Transfusion in Major Trauma: The PROPPR Trial
What should we be transfusing in major trauma?
The Trial
Results
Conclusions
How does this affect my practice?
A 1:1:1 transfusion practice is safe and can decrease mortality from hemorrhage in major trauma
Other points: control bleeding, permissive hypotension, avoid crystalloids, use TEG to guide therapy (TXA etc)
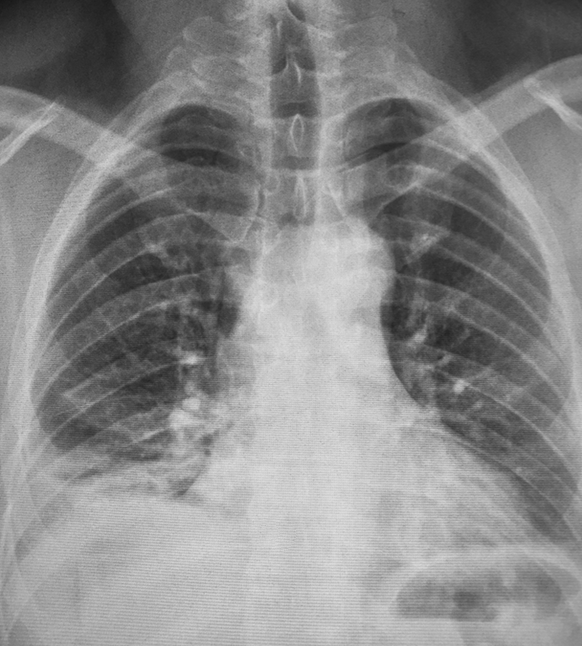
35 year-old female presents with acute leg pain and swelling. What's the diagnosis?

Afib Clinical Decision Aid: AFFORD
- Atrial fibrillation (AF) affects ~34 million people worldwide; the hospital admission rates vary with frequencies of 81%, 62%, and 24% in the US, Australia, and Canada respectively.
- Lack of a reproducible and accurate risk stratification/decision aid likely contributes to variability in ED disposition.
- AFFORD (Atrial fibrillation and flutter outcome risk determination) was the 1st clinical decision aid (contains 17 variables) to predict 30-day adverse events in a prospective ED patient cohort with acute symptomatic AF.
- Vanderbilt University Medical Center's ED (2010-2013) derived and internal validated an ED based clinical decision aid for prediction of MACE within 30 days utilizing the AFFORD decision aid in hemodynamically stable patients whose AF reverted to sinus rhythm, either spontaneously or after cardioversion (pharmacologic or electrical), and those who are adequately rate controlled and candidates for outpatient management.
- Incorporating AFFORD with a shared decision model into ED practice may help identify patients at low risk and potentially reduce rate of hospitalizations.
Emergency Departments are increasingly searching for alternatives to opioids for acute pain management.
An urban trauma center in California retrospectively evaluated their use of low-dose ketamine for acute pain over a two-year period. [1]
Application to Clinical Practice
There was no comparison group and there was no mention of what other pain medicines were given. Adverse events are often under-reported in retrospective studies. This study seems to demonstrate that low-dose ketamine administration for acute pain management in the ED is feasible with a low rate of adverse effects.
It's worth noting that a new review of 4 randomized controlled trials evaluating subdissociative-dose ketamine found no convincing evidence to support or refute its use in the ED. The 4 included trials had methodologic limitations. [2]
Background: While much of international health focuses on communicable diseases, it is clear that noncommunicable diseases (NCDs), such as cardiovascular diseases, cancer and diabetes, causes substantial morbidity and mortality.
Epidemiology:
Bottom line: As in developed countries, risk factors for NCDs deaths include physical in activity, tobacco use, unhealthy diabetes, harmful use of alcohol.
High-Flow Nasal Cannula for Apneic Oxygenation
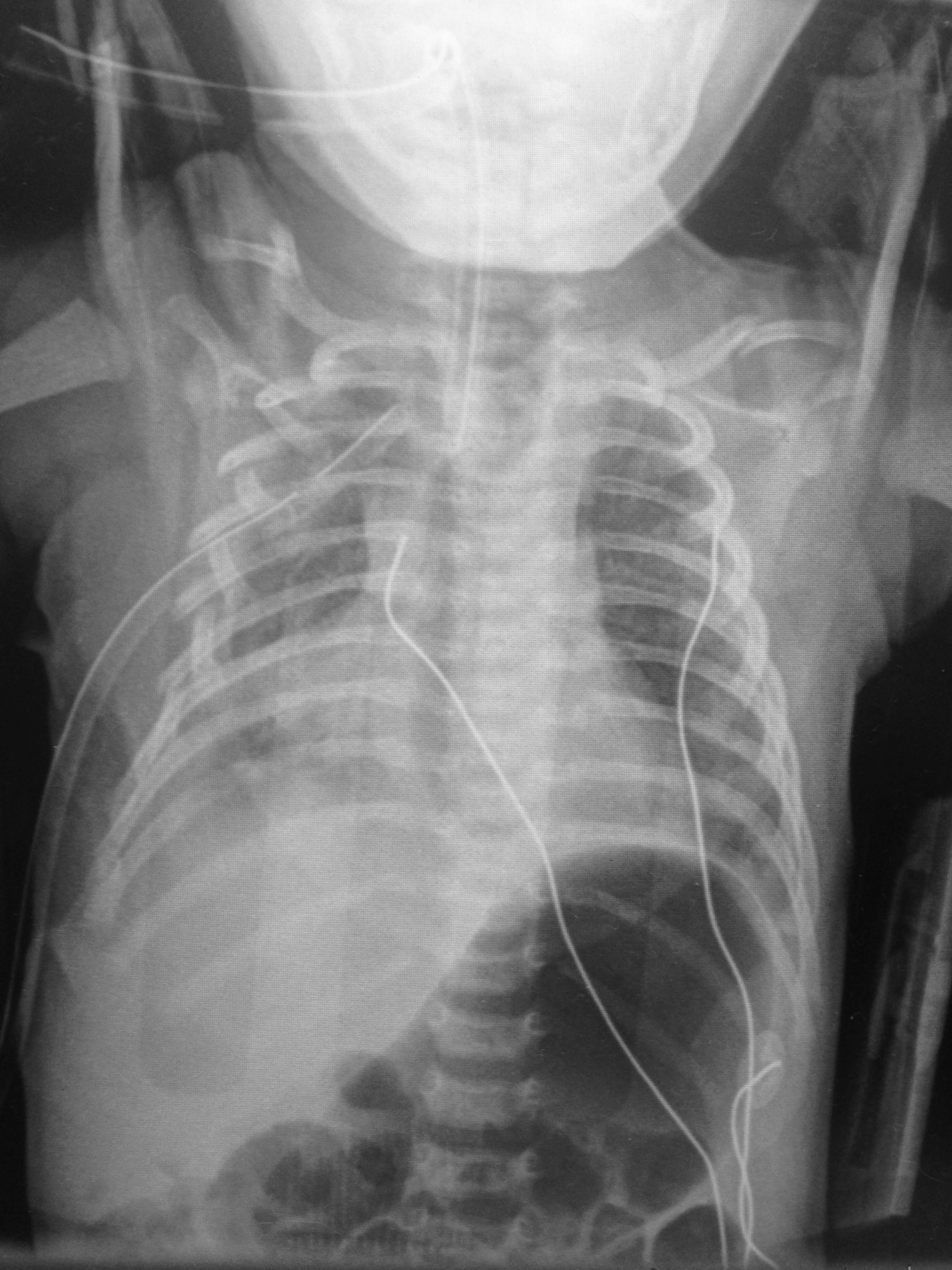
6 day-old child is brought in by parents with 1 day of reduced oral intake and 4 hours of rapid breathing. The child has no fever and no significant birth history. The child is tachycardic, hypotensive, and hypoxic. What’s the diagnosis?
Safety Risk? Digoxin in Atrial Fibrillation
- Digoxin is commonly utilize for atrial fibrillation/flutter with rapid ventricular response, though beta blockers and/or calcium channel blockers are a better 1st line therapy given digoxin’s narrow therapeutic index and lack of mortality benefit.
- Digoxin in the acute setting is often favored given its ability to reduce the heart rate while maintaining or slightly augmenting blood pressure.
- 2014 AHA/ACC guidelines recommend digoxin, specifically for rate control in patients with heart failure and/or reduced ejection fraction.
- There have been 2 post hoc studies from the AFFIRM trial which showed conflicting results w/regards to digoxin and risk of mortality.
1. Increased risk of mortality associated w/digoxin (on-treatment analytic strategy)
2. No association w/mortality (intent-to-treat analytic strategy)
- A recent retrospective cohort examination of newly diagnosed afib patients without heart failure & no prior use of digoxin; digoxin was independently associated with a 71% higher risk of death & a 63% higher risk of hospitalization.
- Consistent and substantial increase in mortality and hospitalization risk was seen using both on-treatment and intent-to-treat analytic methods.
- Given other available rate control options, digoxin should be used with caution.
Sesamoid Injuries
The first MTP joint contains the 2 sesamoid bones. They play a significant part in the proper functioning of the great toe. 30% of individuals have a bipartite medial or lateral sesamoid.
http://www.coreconcepts.com.sg/mcr/wp-content/uploads/2008/05/sesamoid_foot.jpg
Injury can occur from trauma, stress fracture or sprain of the sesamoid articulation or of the sesamoid metatarsal articulation. Overuse injuries tend to occur in sports with a great deal of forefoot loading (basketball/tennis).
SXs: Pain with weight bearing, pain with movement of first MTP, ambulation on lateral part of foot.
PE: Tenderness and swelling over medial or lateral sesamoid. Resisted plantar flexion (flexor hallucis) reveals pain and weakness.
Imaging: plain film with sesamoid view to assess for a sesamoid fracture. Stress fractures may take 3-4 weeks to show on plain film.
http://www.agoodgroup.com/running/Fracture002.jpg
Treatment for fractures and suspected stress fractures involve 4 to 6 weeks of non weight bearing.
Orthopedic Causes of Chest Pain
The first thing that pops into everybody’s mind when they hear a patient state they have chest pain radiating to the left arm is Acute Coronary Syndrome and specifically a Myocardial Infarction. However, there are a lot of orthopedic causes of chest pain that can also radiate to the left arm. It is estimate that up to 20% of patients with pectoral symptoms have an underlying orthopedic problem.
Some of them are:
Some other less common causes are
So instead of just ordering some troponin and admitting to medicine, consider that the cause can be orthopedic in origin.
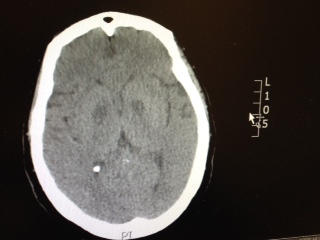
Patient has the following Head CT, what is your differential diagnosis? There are only a few characteristic toxins that can cause this type of finding on CT.
Neurologic causes of cardiac arrest have not been well described. Two recent retrospective studies looked at the epidemiology and clinical features of these patients.
Hubner P. et al.
Arnaout M. et al.
Neurologic causes of cardiac arrest are uncommon presentations that may be difficult to distinguish from cardiac etiology of cardiac arrest. If history and clinical presentation suggests a neurologic cause, obtain a non-contrast head CT for evaluation.
The Role of the CVP in a Post- “7 Mares” Era
The role for using central venous pressure (CVP) as a measure of volume responsiveness has largely fallen out of favor over the years.1 There are certainly better indices for fluid responsiveness, but don’t be fooled – the CVP isn’t a one trick pony. In fact, a high or rapidly rising CVP should raise a significant concern for impending cardiovascular collapse.
Consider the following differential diagnosis in the patient with an abnormally high or rising CVP ( >10 cm H2O).
Bottom Line: In a time where the utility of the CVP has been largely dismissed, remember that an abnormal CVP offers great deal of information beyond a simple measure of volume status.
References
Follow me on Twitter: @JohnGreenwoodMD
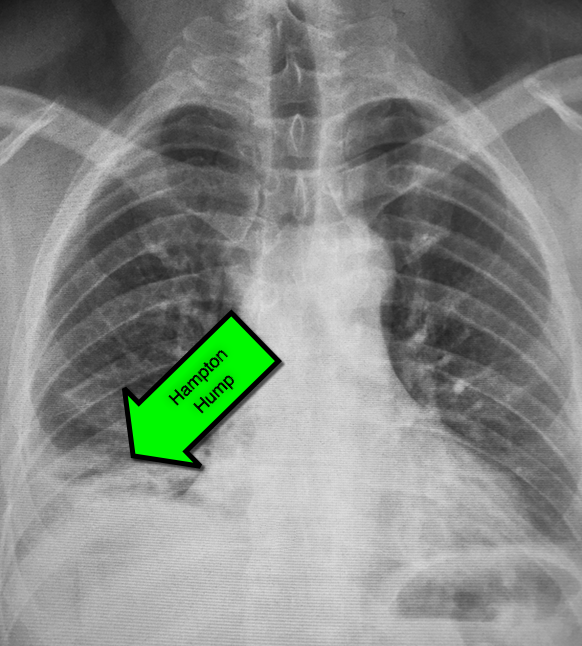
45 year-old male complains of pleuritic chest pain following a "long" flight. What's the diagnosis and what's this sign called?
This study is a case control study of the association of congenital heart disease (CHD) and stroke using a base population of 2.5 million Kaiser patients in California. 412 cases of stroke were identified and compared to 1236 controls. Of these stroke patients, 11/216 ischemic strokes and 4/196 hemorrhagic strokes were attributed to CHD (both cyanotic and acyanotic lesions). CHD was found in 7/1236 controls.
Children with CHD and history of cardiac surgery had the strongest risk of stroke (31 fold over the control group). Many of these children had strokes years after their surgery. Children with CHD who did not have cardiac surgery had a trend towards elevated stroke risk, but the confidence intervals included the null. More children without CHD history presented with headache.
Bottom line: Stroke risk (both hemorrhagic and ischemic) extend past the immediate postoperative period in patients with CHD.
The Centers for Disease Control continues to report increased numbers of measles patients in the US. From January 1 to February 13, 2015 there have been 141 cases. It has spread to 17 states and the District of Columbia, with 80% linked to the multistate outbreak from Disneyland.
Measles is not a benign disease!
Per the World Health Organization, there were 146,700 measles deaths globally in 2013. Most of these deaths occur in lower- and middle-income countries,
Even in the US, measles can cause serious complications and death. Complications from measles can be seen in any age group, but particularly in children <5 years of age and in adults >20 years of age.
Measles Complications:
Common:
Severe:
Long-term:
Bottom Line:
Per Dr. Anne Schuchat of the CDC: “This is not a problem with the measles vaccine not working. This is a problem of the measles vaccine not being used.”
As the cold and snow rips through the United States, hypothermia is a major concern because each year approximately 1,300 Americans die of hypothermia.
Classification of hypothermia:
The risk of cardiac arrest increases when the core temperature is less than 32 Celsius and significantly rises when the temperature is less than 28 Celsius. Rapid rewarming is required as part of resuscitation should cardiac arrest occur.
A rescue therapy to consider (when available) is extra corporeal membrane oxygenation (ECMO). ECMO not only provides circulatory support for patients in cardiac arrest, but allows re-warming of patients by 8-12 Celsius per hour.
Some studies quote survival rates of 50% with hypothermic cardiac arrest patients receiving ECMO versus 10% in similar patients who do not receive ECMO.
As winter lingers in the United States, consider speaking to your cardiac surgeons now to plan an Emergency Department protocol for hypothermic patients that may require ECMO.

The Unforgotten: ECG Utilization to Differentiate Athletic Heart vs. Brugada
- Highly trained athletes develop ECG changes as a physiologic consequence of increased vagal tone; The ECG manifestations of early repolarization (ER) can range from simple J–point elevation to anterior (V1 to V3) "domed" ST-segment elevation and negative T wave.
- The former raises problems of differential some forms of ER with the “ coved-type” pattern seen in Brugada Syndrome (BS).
- A recent study compared the ECG tracings of 61 athletes w/a “domed” ST-segment elevation & negative T wave and 92 age/sex-matched BS patients w/a “ coved-type” pattern to identify an ECG criteria for distinguishing benign athletic changes seen in ER from BS.
- ECG analysis focused on ST-segment elevation at J-point (STJ ) and at 80 milliseconds after J-point (ST80 ).
- Athletes had a lower maximum amplitude of STJ (p < 0.001) & lower STJ /ST80 (p < 0.001)
- All patients (100%) with BS showed a downsloping ST-segment configuration (STJ/ST80 > 1) versus only 2 (3%) athletes (p < 0.001)
- An upsloping ST-segment configuration (STJ /ST80 < 1) showed a sensitivity of 97%, a specificity of 100%, and a diagnostic accuracy of 98.7% for the diagnosis of ER.
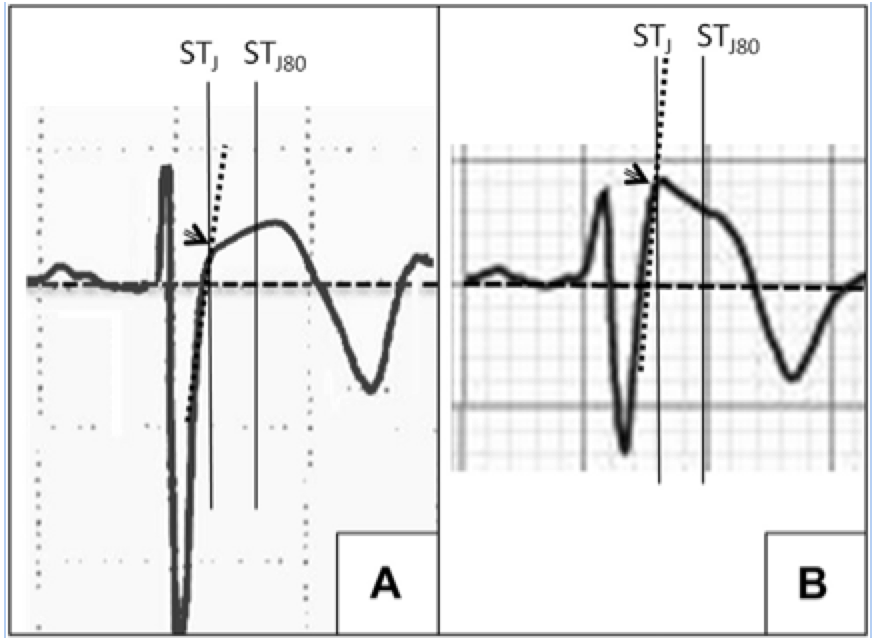
A: ER
B: Brugada
LATERAL ANKLE TENDINOPATHY
Hx: subacute onset (weeks) of the pain seen in athletes esp. runners (banked or uneven surfaces).
PE: Tenderness to palpation posterior to the lateral malleolus or over the course of the tendon. Pain worse with resisted ankle eversion from a dorsiflexed postion. Examine for subluxation of tendon.
The diagnosis is made from the above and does not require imaging.
Tx: Rest, conservative care, physical therapy (eccentric exercise focus), ankle taping or lace up brace. Severe cases may even require a walking boot.
http://www.epainassist.com/images/Article-Images/Peroneal_Tendonitis.jpg