Hand elevation test
https://www.youtube.com/watch?v=IO2qC5qHVFE
Bottom Line: There is no significant difference between endovascular thrombectomy and medical management for basilar artery occlusion strokes within 6 hours of symptom onset.
A recent pilot study was conducted in two centers (Mayo Clinic & Cleveland Clinic Affiliate) and aimed to evaluate if the administration of oral midodrine in early septic shock could decrease the use of IV vasopressors and decrease ICU and hospital length of stay (LOS). The study was a placebo-controlled, double blinded randomized trial.
This study enrolled:
The study did not find a statistical difference between the two groups in the use of vasopressors or ICU/Hospital LOS. However, there was a trend in the midodrine group which is suggestive of decreased vasopressor use and ICU/Hospital LOS.
It is Important to note the study was not powered to determine clinical significance. Overall the trend noted in the midodrine group should encourage further studies that are clinically powered to determine if there is a statistical difference and therefore a potential benefit to early initiation of oral midodrine in septic shock.
Vancomycin infusion reactions can manifest as pruritus and an erythematous rash of the neck, face, and torso during or after a vancomycin infusion. This is a histamine reaction caused by degranulation of mast cells and basophils, and can be caused short infusion times <60 min. It is commonly treated with antihistamines and/or a slowing of the infusion rate.
Norepinephrine is widely considered the first-line vasopressor for patients in septic shock. Vasopressin is often added to norepinephrine in patients requiring escalating doses, but when to add vasopressin, and what exactly the benefit is (as opposed to just further titrating up the norepinephrine) remain unclear. Given the limited evidence for a patient-oriented benefit and the increasing cost of vasopressin, some centers are becoming more judicious in the use of vasopressin. A systematic review in AJEM October 2021 examined the literature on early (< 6 hours of diagnosis) addition of vasopressin to the management of septic shock patients, compared to either no vasopressin or starting it after 6 hours.
Improved with early vasopressin: Need for renal replacement therapy (RRT; secondary outcome)
No difference: mortality, ICU length of stay, hospital length of stay, new onset arrhythmias
Bottom Line: When, and if, to start vasopressin in patients requiring escalating doses of norepinephrine remains controversial. Based on the prior VASST trial, many providers will start vasopressin when norepi doses reach ~ 5-15 mcg/min (approx 0.1-0.2 mcg/kg/min), but there remains limited data to support this practice, and either starting vasopressin or continuing to titrate the norepinephrine as needed are both reasonable approaches in most patients.
What is the mechanism of action of N-acetylcysteine that is used to treat acetaminophen induced liver injury/toxicity?
Refractory Anaphylaxis
During cardiac arrest, metabolic acidosis develops because of hypoxia-induced anaerobic metabolism and decreased acid excretion caused by inadequate renal perfusion. Sodium bicarbonate (SB) administration was considered as a buffer therapy to correct metabolic acidosis. However, SB has several side effects such as hypernatremia, metabolic alkalosis, hypocalcemia, hypercapnia, impairment of tissue oxygenation, intracellular acidosis, hyperosmolarity, and increased lactate production. The 2010 Pediatric Advanced Life Support (PALS) guideline stated that routine administration of SB was not recommended for cardiac arrest except in special resuscitation situations, such as hyperkalemia or certain toxidromes. An evidence update was conducted in the 2020 Pediatric Life Support (PLS) guideline and the recommendations of 2010 remain valid. This article was a systematic review and meta-analysis of observational studies of pediatric in hospital cardiac arrests. The primary outcome was the rate of survival to hospital discharge after in hospital cardiac arrests. The secondary outcomes were the 24-hour survival rate and neurological outcomes.
Bottom Line: The use of atraumatic needles is most effective in reducing the risk of post-LP headaches. These needles are easy to use and have similar rate of success as cutting needles.
RECAP: RECOVERY trial is a large, randomized, open label, adaptive trial studying different treatments on COVID-19. Most well known is the use of dexamethasone which reduced mortality by 1/3 in COVID patients requiring mechanical ventilation and by 1/5 in those requiring oxygen, with no benefit on those patients not requiring oxygen.
They recently published results in the Lancet on the use of tocilizumab.
Population:
Inclusion:
Outcomes:
Results:
Conclusion:
Both erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are highly sensitive (84-100%) for spinal infections and are observed in >80% with vertebral osteomyelitis and epidural abscesses.
ESR
Most sensitive and specific serum marker, usually elevated in both spinal epidural abscess (SEA) and vertebral osteomyelitis.
ESR was elevated in 94-100% of patients with SEA vs. only 33% of non-SEA patients
Mean ESR in patients with SEA was significantly elevated (51-77mm/hour)
CRP
Not highly specific
Less useful for acute diagnosis since CRP levels rise faster and return to baseline faster than ESR (elevated CRP seen in 87% of patients with SEA as well as in 50% of patients with spine pain not due to a SEA)
Better used as a marker of response to treatment.
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation site.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation sites.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Bottom Line: Functional neurological disorders (FND) are commonly encountered in the ED. A thorough neurological exam may reveal positive signs suggestive of FND. Early diagnosis and referral to specialists may improve outcomes.
Erythrocyte sedimentation rate (ESR) for spinal infection
Sensitive for spinal infection but not specific
Elevated ESR is observed in greater than 80% of patients with vertebral osteomyelitis and epidural abscess
ESR is the most sensitive and specific serum marker for spinal infection
Usually elevated in acute presentations of SEA and vertebral osteomyelitis
ESR was elevated in 94-100% of patients with SEA vs. only 33% of non-SEA patients
Mean ESR in patients with SEA was significantly elevated (51-77mm/hour)
Infection is unlikely in patients with an ESR less than 20 mm/h.
Incorporating ESR into an ED decision guideline may improve diagnostic delays and help distinguish patients in whom MRI may be performed on a non-emergent basis
Supplemental oxygen therapy is frequently required for patients presenting with acute respiratory distress and COPD exacerbation. Over-oxygenation can derail compensatory physiologic responses to hypoxia,1 resulting in worsening VQ mismatch and, to a lesser degree, decreases in minute ventilation, that cause worsened respiratory failure.
The 2012 DECAF (Dyspnea, Eosinopenia, Consolidation, Acidaemia, and Atrial Fibrillation) score was found to predict risk of in-hospital mortality in patients admitted with acute COPD exacerbation.2,3 Data from the DECAF study’s derivation and external validation cohorts were examined specifically to look at outcome associated with varying levels of oxygen saturation.
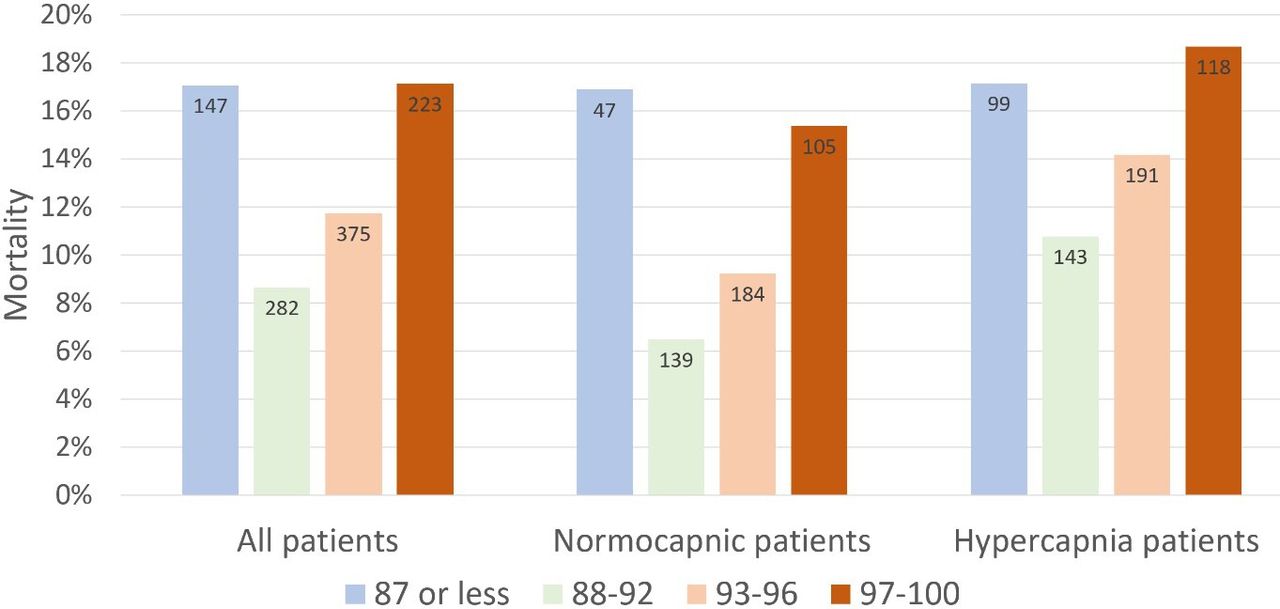
Bottom Line
In patients presenting to the ED with acute COPD exacerbation requiring oxygen supplementation, a target oxygen saturation of 88-92% is associated with the lowest in-hospital mortality, and higher oxygen saturations should be avoided independent of patients' PCO2 levels.
Bottom Line: Alteplase administration in acute ischemic stroke is associated with errors, most commonly with over-dosage of the medication.
A total of 367 patients were enrolled. Median age was 32 years Male 43%/Female 57%.
Result: There was no difference in the proportion of patients with postconcussion symptoms at 30 days. There were no differences in median change of concussion testing scores, median number of return PCP visits, median number of missed school or work days, or unplanned return ED visits within 30 days. Participants in the control group reported fewer minutes of light exercise at 7 days (30 vs 35).
Conclusion
Prescribing light exercise for acute mTBI, demonstrated no differences in recovery or health care utilization outcomes.
Extrapolating from studies in the athletic population, there may be a patient benefit for light exercise prescription.
Make sure that the patient is only exercising to their symptomatic threshold as we recommend with concussed athletes. Previous studies have shown that athletes with the highest post injury activity levels had poorer visual memory and reaction time scores than those with moderate activity levels.