Despite ongoing research and efforts to improve our care of patients with ARDS, it remains an entity with high morbidity and mortality. Early recognition of the disease process and appropriate management by emergency physicians can have profound effects on the patient's course, especially in centers where ICU boarding continues to be an issue.
Recognition of ARDS (Berlin criteria)
*An ABG should be obtained in the ED if physicians are unable to wean down FiO2 from high settings, if oxygenation by pulse ox is marginal, or if the patient is in a shock state.
Tenets of ARDS Management:
*IBW Males = 50 + 2.3 x [Height (in) - 60] / IBW Females = 45.5 + 2.3 x [Height (in) - 60]
Strategies for Refractory Hypoxemia in the ED: You can't prone the patient, but what else can you do?
1. Escalate PEEP in stepwise fashion
2. Recruitment maneuvers
3. Appropriate sedation and neuromuscular blockade
4. Inhaled pulmonary vasodilators (inhaled prostaglandins, nitric oxide) if known or suspected right heart failure or pulmonary hypertension
Bottom Line: Emergency physicians are the first line of defense against ARDS. Early recognition of the disease process and appropriate management is important to improve outcomes AND to help ICU physicians triage which patients need to be emergently proned or even who should potentially be referred for ECMO.
In patients with lower back pain, there is good evidence that muscle relaxants reduce pain as compared to placebo and that different types are equally effective. However, the high incidence of significant side effects such as dizziness and sedation limits their use. Muscle relaxants may be beneficial in an every bedtime capacity thereby limiting side effects.
If cyclobenzaprine is used during daytime hours, a lower dose schedule may work as well as a higher dose with somewhat less somnolence (5 mg three times a day vs 10 mg three times a day. In general, muscle relaxants should only be used when patients cannot tolerate NSAIDs but can tolerate the side effect profile.
We commonly add muscle relaxants to NSAIDs hoping for a larger analgesic effect. However, combination therapy does not appear to be better than monotherapy.
Adding cyclobenzaprine to high-dose ibuprofen does not seem to provide additional pain relief in the first 48 hours in ED patients with acute myofascial strain. Among an ED population with acute non radicular low back pain, a randomized trial found that adding cyclobenzaprine/other muscle relaxants to Naproxen did not improve functional outcomes or pain at one week or 3 months compared to naproxen alone.
Take home: Consider the limited usefulness use of muscle relaxants in ED patients with back pain
The hyperoxia-hyperventilation test (aka 100% Oxygen Challenge test) is used to differentiate the cause of central cyanosis in the sick neonate. The majority of neonatal cyanosis is caused by either cardiac or respiratory pathology.
Classically the test is performed as follows:
1. An ABG is obtained with the neonate breathing room air
2. The patient is placed on 100% FiO2 for 10 minutes
3. A repeat ABG is performed looking for an increase in PaO2 to >150 mmHg
- If the hypoxia is secondary to a respiratory cause, the PaO2 should increase to >150 mmHg.
- If the hypoxia is secondary to a congenital cardiac lesion (i.e. secondary to a right-to-left cardiac shunt) the PaO2 is not expected to rise significantly.
In practice, many physicians instead use pulse oximetry and monitor the SpO2 pre and post administration of 10 minutes of 100% FiO2.
- If after 10min of 100% FiO2, if SpO2 is not ? 95% (some resources use 85%) then the central cyanosis is likely secondary to intracardiac shunt.
- When this occurs, presume the sick neonate is symptomatic from a congenital cardiac lesion and initiate prostaglandin E-1 (PGE1) at 0.05-0.01 mcg/kg/min. Use caution as PGE1 may cause apnea.
The primary tenet of poisoning treatment is to separate the patient from the poison. Gastric decontamination has been the cornerstone of poisoning treatment throughout history and methods include induced emesis, nasogastric suctioning, EGD or gastrostomy retrieval, activated charcoal, and whole bowel irrigation. Current guidelines for gastic decontamination are limited to few clinical situations. The detection of residual life threatening poisons in the stomach would be of value in predicting who might benefit from gastric decontamination in overdose.
Plain radiographs have variable sensitvity in detecting radioopaque pills. Computed tomography (CT) has been successful and gained wide acceptance in the detection of drug in body packers. In a recent study, authors studied the usefulness of non-contrast abdominal computed tomography for detection of residual drugs in the stomach in patients presenting over 60 minutes from acute drug overdose:
BOTTOM LINE:
Non-contrast CT may help to predict which patients would benefit from gastric decontamination in acute life-threatening drug poisonings.
Does This Patient Have Pericardial Tamponade?
Hyponatremia is the most common electrolyte abnormality in hospitalized patients, affecting approximately 15-30% of patients. Children have historically been given hypotonic maintenance IV fluids based off of theoretical calculations from the 1950s. Multiple studies have shown complications related to iatrogenic hyponatremia, including increased length of hospital stay, seizures and death.
The American Academy of pediatrics completed a systematic review and developed an updated clinical practice guideline:
Patient's age 28 days to 18 years requiring maintenance IV fluids should receive isotonic solutions with the appropriate amount KCl and dextrose.
Physostigmine is a cholinergic agent that can be administered to reverse delirium associated with anticholinergic toxicity. However, it is infrequenly used since the reports of cardiac arrest in patients with TCA overdose.
A recently published study reviewed 161 articles – involving 2299 patients – to determine the adverse effects and their frequency after the administration of physostigmine.
Findings
Adverse effects were observed in 415 patients (18.1%)
Specific adverse effects
Of 394 TCA overdose, adverse effects occurred in 14 patients (3.6%)
Conclusion
Neutropenic enterocolitis can occur in immunosuppressed patients, classically those being treated for malignancy (hematologic much more commonly than solid tumor). When involving the cecum specifically, it is known as "typhlitis."
It should be considered in any febrile neutropenic patients with abdominal pain or other symptoms of GI discomfort (diarrhea, vomiting, lower GI bleeding), and can be confirmed with CT imaging.
A recent study found that invasive fungal disease, most often candidemia, occurred in 20% of febrile neutropenic patients with CT-confirmed enteritis, a rate that increased to 30% if the patient was in septic shock.
Take Home:
1. Have a lower threshold for abdominal CT imaging in your patients with febrile neutropenia and abdominal pain/GI symptoms, especially if they are critically ill.
2. Consider addition of IV antifungal therapy if they are hemodynamically unstable with enterocolitis on CT.
Spurling’s maneuver and modified Spurling’s maneuver aka neck compression test.
This maneuver is highly specific for the presence of cervical root compression
Can be used to reproduce radicular pain/symptoms.
Perform this maneuver with caution as it should not be performed in patients who have potential cervical spine instability.
Keeping the patient’s head in a neutral position pressing down on the top of the head. If this fails to reproduce the patient's pain, the test is repeated with the head extended, rotated and tilted to the affected side (the modified Spurling’s maneuver).
Reproduction of symptoms (limb pain or paresthesias) beyond the shoulder is considered positive. Neck pain alone is nonspecific and constitutes a negative test.
The test has a high specificity (0.89 to 1.00) but low sensitivity (0.38 to 0.97).
Meaning a positive test is helpful but a negative test does not rule out radicular pain.
This test should be used in conjunction with a thorough history and physical examination (strength, sensation and reflex testing)
https://www.youtube.com/watch?v=17QWqbXjSpc
Management of Acute Variceal Bleeding
Yes.
Serum creatinine decreases with age with the decrease in lean body mass. However, the number of functioning glemeruli and kidney function decrease with age as well, making the creatinine an unreliable indicator of renal function in older adults.
The solution? Calculate the creatinine clearance (CrCl) (or GFR) for a more accurate assessment of the renal function. You can use simple equations such as the Cockroft-Gault equation which incorporate the body weight and age.
CrCl (mL/min) = (140-age) x lean body weight (kg) x (0.85 if female)
serum creatinine (mg/dL) x 72
Most clinicians are familiar with use of methylene blue for the treatment of methemoglobinemia, as a urinary analgesic, anti-infective, and anti-spasmodic agent, or for its use in endoscopy as a gastrointestinal dye, but this compound also has a role as a rescue antidote in life threatening poisonings causing refractory shock states and other shock states.
Bottom Line:
Methylene blue should be considered when standard treatment of distributive shock fails.
Historically, there has been very limited data regarding the epidemiology of OHCA in pregnant females. Two recently-published studies tried to shed some light on the issue.
Both Maurin et al.1 and Lipowicz et al.2 looked at all-cause out-of-hospital maternal cardiac arrest (MCA) data in terms of numbers and management, in Paris and Toronto respectively, from 2009/2010 to 2014. Collectively, they found:
A few reminders from the 2015 AHA guidelines for the management of cardiac arrest in pregnancy:
Bottom Line: Although maternal cardiac arrest is relatively rare, survival in OHCA is lower than perhaps previously thought. Areas to improve include public education on the importance of bystander CPR in pregnant females, and appropriate physician adherence to PMCS recommendations, with decreased on-scene time by EMS in order to decrease time to PMCS.
Hook of hamate fracture
Often missed fracture despite classic history
A frequent athletic injury
Seen in stick sports (golf, baseball, hockey)
Typically caused by a direct blow (grounding a gold club)
https://upload.orthobullets.com/topic/6035/images/hamate_baseball.jpg
Patient presents with hypothenar pain and pain with tight gripping
https://upload.orthobullets.com/topic/6035/images/hamate_golf.jpg
Presentation may be subacute with longstanding wrist or palmer pain
Physical exam: Tender to palpation over hook of hamate
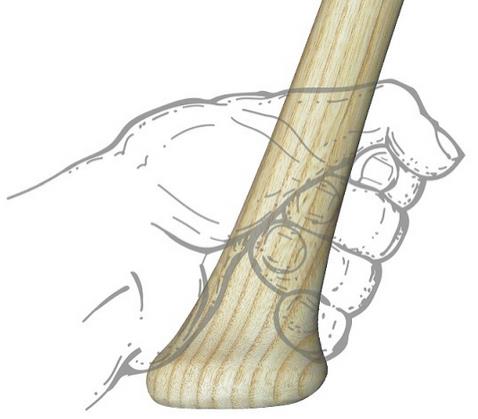
Specialized test: hook of hamate pull test
Supinated hand held in ulnar deviation. Ask patient to actively flex 4th and 5th digits against resistance at DIP.
https://www.youtube.com/watch?v=A-mjRnC1yWQ
Radiology: Consider adding carpal tunnel view to standard wrist series if diagnosis is suspected
CT sometimes needed to image the fracture
Tx: Immobilize in a short arm splint
Therapeutic use or overdose of tramadol has been associated with seizure. However, it is unknown if there are any specific predisposing factor that increases a patient’s risk of seizure after tramadol use/overdose.
In a recently published study, eighty patient data with single ingestion of tramadol were reviewed.
Risk of seizure
Conclusion
In this small study, Asian patients and patients with abuse/misuse were at higher risk of developing seizure compared to patients who overdose tramadol.
Respiratory Complications of ICIs
When caring for a patient with a laceration we often do lcoal infiltration prior to suturing but remember the benefits of regional nerve blocks
Benefits of Regional Nerve Blocks
Quick reminder of properities of common anesthetic
| Anesthetic | Onset of Action | Duration of Action | Max Dose No Epi | Max Dose With Epi |
|---|---|---|---|---|
| Lidocaine | Seconds | 1 hr | 4mg/kg | 7mg/kg |
| Bupivicaine | Seconds + | > 6 hrs | 2mg/kg | 3mg/kg |
Final reminder: There is no evidence that epinephrine causes necrosis and it can be used safely in digital blocks. Duration of action is max 90 minutes. Even individuals that have injected themselves with EpiPens into their hands have not had any long term sequelue or necrosis seen. Vast majority required no treatment at all.
Post tonsillectomy hemorrhage occurs and 0.1-3% of post tonsillectomy patient's. It occurs typically greater than 24 hours after surgery and up to 4-10 days postoperatively. A survey of otolaryngologists showed that ED management strategies for active bleeding have included direct pressure, clot suction, silver nitrate, topical epinephrine, and thrombin powder.
This article was a case study demonstrating the use of nebulized tranexamic acid (TXA) for post tonsillectomy hemorrhage in a 3-year-old patient. The patient had a copious amount of oral bleeding and had failed treatment with nebulized racemic epinephrine and direct pressure was not an option due to the patient's cooperation and small mouth. 250 mg of IV TXA was given via nebulizer with a flow rate of 8 L. Bleeding stopped 5-7 minutes after completion of the nebulizer. The patient was then taken to the OR for definitive management. No adverse effects were noticed.
TXA in the pediatric population has been shown to decrease surgical blood loss and transfusions in cardiac, spine and craniofacial surgeries. Studies have also been done in pediatric patients with diffuse alveolar hemorrhage using doses of 250 mg for children less than 25 kg and 500 mg for those who are greater than 25 kg.
Bottom line: There are case reports of nebulized TXA use in the pediatric population with no adverse outcomes noted. More research is needed.

{kind=link}
{kind=link}