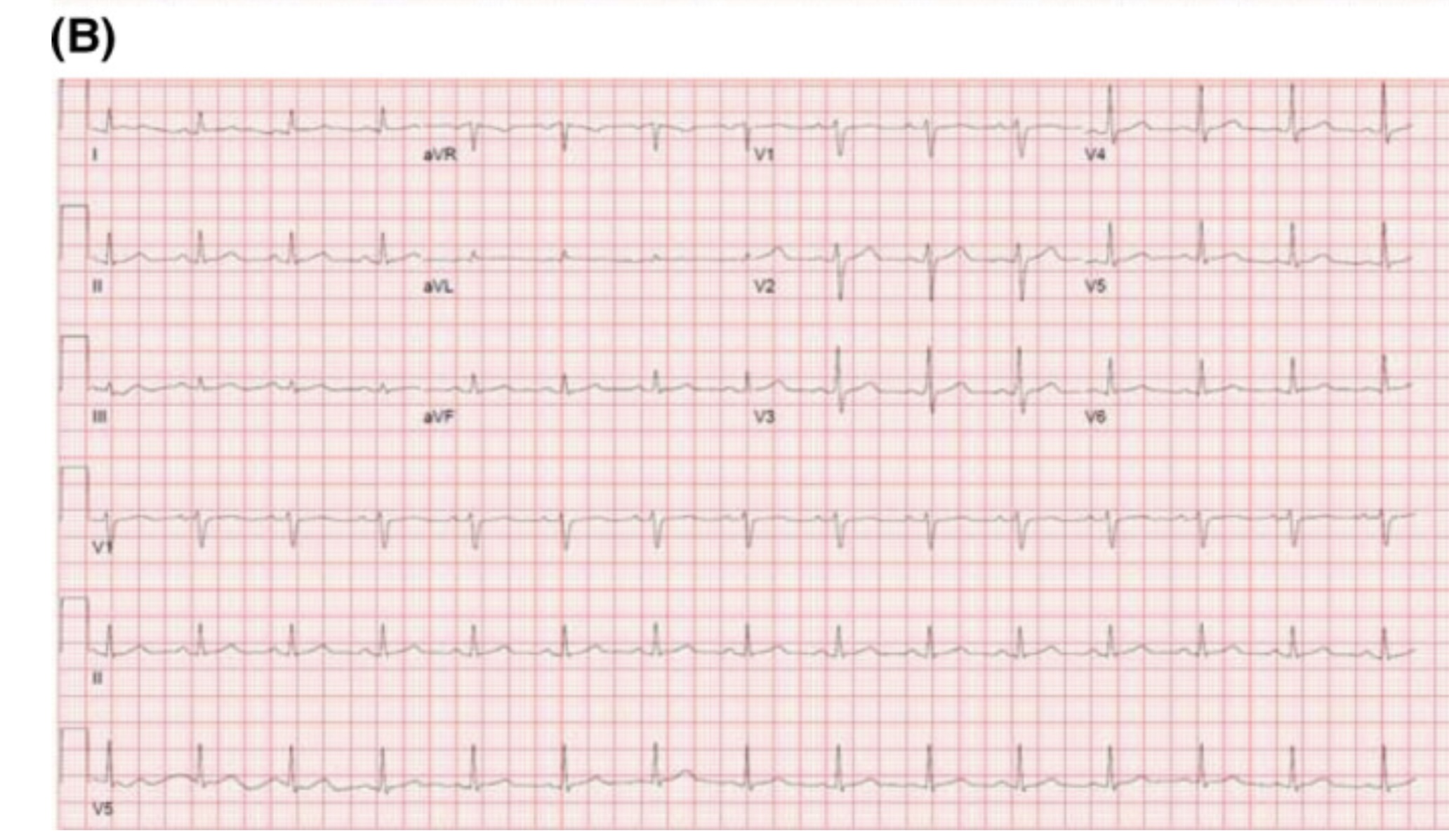
Hyperkalemia can produce a variety of ECG changes, including well-known changes such as peaked t-waves, QRS widening, PR-interval prolongation, loss of the p-waves, and the sine wave morphology. One change not as commonly seen is coved ST-elevation in V1-V3 that mimics the ECG changes associated with Brugada sign. Unlike Brugada syndrome, these ECG changes are transient and resolve upon treatment of the hyperkalemia.
The mechanism of these ECG findings relate to the elevated extracellular potassium’s inactivating effect on sodium channels, similar to the sodium channelopathy found in Brugada syndrome. The mean serum potassium concentration of reported cases is often above 6.5 mEq/L. Importantly, hyperkalemia-induced Brugada pattern has not been associated with sudden cardiac death or ventricular arrhythmias.
An example of a hyperkalemia-induced pseudo Brugada pattern in a patient with a K of 7.2 mEq/L (A) as well as that same patient’s ECG following treatment of their hyperkalemia (B).
You may have seen the headline.
93 million CT examinations conducted on 62 million US patients in 2023 projected to lead to 103000 new cancer diagnoses accounting for 5% of new cancers.
The details of the modeling can be found here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832778.
What does this have to do with administration?
The solutions rely on administrative involvement:
There’s an editorial here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832782 and a commentary with interviews that put the findings nicely in context here https://arstechnica.com/health/2025/04/ct-scans-could-cause-5-of-cancers-study-finds-experts-note-uncertainty/ (including pointing out that lifetime risk of cancer in the US is 40% and the increase from CT scanning on the order of 0.1% / scan).
This large RCT compared High-Flow Nasal Oxygen (HFNO) against Noninvasive Ventilation (NIV) via face mask in 5 types of Acute Respiratory Failure (ARF): non-immunocompromised hypoxemia, immunocompromised hypoxemia, COPD with acidosis, acute cardiogenic pulmonary edema (ACPE), and COVID-19.
Bottom Line:
RENOVATE suggests HFNO might be a reasonable, more comfortable initial choice for non-immunocompromised hypoxemic ARF or COVID-19 ARF. However, exercise caution using HFNO first-line for COPD exacerbations with acidosis or immunocompromised hypoxemic ARF due to conflicting analyses and potential harm signals. The signal for HFNO benefit in ACPE is intriguing but needs confirmation before changing practice. Close monitoring for failure and timely escalation are essential regardless of the initial noninvasive strategy.
This study looking at the type of facility that cared for rural injured patients reminds us that the majority of trauma care for rural patients occurs in non-trauma centers. This included some of the most severely injured and for many definitive care was received at these centers.
This may lead to lack of inclusion in trauma registries and under valuing the care being delivered by non-trauma centers. Protocols to facilitate transfers, air medical protocols and availability along with tele-health all are important in rural trauma care. Non-trauma designated centers are a critical part of the trauma network for rural residents and their value can not be ignored.
This study was the first look at the author's experiences with racial disparities in head and neck trauma in children. It looked at community EDs, and found that white children were more likely to be diagnosed with concussion compared to black children. White children were more likely to be seen as a result of sports or motor vehicle accidents, while black children were more likely to be seen as a result of an assault.
This study revealed the need for further research into the cause of the disparities in care that they identified.
Have you been wondering what the latest pediatric emergency medicine lecture says?
See the attached table from this review which highlights the 10 top articles from 2024 with their key findings!
Pulseless electrical activity (PEA) is the initial rhythm in up to 25% of out of hospital cardiac arrests.
This paper is a systemic review and analysis examining if the rate or width of the initial PEA qrs complex was associated with survival. The qrs complex was either wide (>= 120 ms) or narrow (<120ms) and a frequency of fast (>= 60/s) or slow (<60/s). 7 studies including 9727 patients were included. Analysis showed:
- mortality was higher in the wide qrs group compared to narrow
- mortality was higher in the slow PEA rate compared to fast
- neurological outcome was better in patients with a fast PEA rate compared to slow.
Emergency contraception comes in multiple forms, all of which have their own side effects and best case use scenarios that emergency medicine providers should be aware of to offer the best counseling.
Consider your patient before advising - if their BMI is > 25, consider ulipristal. If they want the most effective method, that'll be a copper IUD - but make sure they can get an appointment within 5 days of the unprotected intercourse! If they cannot afford ulipristal or levonorgestrel (which can both be $50 without insurance), but they already have OCPs, combining OCPs to the total noted above can be a method of emergency contraception that is still very effective.
Background:
Acetaminophen can reduce hemoprotein induced oxidative damage. There has been growing discussion about its benefits in critically ill patients with sepsis. Multiple observational studies have found conflicting results on mortality in critically ill patients with sepsis. The ASTER trial found no difference in number of days alive and free of organ support. Interestingly their secondary outcomes found significantly less development of ARDS in the acetaminophen group 2.2% vs 8.5%, p = .01. There was also a non-statistically significant difference in mortality between the groups in favor of the acetaminophen group, 17% vs 22% p = 0.19. This study looked to further evaluate if acetaminophen used in critically ill patients with sepsis would have a decrease in mortality and increase in ventilator free days.
Study:
- Retrospective analysis of the Ibuprofen in Sepsis Study (ISS)
- The ISS was a randomized clinical trial comparing ibuprofen with placebo in critically ill patients with sepsis. Careful documentation of Acetaminophen use was recorded for the trial
- Critically-ill adults across 7 ICU’s in the US and Canada with known or suspected infection and severe organ dysfunction
- Acetaminophen use within 48 hours of enrollment = Acetaminophen exposed
- Primary outcome: 30-day mortality
- Secondary outcome: Renal failure and ventilator free days up to day 28
- 455 patients. 172 Acetaminophen unexposed, 235 Acetaminophen exposed.
Results:
- Propensity-matched analysis showed a lower mortality risk at 30 days in patients exposed to acetaminophen compared to unexposed, 32% vs 49% (HR 0.58, p .004)
- Secondary outcomes found acetaminophen exposed group had more ventilator free days (p .02) but there was no difference in renal failure among the groups.
Limitations:
- Major risk for confounding variables
- Retrospective and the data used was from decades ago (1989 -1995). Sepsis care has evolved and improved since this time
- Dose and frequency of acetaminophen administration was not standardized
Take Home Points:
- Interesting research that provides further support on the possible benefit to using acetaminophen in the management of critically ill patients with sepsis.
- With the ASTER trial showing a signal for the decrease in development of ARDS and this study showing improvement in mortality one could make a case for starting acetaminophen early in the course for these patients. However, the data is conflicting and more prospective, RCT’s are needed to confirm these findings before making this a staple for sepsis care in critically ill patients.
This study looked at pre-trauma mental health diagnosis (from medical records) and post-trauma mental health symptoms as assessed by survey. The majority of patients suffered blunt trauma and mean age was 67. Having pre/traumatic mental health diagnosis and particularly post-traumatic symptoms lead to worse health outcomes and financial conditions. Further work needs to be done to assess how to improve mental health symptoms post-traumatic injury.
Non benzodiazepine muscle relaxants
Muscle relaxants were the most commonly (32%) prescribed medication upon discharge from the ED for lower back pain.
Muscle relaxants, such as cyclobenzaprine, provide short term pain-relief for patients with acute low back pain compared to placebo.
There is little difference in efficacy among the various muscle relaxants.
Evidence for muscle relaxants for back pain is weak compared to NSAIDs, so limit use to patients who have contraindications to NSAIDS.
There is no strong evidence that combination therapy with NSAIDs is more effective than NSAIDs alone.
If using during the day, consider using a lower dose (cyclobenzaprine 5mg) and a higher dose at night (10mg).
If treating with NSAIDs, consider using only at night to promote sleep.
Also, limit use to those patients who can tolerate the side effect profile of muscle relaxants, which include anticholinergic effects, dizziness, and sedation.
Risks of these agents increase with age, so should be used with caution in older adults.
Often given to this population due to fears of NSAID side effects.
Presentation:
JME is a common cause of juvenile/adolescent seizures.
Patients typically present between 12-18 years of age with a combination of myoclonic movements, absence seizures and generalized tonic-clonic seizures.
This diagnosis is often mistaken for morning clumsiness due to the myoclonic movements and asking about myoclonic movements can help make the diagnosis.
Diagnosis:
Diagnosis is primarily based on history. Myoclonic seizures are required to make the diagnosis. Patients with consistent history can receive outpatient EEG to confirm the diagnosis.
No ED images or tests needed with the correct clinical history and return to baseline. (even outpatient with appropriate history imaging is not needed as it is usually normal)
Treatment:
Valproic acid is typically the treatment of choice for patients though must be used with caution in women of childbearing age. Other common treatment options include levetiracetam and lamotrigine. With the correct clinical history, these can be started in the ED.
Be sure to discuss good sleep hygiene and avoidance of alcohol with patients as these can be triggers.
Albuterol, a common bronchodilator used in the treatment of asthma and chronic obstructive pulmonary disease (COPD), can cause a surprising increase of lactate levels. The increase in lactate is usually mild to moderate (typically < 4 mmol/L) and transient. It does not necessarily indicate underlying sepsis, tissue hypoxia, or severe metabolic acidosis.
Mechanism:
Albuterol can cause a transient increase in lactate levels due to its beta-2 agonist effects, which promote glycogenolysis and increase anaerobic metabolism. This can result in elevated lactic acid production, even in the absence of tissue hypoxia or shock.
Timing:
This effect is typically seen within 30 minutes of albuterol administration and can persist for 1-2 hours after discontinuing treatment.
Monitoring:
If lactate levels are elevated in a patient receiving albuterol, consider the possibility of a pharmacologic cause rather than immediately assuming a more serious etiology like shock or severe metabolic disturbance.
Differentiating Causes of Elevated Lactate:
In a critically ill patient, elevated lactate can indicate hypoperfusion (e.g., septic shock, cardiogenic shock, or hypovolemic shock). However, when elevated lactate is associated with albuterol administration, the rise in lactate is often lower and resolves without intervention.
Management:
If albuterol-induced lactate elevation is suspected, continue with supportive care and monitor lactate trends. No specific treatment is necessary for the elevated lactate unless there are other concerning clinical findings that suggest a different underlying cause.
Conclusion:
In emergency settings, it's important to recognize that albuterol can cause a transient increase in lactate levels. Understanding this phenomenon can help avoid misdiagnosis and prevent unnecessary interventions in patients receiving albuterol therapy. Always correlate lactate levels with the broader clinical picture to guide management decisions.
Flow rates are, in theory, determined by Poiseuille’s Law, which states that the flow rate depends on fluid viscosity, pipe length, and the pressure difference between the ends of the pipe .
Of course we won’t be calculating this during a resuscitation! Nor would it be useful if we did: the equation assumes laminar flow, whereas turbulent flow is more likely. Nor is it practical to look up the viscosity of crystalloid/blood/plasma, which also dramatically impacts flow rates.
Instead, remember this equation: Larger + shorter = faster
And keep in mind the following:
In practice, our friends in Australia actually put common catheters to the test, and provided these helpful results:
Or, as a picture:
Note, these flow rates were achieved using crystalloid. Blood will be slower due to higher viscosity.
Do you ever tell your patients to “follow up with your primary care physician in 3-5 days”? How many of them actually do it? And does it make a difference?
Study Overview:
This study is a retrospective analysis of 28,085 adults (?20 years) presenting with acute abdominal pain (AAP) at 15 German emergency departments (EDs) in 2016.
Key Findings:
Hospitalization rate:
39.8% were admitted to the hospital from the ED.
Outpatient Care (OC) Before ED Visit:
33.9% had an OC visit within 3 days before their ED visit.
Of these, 48.6% were hospitalized.
Outpatient Care After ED Visit:
62.7% had OC follow-up within 30 days.
Factors Increasing Hospitalization Odds:
Age ?65 years: aOR 3.05
Prior OC: aOR 1.71
Male sex: aOR 1.44
In-Hospital Mortality:
3.1%
ED Re-visits Within 30 Days:
More likely in age ?65: aOR 1.32
Less likely with prior OC: aOR 0.37
Conclusion:
Acute abdominal pain in the ED is associated with high hospitalization and mortality rates, especially in older adults and those with prior outpatient visits. Prior outpatient contact is linked with both increased admission likelihood and reduced risk of ED re-visits, highlighting its complex role in care continuity. Improving outpatient care access and coordination may reduce ED burden and enhance outcomes for AAP patients.
While there are other factors to consider ie the health care system and its infrastructure, this does provide some interesting food for thought about what happens when we discharge patients.
A recent systematic review and meta-analysis evaluated the diagnostic accuracy of ultrasound in detecting acute diverticulitis. The analysis included 12 studies with a total of 2,056 patients. Ultrasound demonstrated a sensitivity of 92.5% (95% CI: 86.9%–95.8%) and a specificity of 87.7% (95% CI: 75.7%–94.2%).
The most commonly used diagnostic criteria across the studies included:
Similar to prior research on POCUS for nephrolithiasis, these findings support a POCUS-first approach for patients at low risk for serious alternative diagnoses. Ultrasound is a great alternative for patients with contraindications to contrast-enhanced CT, such as those with contrast allergies.
As the authors state, while ultrasound may be effective in identifying acute diverticulitis and its complications, such as abscess, additional imaging with CT may still be required to assess the severity of complications.
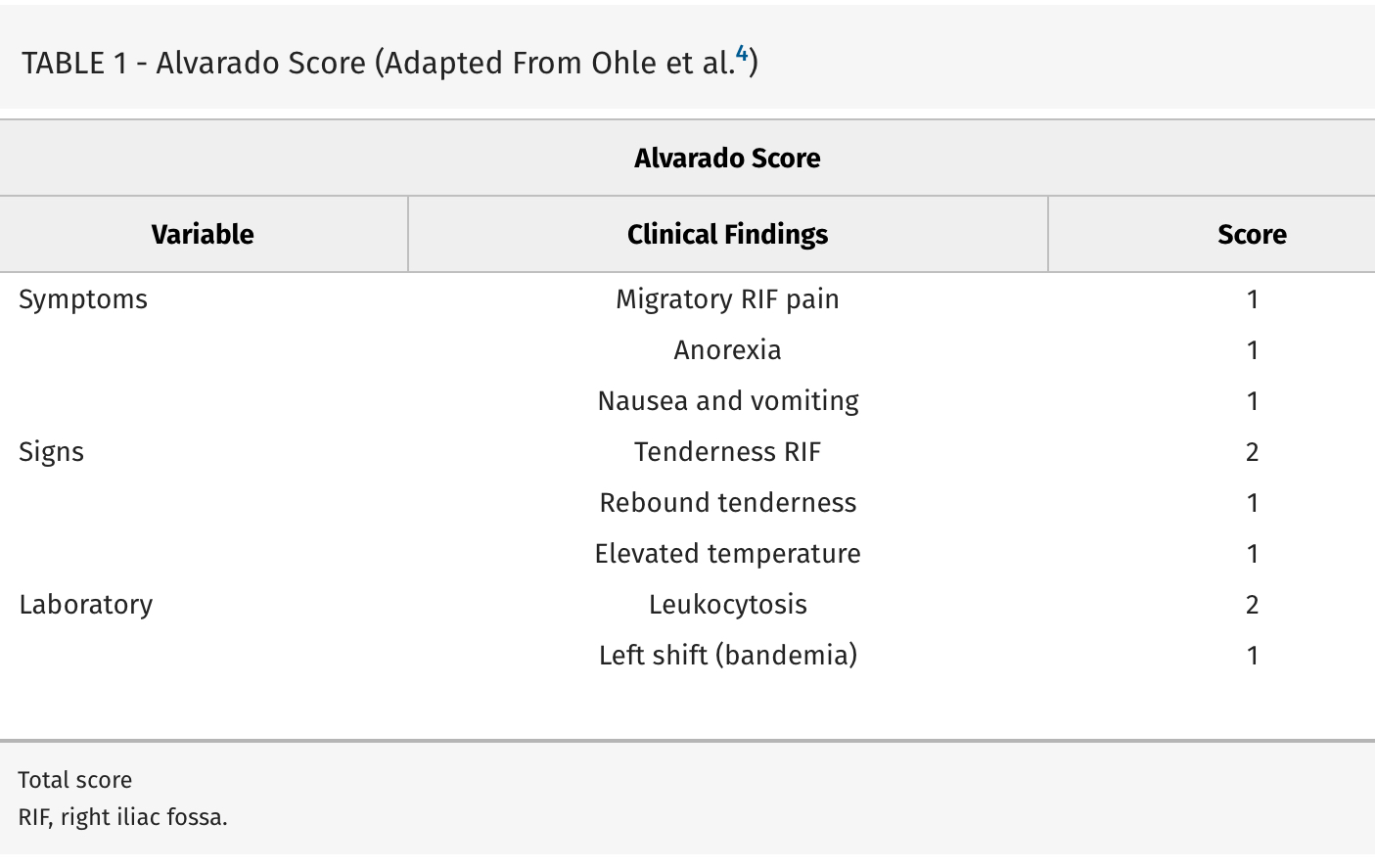
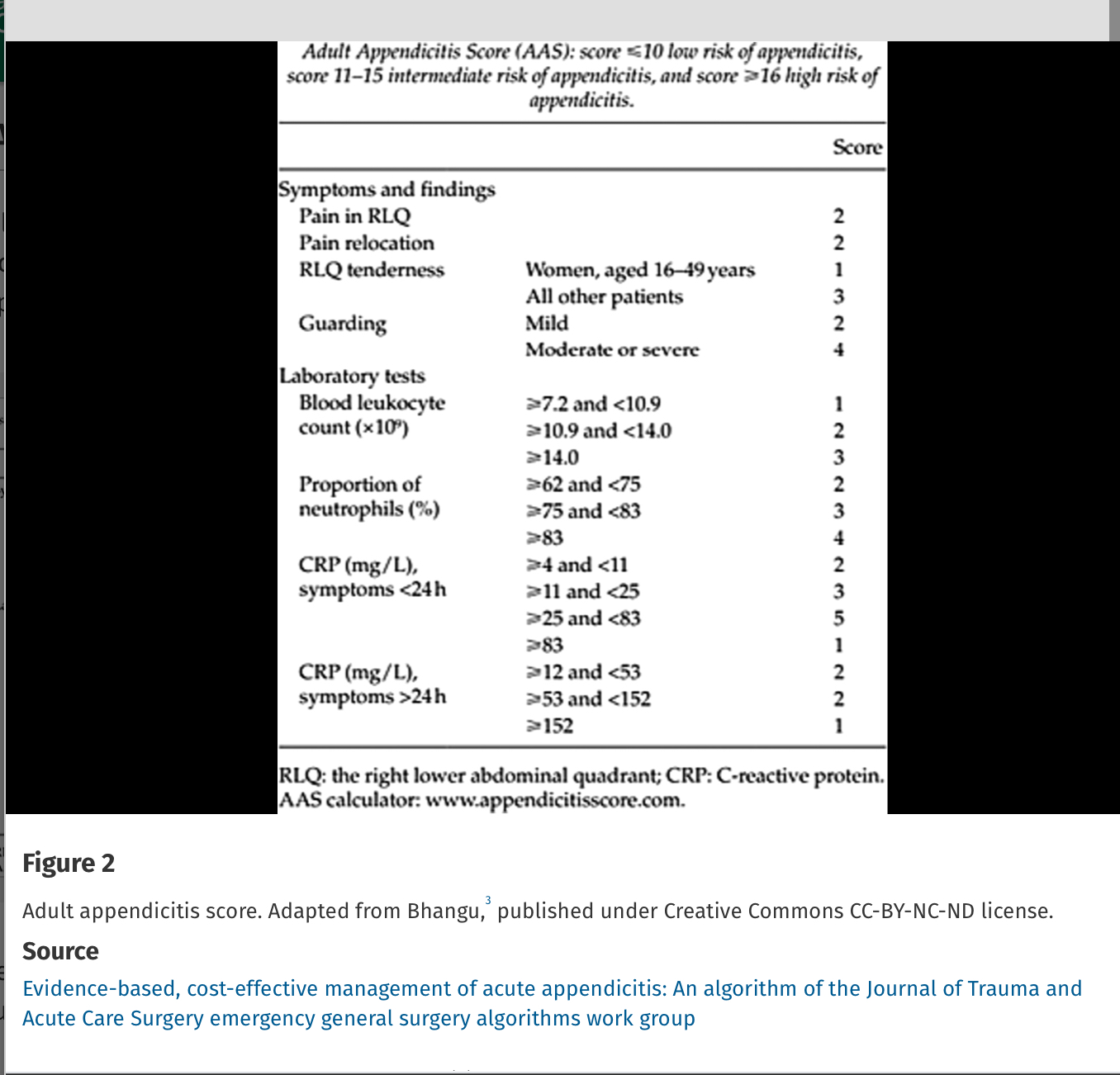
Missed appendicitis leading to rupture and peritonitis leads to morbidity, mortality, and malpractice claims. Part of a longer article looking at evaluation and management of appendicitis, these authors provide three scoring systems that can be used to identify appendicitis. Use of these scores can guide imaging and surgical consultation.
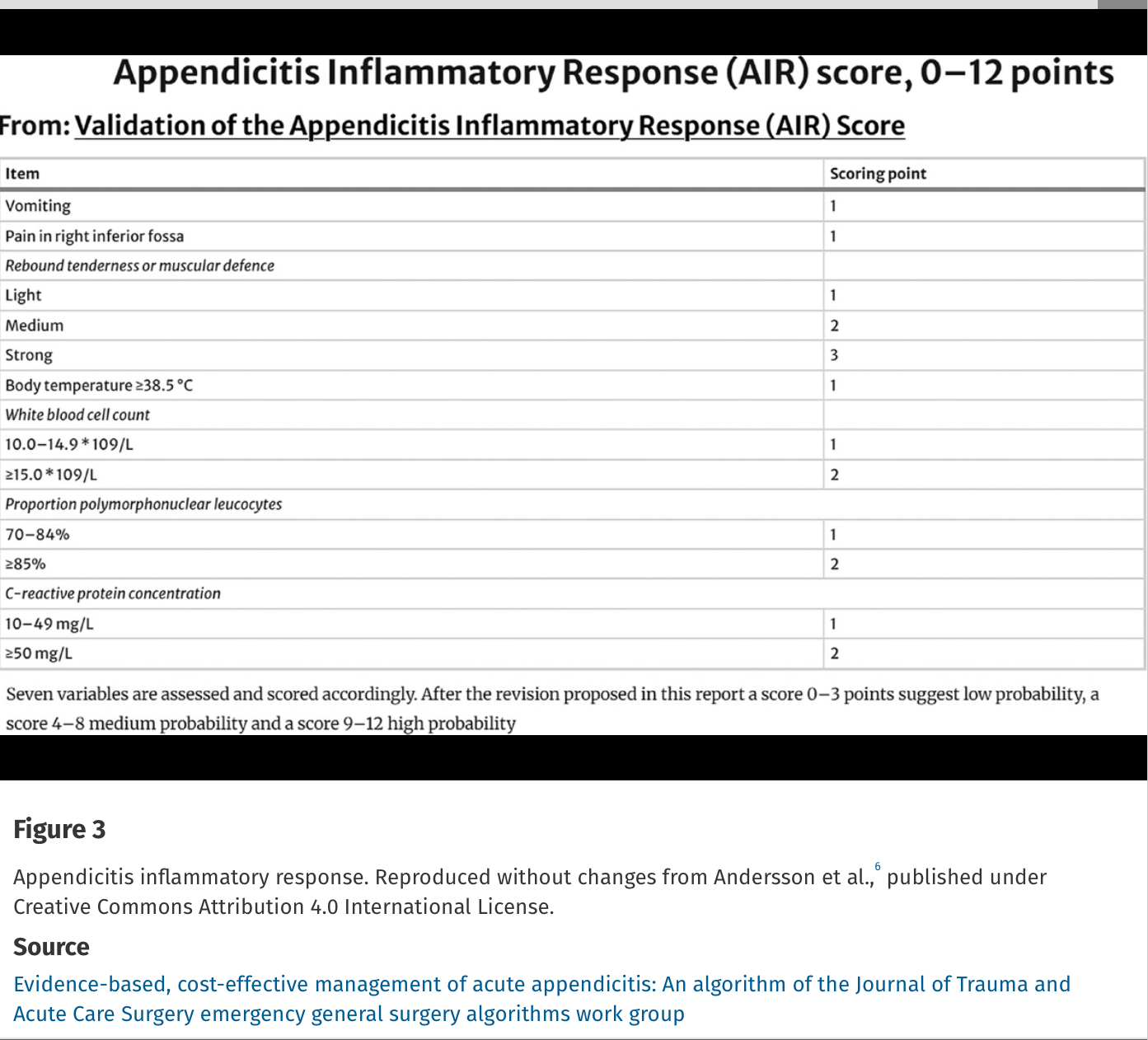
Alvarado Score: If a patient scores 1 to 4, the risk of appendicitis drops to 33%. If a patient scores >5, the risk of acute appendicitis is 66% or greater.