Patients may present atypically with ischemic strokes, reporting symptoms such as face or hemibody pain, lightheadedness, mental status change, headache and non-neurological symptoms.
Up to 25% of patients will have these symptoms.
Women are more likely than men to present with these atypical (or “nontraditional”) symptoms, especially altered mental status.
Background:
Animal studies in post-ROSC management after cardiac arrest have repeatedly demonstrated poorer neurological outcomes with higher amounts of oxygen administration.1 Studies in humans have also demonstrated dose-dependent associations between hyperoxia and poorer neurologic outcomes, as well as in-hospital mortality.2,3
Recent Data
A retrospective analysis of prospectively-collected data in 187 OHCA patients undergoing postarrest care with targeted temperature management found worse neurologic outcomes in patients experiencing hyperoxia in the first 6 hours following ROSC.4
This association was dose-dependent, with worsening outcomes as with higher PaO2 levels >200.
Bottom Line:
Boutonniere Deformity
aka buttonhole deformity
Misdiagnosed as a “jammed” or “sprained” finger
Recently, an ex-Russian spy and his daughter were poisoned in Salisbury, England using a Soviet nerve agent called Novichok. He joins a list of defectors and ex-spies who's poisoning have been connected to Russia.
Nerve agents are organophosphate compounds, similar to the commercially available pesticides, but significantly more potent. Nerve agents such as VX take seconds to minutes to irreversibly inhibit acetylcholinesterase by “aging” and result in clinical toxicity.
Signs and symptoms
Treatment
Worsening hypoxemia is not uncommon upon initiation of VV ECMO for severe ARDS as tidal volumes drop to double digits (often <20cc) after transition to “lung rest” ventilator settings. The following are strategies to improve peripheral oxygenation:
1. Increase the blood’s oxygen content
- Ensure FIO2 of ECMO sweep gas is 1
- Increase ECMO blood flow
o Limited by cannula size and configuration – may require placement of additional venous drainage cannula
o Also limited by greater risk of recirculation and hemolysis
- Increase blood oxygen-carrying capacity
o Transfuse PRBCs – some advocate for goal hemoglobin 12-14, though institutional practices vary significantly
2. Minimize recirculation
- Maximize distance between drainage and return cannulae
3. Reduce oxygen consumption
- Optimize sedation and neuromuscular blockade. (This is not the appropriate scenario for awake ECMO.)
- Consider therapeutic hypothermia
4. Decrease cardiac output and intrapulmonary shunt
- Consider beta blocker (esmolol) infusion
- Prone positioning (only if staff are experienced with proning on ECMO as this poses significant risk of cannula displacement)
5. Consider switching to hybrid configuration (VVA – continued venous drainage cannula and venous return cannula with addition of arterial return cannula)
Peri-Intubation Cardiac Arrest
Fluid overload (defined in this study as (fluid input-output)/weight)) is associated with longer hospital stays, longer treatment duration and oxygen use.
Bottom line: Treat dehydration appropriately but try not to over resuscitate the asthmatic. Further studies are needed before definitive recommendations are made.
Pectoralis Major Rupture
Most commonly seen in male weightlifters
Usually occurs as a tendon avulsion
Incidence is increasing
Hx: Sudden, sharp, tearing sensation with pain and weakness with arm movement
PE: Palpable defect and deformity of anterior axillary fold. Bruising and swelling.
Deformity may not be obvious with arm by side and relaxed
Testing: Weakness with ADDuction and internal rotation
Treatment: Operative treatment has better outcomes but depends on patient subgroups
Nonoperative treatment generally indicated for partial ruptures and tears in the body of the pec and muscle tendon junction
Sling, ice and pain control.
Operative treatment generally for high demand patients (athletes) and bony avulsion injuries
Signs and symptoms of acute cyanide poisoning are not well characterized due to its rare occurrence. Commonly mentioned characteristics of bitter almond odor and cherry red skin have poor clinical utility.
Recently published review of 65 articles (102 patients) showed that most patients experienced following signs and symptoms:
There is no clear toxidrome for cyanide poisoning.
In a poisoned patient, health care providers should consider cyanide in their differential diagnosis in the presence of severe metabolic and lactic acidosis (lactic acid > 8 in isolated cyanide poisoning or > 10 in smoke/fire victim).
Fosfomycin is an antibiotic infrequently used for the treatment of urinary tract infections (UTIs). It has a broad spectrum of activity that covers both gram-positive (MRSA, VRE) and gram-negative bacteria (Pseudomonas, ESBL, and carbapenem-resistant Enterobacteriaceae), which is useful in the treatment of multidrug-resistant bacteria.
Fosfomycin is FDA approved for the treatment of uncomplicated UTIs in women due to susceptible strains of Escherichia coli and Enterococcus faecalis (3g oral as a single dose). Data has also demonstrated that it can be used for complicated UTIs; however, dosing is different in this population (3 g oral every 2-3 days for 3 doses). Fosfomycin is not recommended for pyelonephritis.
The broad spectrum of activity, in addition to only needing a single dose in most cases, makes fosfomycin an attractive option; however, it should be reserved for use in certain circumstances. Fosfomycin should not be considered as a first-line option. It is also more expensive than other medications (~$100/dose) and in countries with high rates of utilization bacteria are developing resistance to fosfomycin. In addition, most outpatient pharmacies do not keep this medication in stock.
Take-Home Point:
Fosfomycin should be reserved for multidrug-resistant UTIs in which other first-line options have been exhausted.
A leading cause of cardiac arrest in patients 40 years and younger is due to drug poisoning. Adverse cardiovascular events (ACVE) such as myocardial injury (by biomarker or ECG), shock (hypotension or hypoperfusion requiring vasopressors), ventricular dysrhythmias (ventricular tachycardia/fibrillation, torsade de pointes), and cardiac arrest (loss of pulse requiring CPR) are responsible for the largest proportion of morbidity and mortality overdose emergencies. Clinical predictors of adverse cardiovascular events in drug overdose in recent studies include:
Bottom line:
Obtain ECG and perform continuous telemetry monitoring in overdose patients with above risk factors. Patients with two or more risk factors have extremely high risk of in-hospital adverse cardiovascular events and intensive care setting should be considered.
Benign headaches are common in bodybuilders. However, several less benign headaches are worth noting:
All except the first two are exclusively reported in patients on anabolic steroids, growth hormone, and/or “energy” supplements. Make sure to ask your patient about these risk factors.
Which septic patients should receive empiric antifungal therapy?
Patients with fungemia only make up about 5% of patients presenting with septic shock, but invasive fungal infections are associated with increased hospital mortality (40-50%), prolonged ICU and hospital length of stay, and increased costs of care.1
The EMPIRICUS trial showed no mortality benefit to empiric antifungals for all, even patients with candidal colonization and recent exposure to antibiotics.2
Bottom Line
Therapy should always be tailored to the specific patient, but providers should strongly consider admininistering empiric echinocandin (micafungin, caspofungin) over fluconazole in patients with severe sepsis/septic shock and:
*Especially consider addition of antifungal in patients who do not show improvements after initial management with IVF and broad spectrum antibiotics in the ED.*
The search for an objective reliable test for mild traumatic brain injury found an early promising result last week.
May be arriving in your hospital in the near future.
A handheld sideline version is sure to follow
The FDA approved the first blood test for concussion/mild TBI
Called the Banyan BTI (Brain Trauma Indicator)
This test measures 2 neural protein biomarkers released into the blood following mild TBI
The FDA approved this test within 6 months after reviewing data on just under 2,000 blood samples.
They concluded the Banyan BTI can predict the absence of cranial CT lesions with an accuracy greater than 99% and may reduce imaging in up to a 1/3rd
Be optimistic but consider the small sample size and remember that this test looks for biomarkers and may miss subtle cases where proteins didn’t leak. This test is NOT ready to be used for return to play decisions. It takes 3 to 4 hours to result and costs about $150. Other biomarkers are being investigated and may prove to be better
https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm596531.htm
Abnormal ocular movement (e.g. nystagmus) can often be observed in select CNS pathology.
Certain drugs/toxin overdose can also induce nystagmus.
In an "unknown" intoxication, physical exam findings such as nystagmus may help narrow the identity of the suspected ingestion/overdose.
-Nonischemic cardiomyopathy, classically seen in post-menopausal women preceded by an emotional or physical stressor
-Named for characteristic appearance on echocardiography and ventriculography with apical ballooning and contraction of the basilar segments of the LV – looks like a Japanese octopus trap or “takotsubo" (pot with narrow neck and round bottom)
-Clinical presentation usually similar to ACS with chest pain, dyspnea, syncope, and EKG changes not easily distinguished from ischemia (ST elevations – 43.7%, ST depressions, TW inversions, repol abnormalities) and elevation in cardiac biomarkers (though peak is typically much lower than in true ACS)
** Diagnosis of exclusion – only after normal (or near-normal) coronary angiography **
-Care is supportive and prognosis is excellent with full and early recovery in almost all patients (majority have normalization of LVEF within 1 week)
-Supportive care may include inotropes, vasopressors, IABP, and/or VA ECMO in profound cardiogenic shock
** LVOT Obstruction **
-occurs in 10-25% of patients with Takotsubo’s cardiomyopathy
-LV mid and apical hypokinesis with associated hypercontractility of basal segments of the LV predisposes to LV outflow tract obstruction
-Important to recognize as it is managed differently:
-may be worsened by hypovolemia, inotropes, and/or systemic vasodilatation
-mainstay of treatment is avoidance of the above triggers/exacerbating factors while increasing afterload
*phenylephrine is agent of choice +/- beta blockade
Take Home Points:
***Diagnosis of exclusion!!! Presentation very similar to ACS and ACS MUST be ruled out
* Treatment is supportive and similar to usual care for cardiogenic shock. Can be severe and require mechanical circulatory support!
*10-25% have LVOT obstruction. Manage with phenylephrine +/- beta blockade
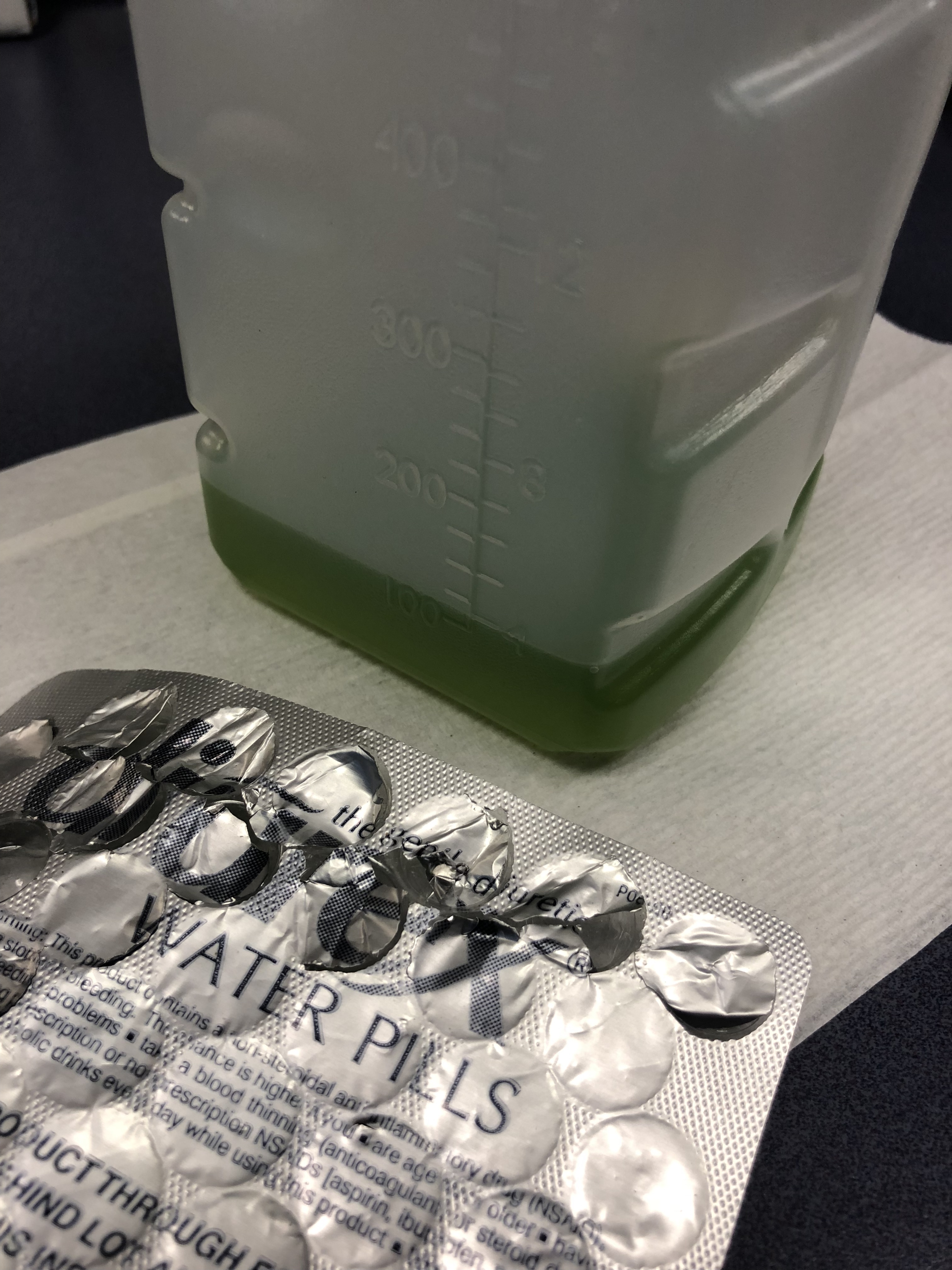
75 y/o M is brought in by EMS after he fell off the light rail and hit his head. In the ED he is A&Ox3, and is asking for a urinal. Two minutes later the tech comes running to show you the following:
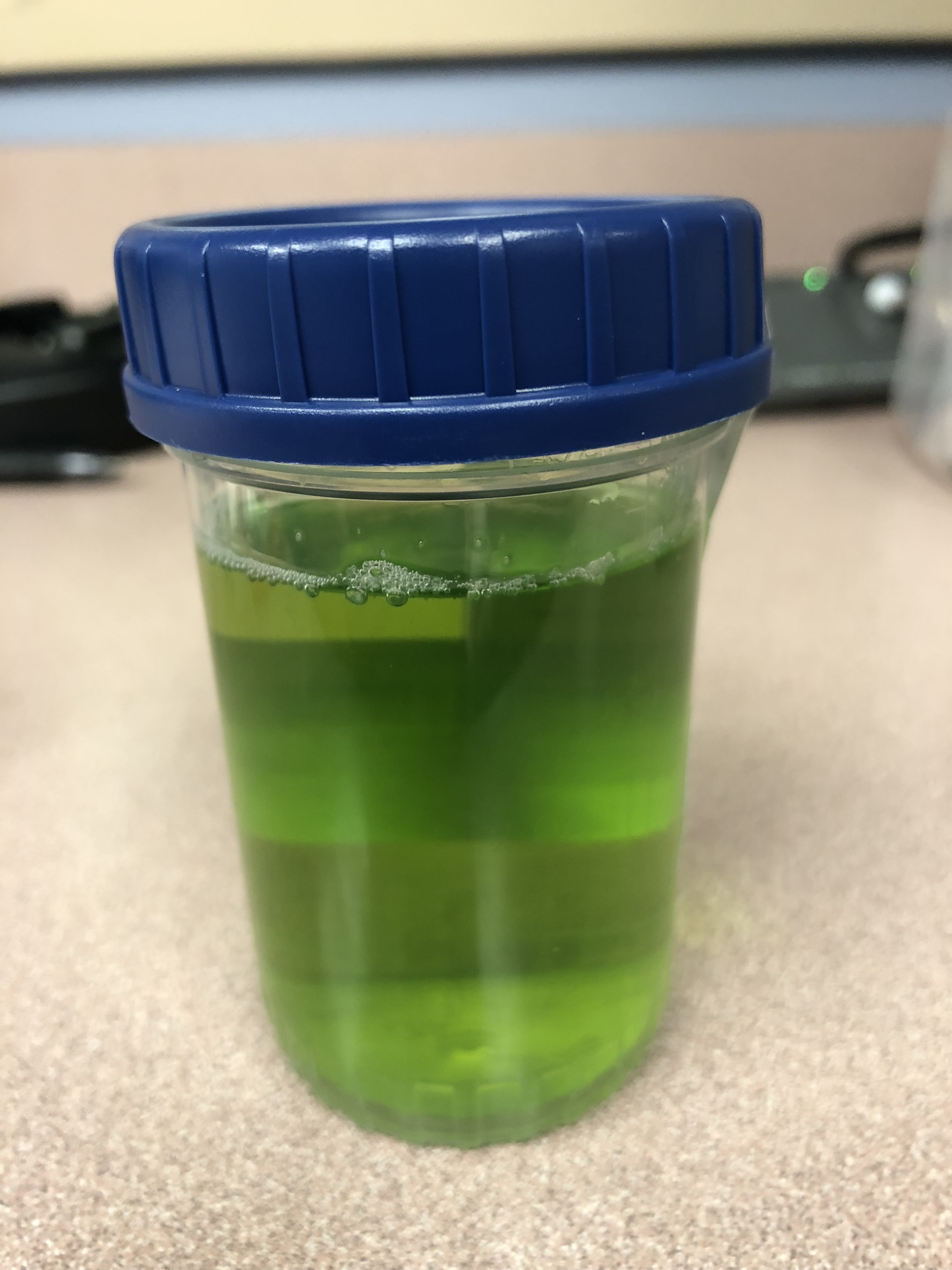
What is the cause of this patients Jolly Rancher Green Apple looking urine sample?
Patient: 11 month old with trouble breathing and color change after a family member sprayed air freshener. Symptoms have since resolved.
What are you concerned about in the attached xrays?