This study from Australia reminds us that what patients think they ingested isn’t always what they did ingest. A high percentage of “cocaine” and other stimulants was actually fentanyl or other opiates. The authors do a nice job referencing similar studies in the United States. Any overdose could be a mixed picture due to impure street drugs.
Perinatal HIV transmission in the U.S. can approach rates of <1% if appropriate interventions are offered to both pregnant individuals and their neonates.
However, a recently published case series evaluating hospitals in Maryland noted that there were 6 new cases of perinatal HIV transmission in 2022, compared with nationwide decreases and zero cases in the state of MD in 2021. Transmission was believed to be related to several issues: delayed entry to prenatal care, HIV diagnosis occurring in pregnancy (as opposed to pre-conception), adherence in the setting of hardships such as substance use, and delays in anti-retroviral therapy (ART) initiation during pregnancy.
How can we work to lower perinatal HIV transmission? Opportunities include the use of pre-exposure prophylaxis (PrEP), routine HIV testing in individuals of child-bearing age (especially if at high-risk of HIV acquisition), and rapid initiation of ART in pregnant individuals. As emergency physicians and providers, we are at the front line of assessing for these barriers and getting patients the resources they need to minimize perinatal transmission.
A 2023 retrospective cohort study comparing amiodarone to lidocaine for in-hospital cardiac arrests (IHCA) with refractory VT/VF found that use of lidocaine was associated with increased chance of ROSC, 24 hour survival, survival to discharge, and favorable neurologic outcome at hospital discharge.[1]
Now, a recent study comparing amiodarone to lidocaine in the pre-hospital setting for OHCA has found similar results. [2] Another retrospective cohort study using propensity score matching, they evaluated 23,263 adult patients with OHCA and defibrillation refractory VT/VF managed by 1700 EMS agencies.
Use of lidocaine was associated with greater odds of prehospital ROSC, fewer post-drug administration defibrillations, and greater odds of survival to discharge.
In comparison to earlier trials, these studies are some of the first demonstrating benefits to lidocaine use over amiodarone that reach statistical significance, but of course have all the limitations that come with retrospective studies and are not further analyzed in the context of etiologies for cardiac arrest or application of post-ROSC care.
Bottom Line: If you happen to be someone who reaches for amiodarone as your go-to, it may be time to start considering lidocaine.
The Jarisch-Herxheimer reaction (JHR) is a non-specific set of symptoms (fever, malaise, worsened rash, hemodynamic instability, leukocytosis) seen after treating syphillis and other spirochete induced infections. In this study 1 in 4 patients treated with 2.4 million units of benzathine penicillin G developed a short lived JHR. Those who developed the reaction were more likely HIV negative, had secondary syphillis and had successful treatment at 6 months.
A recent cohort study performed by the NCAA and US Department of Defense looked at NCAA athletes and military cadets who had suffered a concussion.
The study included 1661 NCAA athletes and military cadets, mean age was about 18 years, and 45% were women.
In these groupings, 813 people took over-the-counter pain relievers after their concussion and 848 people did not take any pain relievers.
Analgesics used included medications such as acetaminophen or NSAIDs such as ibuprofen.
Acetaminophen (n = 600), NSAIDs (n = 75), and those taking both (n = 78).
1) 50% recovery
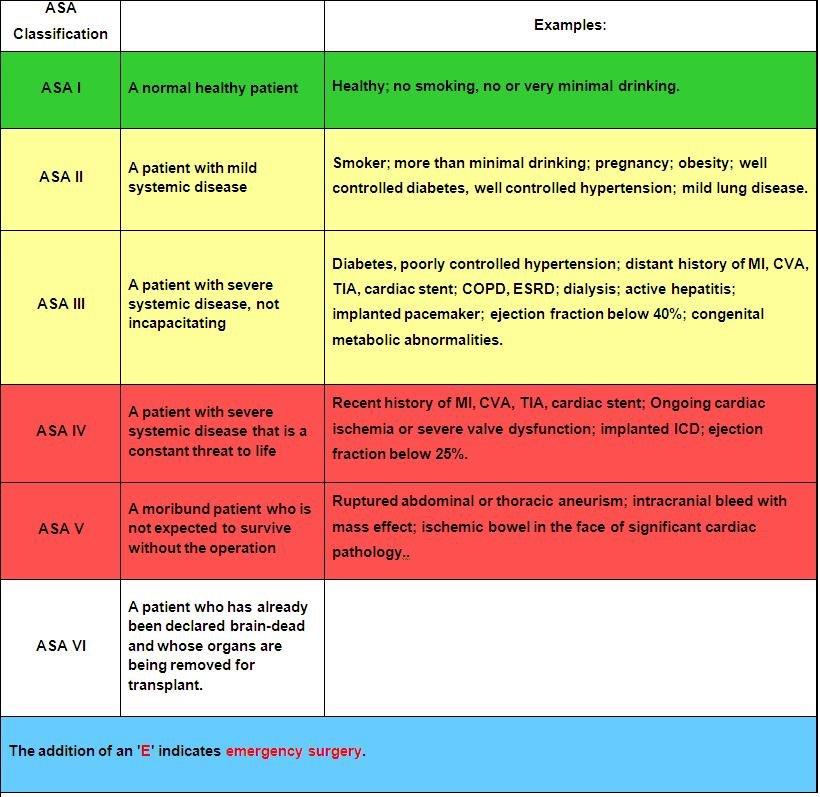
The American Society of Anesthesia score was an independent predictor of 90-day mortality as
well as low functional status at one year in 720 patients presenting to a single center with
moderate to severe brain injury. When used in conjunction with other prognosticating tools such
as the Trauma and Injury Severity Score, it increased the prognostic value of these scales.
Anticoagulation is the mainstay of treatment of cerebral venous sinus thrombosis, irrespective of whether associated venous hemorrhage is present. Anticoagulant selection is variable, with physicians opting for unfractionated heparin (UFH) about 72% of the time in one international study. However, recent evidence favors the use of low-molecular-weight heparin (LMWH), with meta-analytic data showing trends towards lower mortality rates and improved functional outcomes in LMWH cohorts. UFH is often viewed more favorably due to the ability to rapidly discontinue the infusion in the event of major bleeding; however, risk of major bleeding complications were actually found to be lower in patients treated with LMWH compared to UFH. Further, LMWH has many pharmacological and practical benefits compared to UFH, including more predictable pharmacokinetics, reduced risk of heparin-induced thrombocytopenia (HIT), lack of need for frequent aPTT monitoring, ease of administration (daily subcutaneous injection), and ease of transition to outpatient therapy.
Takeaway: Consider LMWH (1.5mg/kg subcutaneously once daily) as first-line treatment for CVST in patients with acceptable renal function.
Better teamwork creates better outcomes in emergency medicine. This study investigated how communication practices between physicians and nurses in the ED influence team dynamics and the sense of belonging to the healthcare team.
Methods: 38 emergency physicians and emergency nurses from EDs within a single metropolitan area participated in focus groups.
Positive Influences on Team Belonging:
Negative Influences on Team Belonging:
The findings emphasize the importance of fostering positive communication practices to enhance team dynamics, cohesiveness, and overall well-being within ED healthcare teams.
If you watch those medical drama (House MD, ER, Grey’s Anatomy, Resident…), the doctors and residents are always faced with a dilemma – is it a rare autoimmune disorder or is it an infection? They are worried that if they give steroid to a patient with infections, that would kill the patients.
Well, it might not be the case for Community acquired pneumonia.
A meta-analysis of randomized control trials involving 3224 patients to look into the efficacy of adjuvant corticosteroids for CAP. The authors assessed the heterogeneity of treatment effect (different groups should have different response to treatment).
For patients who were anticipated to benefit (those who had CRP > 240 mg/L), corticosteroids were associated with lower odds of 30-day mortality (OR 0·43 [0·25–0·76], p=0·026).
When stratifying by risk, there was no significant effect between those with Pneumonia Severity Index (PSI) I-III versus those with PSI IV-V.
However, corticosteroids increased odds of hyperglycemia (OR 2·50 [95% CI 1·63–3·83], p<0·0001), odds of hospital readmissions (1·95 [1·24–3·07], p=0·0038)
Discussion:
There were different regiments for corticosteroids in the included studies. However, hydrocortisone appeared to be more effective than other corticosteroids.
Furthermore, the time intervals for treatment is still debatable. The data suggested that the ideal treatment is within 24 hours of hospital admission, but patients can still benefit from treatment in up to 48 hours.
A response-dependent treatment is also recommended: 8 days or 14 days, depending on how patients respond to treatment by day 4.
Conclusion:
Adjuvant treatment with corticosteroids among hospitalized patients with CAP was significantly associated with reduction of 30-day mortality. The treatment effect, however, varied according to patients CRP concentrations at baseline.
Controlling pain from rib fractures impacts morbidity and mortality. Over the past decade there has been a focus on decreasing opiate use and approaching this painful condition in a multimodal way. “The multimodal approach utilizes a combination of delivery methods including oral, parenteral, and regional single-shot or catheter-based techniques. Oral medications include opioids, non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, skeletal muscle relaxants, alpha-2 agonists, mood stabilizers, and neuropathic pain medications. Parenteral medications encompass most of the oral options in addition to ketamine and lidocaine. Regional anesthesia includes epidural analgesia (EA), paravertebral blocks, intercostal blocks, and myofascial plane blocks.”
This study is a single center in Canada looking at medication used for patients admitted over 10 years with rib fractures along with demographics, injury severity and outcomes. The authors concluded:
“Although multimodal pain management strategies have improved over time, a large proportion of patients, even among those with flail chest, still do not receive multimodal pain management. Elderly patients, at highest risk of adverse outcomes, were less likely to receive multimodal pain management strategies and should be the target of performance improvement initiatives.”
Achieving faster homeostasis in trauma patients leads to lower mortality, less coagulopathy, and lower total blood volume transfusion requirements. This study looked at time to achieving homeostasis as defined by transfusion requirements as well as laboratory measurements in critically ill trauma patients who either received whole blood or component therapy transfusion as part of their resuscitation. Those receiving whole blood achieved statistically significant faster homeostasis.
This was a retrospective analysis of pediatric cardiac arrests that occurred out of hospital in Japan, where no pediatric termination of resuscitation is allowed. 1007 arrests were included. Patients that were placed on ECMO were excluded. This study included both medical and traumatic arrests looking at a primary outcome of 1 month moderate or better neurological disability. CPR time for both EMS and the hospital prior to ROSC were included. Bystander CPR was not included in these calculations. Possible downtime prior to CPR was not taken into consideration.
Overall, less than 1% of pediatric patients exhibited one-month moderate disability or better neurological outcome when total CPR duration is more than 64 minutes.
A few states have pediatric out of hospital termination of resuscitation protocols. This study used CARES data to create a termination protocol that was not only linked to ROSC, but also to neurological outcomes. This study only included medical arrests.
21240 children were included in the study where 2326 patients survived to hospital discharge. A total of 1894 survived with a favorable neurological outcome. The criteria developed for pediatric TOR in this study had a specificity of 99.1% and a PPV of 99.8% for patient death. Another set of criteria had a 99.7% specificity and PPV of 99.9% for predicting death or survival with poor neurological outcome.
TOR criteria of death consisted of:
unwitnessed arrest
asystole
arrest not due to drowning or electrocution
no sustained ROSC
TOR criteria of death or survival with poor neurological outcome:
unwitnessed arrest
asystole
arrest not due to drowning or electrocution
no sustained ROSC
no bystander CPR
Bottom line: Pediatric termination of resuscitation in the out of hospital setting can be appropriate under the right set of conditions.
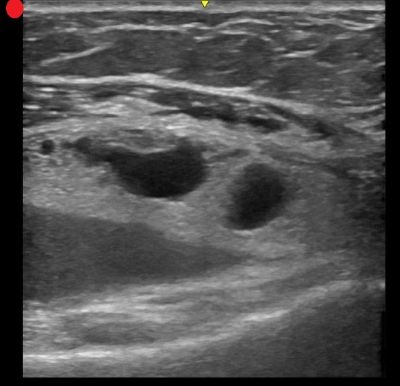
On ultrasound, lipohemarthrosis—the presence of blood and fat in the joint cavity—is a key clinical indicator of an intra-articular fracture.
Lipohemarthrosis appears as three distinct layers near the joint line.
Unless a patient is unstable, renal injuries are managed non-operatively or endovascularly. Here is the
2025 Kidney Injury Grading Scale from AAST.
AAST AIS
Grade Severity Imaging Criteria
I 2 –Subcapsular hematoma <3.5 cm without active bleeding
– Parenchymal contusion without laceration
II 2 – Parenchymal laceration length <2.5 cm
– HRD <3.5 cm without active bleeding
III 3 – Parenchymal laceration length ?2.5 cm
– HRD ?3.5 cm without active bleeding
– Partial kidney infarction
– Vascular injuries without active bleeding
– Laceration extending into urinary collecting system and/or urinary extravasation
IV 4 – Active bleeding from kidney
– Pararenal extension of hematoma
– Complete/near-complete kidney infarction without active bleeding
– MFK without active bleeding
– Complete/near-complete ureteropelvic junction disruption
V 5 – Main renal artery or vein laceration or transection with active bleeding
– Complete/near-complete kidney infarction with active bleeding
– MFK with active bleeding
Ramadan is the holy month in the Islam faith, where observers will fast from sunrise to sunset. This includes food, water, some medications, smoking and sex. This can obviously have some impact on patients' health, especially when presenting to the ED. Here are some considerations to keep in mind:
As with everything, maintaining cultural awareness and compassion will help to
Simple Febrile Seizures are a very common cause for presentation to the Emergency Department.
Up to 5% of children will have one in their lifetime, and a single febrile seizure increases risk of recurrence.
Definition:
While not part of the formal definition, the following details are critical to obtain on history, and high risk features that should not be missed on initial evaluation:
Evaluation and Management:
Consider a finger stick
Most patients can be discharged to home after a period of observation - most use a 2-4 hour minimum. More recent literature suggests considering a longer observation period in patients who have seizures at lower core body temperatures (<39°C) or those with a history of recurrent simple febrile seizures (2 simple febrile seizures within 24 hours with return to baseline in between)
Obtain a lumbar puncture in all patients with symptoms of meningitis
Consider a lumbar puncture, lab evaluation, and prolonged observation in patients who are under-vaccinated/unvaccinated/unknown vaccination status between 6 months and 12 months of age, or received antibiotics within the last 48 hours
On March 3, 2025, the FDA approved tenecteplase to treat acute ischemic stroke. Historically, only alteplase was FDA-approved, but the stroke guidelines suggest tenecteplase as a reasonable alternative and many centers have made the change to use tenecteplase.
The EXTEND-IA TNK trial showed benefit of tenecteplase over alteplase in patients who were candidates for mechanical thrombectomy. The newer AcT trial found that tenecteplase was non-inferior to alteplase for patients eligible for thrombolysis, regardless of thrombectomy candidacy. There was no difference in safety outcomes, specifically ICH or angioedema in either trial.
Tenecteplase will soon be available in a new 25 mg vial with stroke-specific packaging (potentially as early as June 2025). Currently, there is only a 50 mg vial that is used for STEMI and PE which has higher maximum dosing compared to stroke.
The dosing is now recommended in weight-based groupings based on the supplemental appendix from the AcT trial. This is likely a change in practice for most centers that previously implemented tenecteplase for stroke before the FDA approval. Consult with your stroke and pharmacy team to discuss potential protocol changes at your institution.

Many of us probably use droperidol for pain relief in the ED. If you don't, two recent studies highlight it's use in multimodal pain control:
-In the DRUGS study (2023), droperidol reduced opiod use (46% vs 60%), lowered pain scores (median of 9 vs 5), and decreased the need for antiemetics (60% vs 73%). Before you ask - mean pain score wasn't reported!
-This study evaluated gastroparesis patients, with most common dose of droperidol being 1.25 mg IV
-the DREAMER study (2024) showed that pateitns receiving droperidol required fewer opiods (median 10 Morphine Milligram Equivalents vs 19.4 MME). No significant different in need for antiemetics
-This study evaluated abdominal pain patients, with 2.5 mg IV being the most common dose
Neither study found statistically significant differences in length of stay. Additionally, neither study reported major adverse effects or healthcare costs. Note that these were both single center trials as well.
With droperidol shortages ongoing, suggestions were made to directly compare droperidol to haloperidol, with hopefully more research coming soon!
So you have a patient who is pregnant and has abdominal pain. You, as the astute provider you are, decide to do an ultrasound to rule out an ectopic, and low and behold! You see a gestational sac and a yolk sac within the uterus! You show your patient, you both breathe a sigh of relief, and you discharge them…
But they return two weeks later, now hypotensive, excruciating pain, and extremely pale. On an emergent bedside ultrasound, you see copious amounts of free fluid, and OBGYN tells you, after they rush your patient to the OR, that it was an ectopic - but how? The pregnancy was in the uterus!
Welcome everyone to the world of interstitial and angular pregnancies, pregnancies that are much closer to the endometrium than normal ectopic pregnancies and therefore have a much higher chance of progressing further before they rupture, meaning that when they do, they are devastating!
To evaluate for these ectopics, make sure that you get a mantle distance on every pregnancy ultrasound you do looking for an ectopic. Mantle distance is measured from the end of the gestational sac to the outer edge of the thinnest side of endometrium. If your value is >0.8cm, you should be okay. If it's less than <0.5cm, you most likely have an ectopic. Between 0.5cm and 0.8cm, consult OB urgently or have extremely close follow up for your patient.
