Cannabinoid hyperemesis is a syndrome (CHS) characterized by severe intractable nausea, cyclical vomiting, and abdominal pain associated with chronic marijuana abuse. It is often a underrecognized cause of cyclic vomiting syndrome. Despite well established anti-emetic properties of marijuana, paradoxical effects on the GI tract exist through cannabinoid receptors which exert their neuromodulatory properties in the central nervous system and the enteric plexus. Multiple theories of mechanism of CHS are in the literature. Diagnosis is based on the following clinical criteria:
Acute care goals are to treat dehydration and terminate nausea and vomiting. Administration of intravenous fluids, dopamine antagonists, topical capsaicin cream, and avoidance of narcotic medications are recommened treatment measures. Benzodiazepines followed by haloperidol and topical capsaicin are reported to be most effective. Capsaicin activates the transient receptor potential vanilloid 1 receptors (TRPV1) which impairs substance P signalling in the area postrema and nucleus tract solitarius similar to noxious stimuli, such as heat.
Traumatic brain injury (TBI) is associated with close to half of major trauma admissions in adults over age 65 in the U.K.
Falls accounted for 85% of all TBIs, while 45% of patients had subdural hematomas (SDH).
More than 3/4 of patients were treated conservatively, though outcomes were not significantly better than those who underwent neurosurgical intervention.
Higher age is associated with higher mortality and greater disability.
Bottom Line: Trauma in older adults is increasing and fall prevention is important in reducing significant injuries.
Molecular Adsorbent Recirculating System (MARS) is an artificial liver support system colloquially known in the medical field as "dialysis for the liver."
Take-Home:
1. Consider MARS in your patient with severe acute liver failure due to potentially reversible/recoverable etiology
2. Know if and where MARS is offered near you

(http://findbesttreatment.com/images/healthnet_dialyse_schema.gif)
Fever occurs in 40% of patients with sepsis. Historically, there has been conflicting evidence of whether patient outcomes improve with antipyretic therapy.
A recent large meta-analysis assessed the effect of antipyretic therapy on mortality of critically ill septic patients. The analysis included 8 randomized studies (1,531 patients) and 8 observational studies (17,432 patients) that assessed mortality of septic patients with and without antipyretic therapy.
The authors found no difference in mortality at 28 days or during hospital admission. There was also no difference in shock reversal, heart rate, or minute ventilation.
As expected, they found a statistically significant reduction in posttreatment body temperature (-0.38°C, 95% IC -0.63 to -0.13) in patients who received antipyretic therapy. NSAIDs and cooling therapies were more effective than acetaminophen, however no agent or dosing information was provided and only one study included physical cooling therapies.
Bottom Line: Antipyretic therapies do not reduce mortality in patients with sepsis, but they may improve patient comfort by reducing body temperature.
Bronchiolitis season will soon be upon us. Here are some risk factors for children under 2 y/o with bronchiolitis, who may be more likely to suffer respiratory decompensation:
1. Age under 9 months
2. Black race
3. Hypoxia documented in the ED
4. Persisent accessory muscle use.
Bottom Line: Consider providing respiratory support sooner than later in bronchiolitic infants with risk factors for decompensation. For HFNC, start at 1.5 - 2.0 L/kg/min, and titrate to work of breathing and 02 saturations.
_______________________________________________________________________________
Pathophysiology: Bronchiolitis is a disease process that leads to inflammation of lower airways, causing bronchiolar edema, epithelial hyperplasia, mucus plugging, and air trapping or atelectasis. Common viral causes include RSV, Human Metapneumovirus, Rhinovirus, Influenza, and Parainfluenza.
Clinical Course: For most strains, the disease course is often 5-7 days with the worst days being 3-5. The disease process can last longer, especially in neonates. The predominant presenting symptoms are often rhinorrhea, low grade fevers, and cough, but apnea can be the primary symptom in younger infants. As a result of increased work of breathing, PO feeding tolerance decreases and leads to dehydration.
Treatment: Primarily supportive care with suctioning, hydration, supplemental oxygen via standard NC, HFNC, and in severe cases BiPAP, CPAP or intubation. Trial of bronchodilator is often used, but there is no role for repeated bronchodilator use if no benefit is seen in pre and posttreatment respiratory effort. Hypertonic saline is not recommended for routine use in the ED. Corticosteroids have no role for routine use in viral bronchiolitis, either.
Hunan hand syndrome is a painful contact dermatitis that frequently presents in cooks and chili pepper workers after preparing or handling chili peppers. Contact with other body parts gives rise to the terms: "Hunan nose" ''Hunan eye",and "Chili Willie". Capsaicin, found in the fruit of plants from the genus Capsicum such as red chili peppers, jalapeños, and habaneros, is a hydrophobic, colorless, odorless compound that binds with pain receptors causing the sensation of intense heat or burning. The "heat" or pungency of a peppers is measured in Scoville heat units (SHU), the number of times a chili extract must be diluted with water to lose heat. Habanero peppers generate 30,000 SHU. Even at low concentrations capsaicin is a skin irritant. It is the primary ingredient in pepper spray used in law enforcement and in personal defense sprays.
Treatment consists of decontamination with water irrigation for opthalmic exposure and milk or antacids for dermal or gastrointestinal exposure. Burning can be recurrent and of of long duration depending on tissue penetration. Topical anesthetic especially for the eye and cool compresses for the skin can relieve pain. Parodoxically capsaicin is used as a topical analgesic medication for local pain relief from muscle pain, itching, and painful neuropathies (diabetic, postherpetic). Capsaicin initially causes neuronal excitation followed by a long-lasting refractory period due to depletion of substance P, during which neurons are no longer responsive to a large range of stimuli and thus are desensitized.
Risk of Pneumocystis pneumonia (PCP) increases with degree of immunosuppression. If clinical suspicion exists (CD4 <200 with cough, pulmonary infiltrates, hypoxic respiratory failure), it is reasonable to initiate empiric therapy.
First line treatment is trimethoprim-sulfamethoxazole (TMP-SMX) orally or IV for 21 days. IV pentamidine has equivalent efficacy to IV TMP-SMX but greater toxicity and is generally reserved for patients with severe PCP who cannot tolerate or are unresponsive to TMP-SMX.
Importantly, adjunctive corticosteroids have been shown to significantly improve outcomes (mortality, need for ICU admission, need for mechanical ventilation) in HIV-infected patients with moderate to severe PCP (defined by pO2 <70 mmHg on Room Air).
· Ideally steroids should be started BEFORE (or at the same time as) Pneumocystis-specific treatment to prevent/mitigate the sharp deterioration in lung function that occurs in most patients after initiation of PCP treatment. This is thought to be secondary to the intense inflammatory response to lysis of Pneumocystis organisms, which can cause an ARDS-like picture.
· Recommended dosing schedule: 40mg prednisone twice daily for 5 days, then 40mg once daily for 5 days, followed by 20mg once daily for the remaining 11 days of treatment.
Bottom Line: In patients with moderate to severe PCP (pO2 <70 mmHg on RA), don’t forget to initiate adjunctive corticosteroids early (at the same time you initiate empiric therapy for PCP).
The current number of influenza cases in the Southern Hemisphere is substantially higher than normal. For example, in Australia the number of influenza cases this year are twice the next highest year. 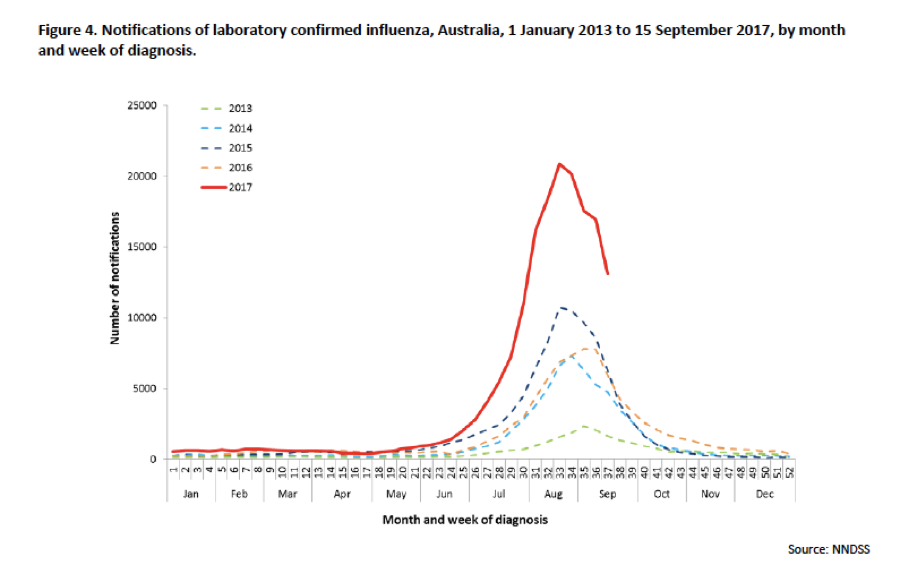
Have you gotten your flu shot yet?
Providing consistent, quality emergency care to the elderly is critically important. The Geriatric Emergency Department (GED) guidelines, developed collaboratively, provide a standardized set of guidelines to help improve care of the geriatric population in the emergency department.
Lever Sign/Lelli’s test
A new test for diagnosing ACL tears
Higher sensitivity (94 - 100%) than the Lachman test (highest sensitivity test to date)
With time and more study, this may become our new gold standard physical examination test
Very easy to learn and apply to bedside care
Can help with diagnosing partial tears
Area of manipulation is the femur and not the tibia (as in other tests)
Consider incorporating into your standard knee examination
https://www.youtube.com/watch?v=T9ujIYIctdw
Original study
https://www.ncbi.nlm.nih.gov/m/pubmed/25536951/
Validation
https://www.ncbi.nlm.nih.gov/pubmed/26753117
Thank you to Ari Kestler for sending
Since the first description of acute respiratory distress syndrome (ARDS), various consensus conferences (including American-European Consensus Conference (AECC) and the Berlin Conference) have produced definitions focused on adult lung injury but have limitations when applied to children.
This prompted the organization of the Pediatric Acute Lung Injury Consensus Conference (PALICC), comprised of 27 experts, representing 21 academic institutions and eight countries. The goals of the conference were 1) to define pediatric ARDS (PARDS); 2) to offer recommendations regarding therapeutic support; and 3) to identify priorities for future research in PARDS.
Although there were several recommendations from the group, some notable ones, in contrast to the Berlin definition focused on adults, include: 1) use the Oxygenation Index (or, if an arterial blood gas is not available, the Oxygenation Severity Index) rather than the P/F ratio; 2) elimination of the requirement for “bilateral” pulmonary infiltrates (may be unilateral or bilateral) 3) elimination of specific age criteria for PARDS.
Tune in next month for pearls on management for children with PARDS...
Hyperkalemia is a potentially life threatening problem which can lead to cardiac dysrhythmias and death. Drug interactions inducing hyperkalemia are extremely common such as the combination of ACE inhibitors and spironolactone or ACE inhibitors and trimehoprim sulfamethoxazole. Hyperkalemia can also occur with a single agent and is a relatively common complication of therapy with trimethoprim sulfamethoxazole. The following drugs can cause hyperkalemia:
The blue-ringed octopus (genus Hapalochlaena) is normally found in the Great Barrier Reef and other coastal waters and tide pools around Australia and other Western Pacific islands. Though not an aggressive animal, when it does bite, such as stepped upon, it can inject tetrodotoxin along with a number of other toxic compounds.
Tetrodotoxin can cause paralysis, leading to respiratory failure and death, though the blockage of voltage-gated fast sodium channel conduction, blocking peripheral nerve conduction. Treatment is supportive, as the venom usually wears off within 4 to 10 hours.
Post-Arrest Tidal Volume Setting
Elective surgeries with general anesthesia are often cancelled when the child has an upper respiratory tract infection. What are the adverse events when procedural sedation is used when the child has an upper respiratory tract infection?
Recent and current URIs were associated with an increased frequency of airway adverse events (AAE). The frequency of AAEs increased from recent URIs, to current URIs with thin secretions to current URIs with thick secretions. Adverse events not related to the airway were less likely to have a statistically significant difference between the URI and non-URI groups
AAEs for children with no URI was 6.3%. Children with URI with thick/green secretions had AAEs in 22.2% of cases. Children with URIs did NOT have a significant increase in the risk of apnea or need for emergent airway intervention. The rates of AAEs, however, still remains low regardless of URI status.
During the past several years, several new classes of diabetic medications were introduced for clinical use, including SGLT2 inhibitors (canagliflozin, dapagliflozin and empagliflozin).
SGLT2 inhibitors prevent reabsorption of glucose in the proximal convoluted tubules in the kidney and does not alter insulin release.
A recent retrospective study (n=88) of 13 poison center data from January 2013 to December 2016 showed
49 patients were evaluated in a health care facility (HCF) with 18 admissions. Referral to HCF was more common in pediatric patients. This was likely due to unfamiliarity with a new mediation and lack of toxicity data.
Other case reports have shown higher incidence of DKA with the therapeutic use of SGLT2 vs. other classes of DM medications.
Bottom line:
Limit data is available regarding the toxicologic profile of SGLT2 inhibitors.
Based upon this small retrospective study, hypoglycemia may not occur and majority of the patient experience minimal symptoms.
IV vs. Non-IV Benzodiazepines for Cessation of Seizures
Negative-pressure pulmonary edema (NPPE) is a well-documented entity that occurs after a patient makes strong inspiratory effort against a blocked airway. The negative pressure causes hydrostatic edema that can be life-threatening if not recognized, but if treated quickly and appropriately, usually resolves after 24-48 hours. These patients may have any type of airway obstruction, whether due to edema secondary to infection or allergy, laryngospasm, or traumatic disruption of the airway, such as in attempted hangings.
Management:
1. Alleviate or bypass the airway obstruction.
· Usually via intubation; may require a surgical airway
· If obstruction in an intubated patient is due to biting on tube or dyssynchrony, add bite-block (if not already in place), sedation, and even paralysis if needed.
2. Provide positive pressure ventilation and oxygen supplementation.
3. Use low tidal volume ventilation.
4. In severe hypoxemia without shock, add a diuretic agent and consider additional measures such as proning and even ECMO if the hypoxemia is refractory to standard therapy.
Viscosupplementation
Hyaluronic acid (HA) is a high-molecular weight polysaccharide
A major component of synovial fluid and of cartilage
Major role of HA is as a lubricant, shock absorption, antinociceptive effect
Used in veterinary medicine for decades
Multiple brands exist with differences based on the molecular weight and how they are produced
Use supported by the Cochrane database (2007, 2014) for knee OA
Post injection strength gains are due to pain relief
May have a role for those who cannot receive steroid injections
Inject in similar manner to intra articular steroids
Caution in those with known allergy to poultry /eggs
Risks: Local reaction (likely from preservative), injection site pain, infection, bleeding.