In this study the researchers looked at patients presenting to the emergency department with high suspicion for ACS and explored if Regional Wall Motion Abnormality (RWMA) evaluation by EPs was associated with occlusion myocardial ischemia (OMI).
FOCUS identified RWMA in 87% of patients with coronary angiography proven OMI. With a sensitivity of 94%, specificity 35%, and overall accuracy of 78%.
The authors concluded that using FOCUS can have good utility when a patient is high risk for OMI and has an equivocal ekg. However, if RWMA is not present, physicians should still continue with work up such as cardiac catheterization.
To evaluate RWMA it is easiest to:
For more information check out this ACEPnow article: https://www.acepnow.com/article/detect-cardiac-regional-wall-motion-abnormalities-point-care-echocardiography/?singlepage=1
Hypoxemic respiratory failure is a common presentation of critically ill patients. If the degree of hypoxemia is severe and disproportionate to the patient's radiographic findings and not responding to increasing FiO2, a right-to-left shunt should be considered. To evaluate for an anatomic shunt, an intravenous agitated saline contrast (ASC) echocardiographic evaluation can be conducted by an ED provider at the bedside.
Technique:
Interpretation:
This is a review of the literature surrounding using mechanical compression devices for in-hospital cardiac arrest. The bottom line is there isn’t much evidence to support the use of these devices and there is scant literature in general on this topic. This is an area in need of further research
CCM recently published Stanford's experience with their Emergency Critical Care Program (ECCP), an ED based intensivist consultation/management model staffed by EM/CC during peak hours with the "goals of improving care of the critically ill in the ED, offloading the ED team, and optimizing ICU bed utilization without the need for a dedicated physical space."
Conclusions:
This is the third group to document decrease in overall mortality utilizing an early or dedicated critical care consult model. EC3 and the CCRU here at UMMC have also both shown improvements in patient transfer and resource utilization metrics. As with all studies in this space, there are many limitations to these studies in both design and generalizability, even amongst each other. However, the literature is replete with data that increased boarding time in the ED for critically ill patients is associated with worse outcomes and these studies are now a body of complementary and growing evidence that teams such as this can perhaps bridge that gap. Hopefully come to an ED near you soon...
Study Details:
Objectives: To determine whether implementation of an Emergency Critical Care Program (ECCP) is associated with improved survival and early downgrade of critically ill medical patients in the emergency department (ED).
Design: Single-center, retrospective cohort study from a tertiary academic medical center using ED-visit data between 2015 and 2019 for adult medical patients presenting to the ED with a critical care admission order within 12 hours of arrival.
Pre and post intervention (2017) cohort analysis of patients when facility implemented dedicated bedside critical care by an ED-based intensivist "following initial resuscitation by the ED team". A difference-in-differences (DiD) analysis compared the change in outcomes for patients arriving during ECCP hours (2 pm to midnight, weekdays) between the preintervention period (2015–2017) and the intervention period (2017–2019) to the change in outcomes for patients arriving during non-ECCP hours (all other hours).
Primary outcomes: In-hospital mortality and proportion of patients downgraded to non-ICU status while in the ED within 6 hours
Results:
In a systematic review looking at patients over age 65 who sustained a cervical spine injury from a low-level fall, there was a 3.8% prevalence of injury identified. The paper could not correlate injury with GCS level or altered level of consciousness due to the quality of the data available.
Bottom line again is patients over age 65 with low-level falls should be considered to have significant injury until proven otherwise.
Glucagon therapy in beta blocker and calcium channel blocker overdose is controversial and no high level evidence is available to support or refute its use in overdose treatment.
Glucagon has the ability to bypass adrenergic blockade from beta and calcium channel blocking agents and theoretically increase myocardial contraction, increase heart rate, and increase AV conduction through cyclic AMP production.
However, practically, the use of glucagon is limited due to high risk of vomiting and subsequent risk of aspiration with administration as well as the high cost and limited hospital stock available for continued use.
Given these limitations, glucagon therapy is no longer recommended for calcium channel blocker overdose in the 2017 Critical Care Medicine Expert Consensus*. The use in beta blocker therapy is still recommended. However, caution must be taken to ensure that more advanced (and possibly more efficacious) therapies such as vasopressors and high dose insulin are administered without delay.
The dose of glucagon therapy for this indication is 3-10 mg IV. You can repeat this dose a second time if no response is seen with the first dose. If clinical response is seen with bolus dosing, transition to continuous infusion at the dose of clinical response (eg. if two 5 mg boluses produced the desired response; start 10 mg/hr infusion). Antiemetic administration prior to initial bolus dose is highly recommended to avoid vomiting.
This paper looks at the possibility of intramuscular tranexamic acid (TXA) administration. Pharmacologic studies support this route as giving correct drug bioavailability to control hemorrhage. Several London, England pre-hospital services have begun using intramuscular TXA for trauma patients when intravenous access cannot be quickly obtained. This paper suggests 500 mg intramuscular injection dosing.
Acute lower back pain is a very common emergency department presenting complaint. Over the last several years there has been impetus to move away from opioids in the management of lower back pain.
A recent systematic review investigated the pharmacologic management of acute low back pain. This review looked at RCTs investigating the efficacy of muscle relaxants, NSAIDs, and acetaminophen for the treatment of acute nonspecific lower back pain of fewer than 12 weeks duration in patients > 18 years of age. Studies that investigated the use of opioids were not considered.
18 RCTs, totaling 3478 patients were included. 54% were women. The mean patient age was 42.5 ± 7.3 years. The mean length of follow-up was 8.0 ± 5.6 days. The mean duration of symptoms before treatment was 15.1 ± 10.3 days.
Results: Muscle relaxants and NSAIDs were effective in reducing pain and disability in acute LBP at approximately 1 week.
The combination of NSAIDs and acetaminophen was associated with a greater improvement than the sole administration of NSAIDs.
However, acetaminophen alone did not promote any significant improvement. Placebo administration was not effective.
Limitations: Most patients with acute LBP experience spontaneous recovery or at least reduction of symptoms, therefore, the real impact of most medications is uncertain. The present study wasn't able to distinguish among different classes of NSAIDs. A best practice treatment protocol cannot be extrapolated from this study.
Take home: In my practice, patients are treated with NSAIDs and Acetaminophen first line. I also include Licocaine patches for all patients. If there is a contraindication to NSAIDs, I treat with muscle relaxants alone.
This study highlights the lack of benefit of acetaminophen as mono therapy (which has been noted in other studies).
Background: Intranasal dexmedetomidine has seen usage in the anesthesia and sedation realms over the past few years, with an increasing interest in usage in the ED setting given its generally favorable safety profile and ease of administration. There has been specific interest and consideration in children with autism and neurodevelopmental disorders.
Study: Single center prospective provider study (compared to a retrospective group of patients under 18 who received oral midazolam for indications of agitation or anxiety via chart review) looking at patients 6 months to 18 years of age with an order for intranasal dexmedetomidine. Following use, a provider survey was completed to evaluate indication/rationale for use, satisfaction, comfort with use, and perceived time to onset as well as duration of effect.
Results: 29% of patients receiving IN dexmedetomidine experienced treatment failure compared with 20.7% of patients receiving oral midazolam (not statistically significant). In subgroup analysis, rates of treatment failure were lower for patients diagnosed with autism spectrum disorder receiving IN dexmedetomidine versus oral versed (21.2% versus 66.7%). Length of stay was longer in the IN dexmedetomidine group (6.0 hours versus 4.4 hours). Indication for use had variability between the two groups.
Bottom Line: IN dexmedetomidine may be a reasonable agent to utilize for anxiolysis in pediatric patients, especially those who have previously had paradoxical reactions or poor efficacy of benzodiazepines. It may be specifically useful when effects are desired for a slightly longer time and for non-painful/minimally painful interventions.
Background: The use of steroids in pneumonia has long been controversial with conflicting data, and the recent ESCAPe randomized controlled trial by Meduri et al. showing no mortality benefit with their use, but likely underpowered due to recruitment issues. The recently published CAPE COD study by Dequin et al. may change the game.
Design: Double-blind, placebo-controlled, multicenter, RCT
Intervention: Early hydrocortisone within 24 hrs, 200mg/day x 4-8 days depending on improvement, then preset taper
Primary outcome: Death at 28 days
Secondary outcomes:
Bottom Line: The addition of hydrocortisone to antibiotics in severe CAP may decrease need for intubation and development of shock, and in this well-done study, decreased 28 and 90-day mortality.
A retrospective review of patients over age 13 presenting to one urban level one trauma center and one urban community hospital looked at traumatic injuries in patients presenting for sexual assault. They looked at 157 patients and found 61% of assailants were acquaintances, 22% strangers, and 15% intimate partners. One third of all patients had some traumatic injury however only 12 patients has serious injuries such as non-fatal strangulation or a fracture. Assault by an intimate partner was more likely to lead to injury/trauma including non-fatal strangulation. Drug and alcohol use was not associated with presence of injury.
Myasthenia gravis is an autoimmune disease of the neuromuscular junction, most commonly due to antibodies attacking acetylcholine receptors in the postsynaptic membrane. Up to 30% of patients with myasthenia gravis will experience a myasthenic crisis during their disease course. If rapid sequence intubation is indicated, the unique characteristics of this patient population must be considered in the event use of a paralytic is necessary. All paralytic agents can be expected to last significantly longer, and an unpredictable response may be seen with depolarizing agents - therefore non-depolarizing agents are preferred in this population.
Non-Depolarizing Agents (Rocuronium, Vecuronium)
Depolarizing Agents (Succinylcholine)
The classic teaching is that patients with acute pancreatitis should be aggressively hydrated with IV fluids. But as we increasingly question heavy handed fluid strategies in other areas such as sepsis, should we look at pancreatitis management too?
Li et al did a systematic review of the literature on aggressive fluid resuscitation (the exact protocol/definition varied per study, but we're mostly talking 15-20 mL/kg boluses followed by 3-5 mL/kg/hr infusion) vs less aggressive fluid resuscitation (mostly 10 mL/kg boluses followed by 1.5 mL/kg/hr infusion). They found that aggressive resuscitation worsened mortality in severe pancreatitis (RR 2.45) and trended towards worse mortality in non-severe pancreatitis (RR 2.26, but CI crossed 1). Aggressive was associated with more complications in both severe and non-severe pancreatitis pancreatitis.
Multiple society guidelines still call for aggressive IVF resuscitation for acute pancreatitis, but probably need to be updated given mounting evidence that this is harmful. More recent guidelines suggest "goal-directed therapy", but no one is completely sure what that means.
Bottom Line: In acute pancreatitis, a more conservative empiric IVF resuscitation is probably better than the clasically taught aggressive approach. Whether even less fluids would be better or worse is not known, but for now it's probably best to stick to a 10 mL/kg bolus and 1-2 mL/kg/hr infusion when ordering fluids for these patients unless you have another indication.
This study is a secondary analysis of another studying looking at hypertonic saline in traumatic brain injury (TBI) making it not the most robust study however it found that TBI patients who’s PaO2 dropped below 100 had a worse outcome than those whose PaO2 did not fall below 100.
Bottom line: This is a reminder that traumatic brain injury patients do not do well with hypoxia or hypotension even if transient (during intubation, etc.). Pre-oxygenate and resuscitate prior to intubation and maintain oxygen saturations in the mid-90s for your traumatic brain injured patients. This applies to prehospital, emergency department, and ICU settings
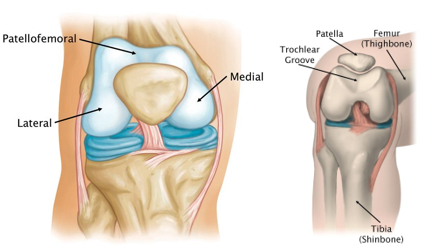
Patellofemoral anatomy and disease (part 1)
During normal knee flexion, the patella slides within the trochlear grove. Both (patella and the trochlear groove) are lined with articular cartilage at the patellofemoral articulation.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint2.jpg
Multiple forces act on the patella which can affect proper tracking: Proximately, by the quadriceps tendon, distally, by the patellar tendon, medially, by the medial retinaculum/vastus medialis and laterally by the lateral retinaculum and the vastus lateralis.
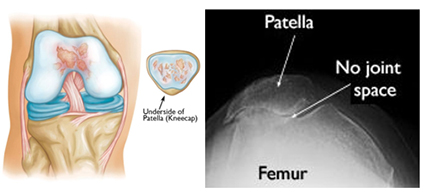
Patellofemoral OA can occur when this cartilage starts to wear and can be seen in skyline/sunrise/notch or equivalent views. OA here rarely occurs in isolation (<10%) and is usually part of medial or lateral knee OA.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint3.jpg
Patellofemoral pain is usually from overuse/training overload or malalignment.
Contributors to overuse involve total joint load which may have influence from training volume (total miles), intensity (competitive sports) in addition to BMI (>25) in addition to overall fitness level.
Malalignment aka abnormal patellar tracking involves both static (leg length discrepancy, hamstring tightness, etc.) and dynamic components (hip weakness, gluteus medius weakness, excessive foot pronation, etc.).
Patients with anterior knee pain should have activity modification, ice, NSAIDs (not steroids) and long-term engagement in physical therapy (>6 months) with a focus on flexibility and strengthening of lower extremity kinetic chain including the vastus medialis, gluteus medius, hip external rotators and core.
Also, consider looking for hyper supination or pronation. Foot orthotics can be of help with this.
Things to Consider for Persistent or Worsening Septic Shock
Predicting the need for a mass hemorrhage protocol (MHP) activation is important both for individual patient outcome as well as for proper utilization of critical resources such as blood products and healthcare workers time and effort. These two studies look at using the RABT score to predict the need for mass transfusion. The RABT score is:
A 4-point score
blunt (0)/penetrating trauma (1),
shock index (hr/SBP)≥ 1 (1),
pelvic fracture (1)
FAST positive (1)
With a score >2 predictive of needing MHP.
These studies (one in Canadian trauma centers, the other in US trauma centers) validate the use of this score to predict the need for activation of a mass hemorrhage protocol.
{kind=link}
{kind=link}